![]()
![]()
![]()
ABORTION
ADDICTION: SEX ADDICTION
ADULTERY
AGING AND SEXUALITY
AIDS AND HIV INFECTION
AIDS, RELIGION, AND SEXUAL ORIENTATION
AMBISEXUALITY
ANAL SEX
ANATOMY AND PHYSIOLOGY
ANORGASMIA
ANTHROPOLOGY: INFLUENCE OF CULTURE ON SEX
APHRODISIACS AND ANAPHRODISIACS
ART: PAINTING, SCULPTURE, AND OTHER VISUAL ART
THE ARTS AND SEXUALITY
ASEXUAL REPRODUCTION
AUTOEROTICISM
Abortions in Ancient Times
Anti-Abortion Laws
Problems Caused by the Laws
Changing Policies
The Right to Life and Pro-Choice Movements
Abortion Procedures
Ethical and Political Issues
Abortion is the termination of a pregnancy before the fetus reaches viability. Traditionally, a fetus was considered viable between the 20th and 28th week of pregnancy. Abortions can be classified as spontaneous or induced. Spontaneous abortions are usually caused by faulty development of the embryo, abnormalities of the placenta, endocrine disturbances, acute infections, severe trauma, or shock. Spontaneous abortions are often called "miscarriages" to differentiate them from abortions that are induced.
Inducing abortions was widely practiced in the ancient world as a method of controlling family size. A Chinese document dated 3000 B.C.E. mentions abortions, and an Egyptian medical papyrus of 1550 B.C.E. describes an abortion technique. Plato advised that any pregnant woman over age 40 be aborted, and Aristotle argued that abortion should be used to control population growth, particularly for persons who felt an aversion to exposing unwanted offspring to the elements.
The Greeks, Romans and Egyptians all developed an extensive literature on abortive techniques. These techniques included inserting papyrus into the cervix, irritating the uterus with laurel and peppers, and using drugs believed to stimulate uterine contractions. The second-century B.C.E. Greek physician Soranus of Ephesus discussed indications for abortions, such as a contracted pelvis, and described methods of abortion, mentioning purging, carrying heavy weights, injecting olive oil into the vagina, and using drugs such as wallflower, cardamom, and brimstone. Although the document describing these methods was written by a physician, abortions in ancient times were ordinarily the work of mid-wives or they were induced by the pregnant woman herself. Throughout most of history, physicians were seldom involved in gynecological procedures; the female reproductive system was considered the domain of women.
Some ancient abortifacients have survived until modern times as folk remedies. Modern Egyptian nurses indicate that village women use mullohaya, a stiff grass used in making soup, to cause abortions - which is not unlike the ancient practice of using papyrus. Ergot, a fungus that grows on rye, was widely used in ancient times as an abortifacient wherever rye was grown. Ergot can cause severe poisoning, even death, so using it to induce abortion was not without danger. Ergotamine, a modem drug used to stimulate uterine contractions, is an alkaloid of ergot. The women of Thailand use a deep massage technique that dates back to ancient times.
Ancient Roman law and customs supported abortion, since the fetus was not considered a human being. Christianity, however, opposed both birth control and abortion and declared that abortion was murder. The early Christian writers were against abortion, although they were divided in their perception as to when the soul enters the fetus. Most did not consider abortion a sin until after quickening (i.e., the point at which the woman first feels the fetus moving), but many medieval theologians allowed abortion only for the first 40 days after conception. For example, St. Thomas Aquinas differentiated between the male fetus and the female fetus, arguing that the soul is infused into the male embryo at about 40 days after conception but it does not enter the female embryo until the 80th day. In 1869, Pope Pius IX eliminated the distinction between the early nonviable fetus and the later viable fetus by declaring that abortion at any point after conception would be considered murder for Catholics.
There were also other moves against abortion in the 19th century. English common law, which had accepted abortions as legal until quickening, was changed in 1803 when a law was passed outlawing abortion by poisoning. Later revisions strengthened the law by outlawing surgical procedures and dropping the distinction between abortions before and after quickening. In the United States, abortions were caught up in the struggle between physicians and midwives that occurred as physicians moved into the field of obstetrics and gynecology. The physicians - who argued that midwives were unsavory characters who performed abortions, so midwives and their skills should be eliminated to save the lives of women - prevailed. Laws were passed in the late 19th and early 20th centuries outlawing mid-wives in most states. Laws were also passed against abortions, with the first such statute enacted in Connecticut in 1821 outlawing abortions after quickening. A revision in 1860 made all abortions illegal. Other states followed; by the beginning of the 20th century abortion had been outlawed in all of the states, although there was some state-to-state variation in what was prohibited. Most states allowed an exception to the law, recognizing the right of physicians to perform allowed therapeutic abortions if it was essential to save the woman's life.
The U.S. anti-abortion statutes were written in an era in which there was an expanding labor market fueled by industrial expansion. In spite of the nation's need for a large work force, however, the pay for laborers was meager and the number of children who could be fed with a worker's salary was limited, so the working-class family was trapped in an irremediable situation. The options for limiting births were relatively few, with coitus interruptus, celibacy, anal intercourse, vaginal sponges, and condoms being the available choices. Since only the wealthy could afford condoms before the 1920s, unwanted pregnancies were common, and desperate women turned to illegal practitioners. Even if these practitioners were skilled, they were cut off from hospitals and physicians who could help them manage such complications as hemorrhages and infections. When antibiotics became available in the 1940s, the illegal abortionists had difficulty obtaining them for their patients because they were obtainable only with a physician's prescription. In the early 1960s, it was estimated that 8,000 therapeutic abortions were performed in the United States each year, but there were 400, 000 to 800, 000 illegal abortions each year with a high maternal mortality rate associated with them. This situation helped create a movement in the 20th century to reform abortion laws.
In addition to concern for the women involved, there was also a growing concern about untrammeled population growth. Thomas Malthus had published an essay on population growth in 1798, arguing that while population growth occurs in geometric steps, doubling every generation, food supply tends to grow only in numeric steps, so without major catastrophes, such as war or plagues, famine is inevitable. Although his theory often proved true on local levels, such as the famine in Ireland in the 19th century, the worldwide implications of his theory became apparent only in the 20th century as advances in sanitation and health allowed many people to live longer and the real dimensions of the population problem started to emerge. From 1650 to 1850, the number of people worldwide approximately doubled, from about 500 million to just over one billion, but the population doubled again in only one hundred years - from 1850 to 1950 - when it reached two billion. Since 1950, the world's population has been increasing at an even faster rate, so it will soon reach the four billion mark. Most of the world's people are now hungry, and famines have become common in many parts of the world.
The first country to legalize abortion in modem times was the Soviet Union, which, in 1920, made abortions legal as a part of its revolution. Abortions quickly became the major method of birth control. In 1936, Joseph Stalin banned abortions and the prohibition remained until his death. They were legalized again in 1955, and most of the countries then in the Soviet bloc legalized them. Poland, now free of domination from the former Union of Soviet Socialist Republics, has again instituted prohibitions against abortions. Most of the other former members of the U.S.S.R. have, however, retained legal abortions as public policy.
In 1938, Sweden passed a law allowing pregnancies to be interrupted if the woman was ill, if she had been impregnated under illegal circumstances, or if there was the possibility of a hereditary disease being transmitted to the fetus. The law was amended in 1946 to allow abortions if it could be assumed that the woman's physical or mental strength would be seriously impaired by the birth and care of the child.
Japan, in 1948, became the first country to legalize abortions for the purpose of regulating population growth. The original law legalized abortion only for women whose health might be impaired from a physical or economic standpoint, but within a few years it was broadened to allow abortion on request. The birthrate quickly dropped from 34.3 per thousand in 1947 to 16.0 per thousand by 1961. In recent years, the number of abortions has dropped somewhat with the improvements in contraceptive technology and the growing wealth of the country, but abortions are still available and selected by many women as the method of choice for controlling pregnancies. The birthrate in Japan remains low, with a virtually stable level of population growth.
The leaders of the Chinese revolution in 1949 opposed all birth control measures, but within a few years it became apparent that the rapidly increasing population was wiping out all efforts to improve the standard of living. Various measures were tried, with little success, given the degree of political upheaval at the time. By 1981, the population had reached approximately one billion people, and the People's Republic of China embarked on a comprehensive and deliberate effort to cut population growth to the zero level by the year 2000. This effort included a campaign to limit family size to one child. To accomplish this goal, contraceptives and abortions were not only offered freely, a variety of positive and negative sanctions were instituted to enforce the policy. While the "one-child" goal proved impossible to achieve and the population is not yet stable, significant strides have been made in curbing the rapid growth of the Chinese population.
U.S. policy toward abortion started changing in the 1960s. Relatively insulated from concerns about world population growth because of limitations on immigration, Americans were primarily influenced by the growing women's movement. Improved methods of contraception, including oral contraceptives, had begun to give women a sense of control over their biological destiny and as they experienced this power over the reproductive cycle they wanted more. Betty Friedan's 1963 book, The Feminine Mystique, raised the consciousness of many women and made the concept of choice over whether to reproduce respected, but to turn concept into reality required changes in the state laws.
The Model Penal Code adopted by the American Law Institute proposed that state laws be amended to allow termination of pregnancy when the physical or mental health of the woman was greatly impaired; when the infant might be born with a grave physical or mental defect; or when the pregnancy resulted from rape, incest, or other felonious intercourse, including illicit intercourse with a girl under age 16. Little action on this proposal was taken until the publicity related to Mrs. Sherri Finkbine, a Phoenix, Arizona, mother of four, illustrated the problems created by the restrictive state abortion laws. Mrs. Finkbine had taken the drug thalidomide during the first few months of her fifth pregnancy. Although the drug had not been approved by the U.S. Food and Drug Administration, and was therefore not marketed in the United States, Mr. Finkbine had obtained a bottle of thalidomide pills in Europe. Two months after Mrs. Finkbine had taken the pills, news of the deformities the pill was causing in European children was made public. Mrs. Finkbine's physician estimated that the chance her infant would be deformed was at least 50 percent, and he arranged to admit her to the hospital for a therapeutic abortion. Because Mrs. Finkbine's story reached the media, the hospital was fearful of further publicity and canceled the abortion. The Finkbines flew to Los Angeles, planning to travel to Japan for the abortion, but the Japanese counsel, also afraid of negative publicity, refused to issue them a visa. The couple then flew to Sweden, where Mrs. Finkbine had the abortion. The fetus was deformed.
This incident brought the discussion of anti-abortion laws and practices out in the open and helped to crystalize a movement for abortion law reform. An influential book by Lawrence Lader, entitled Abortion, was published in 1966. It argued that abortion was a right of privacy. Also in 1966, the National Organization for Women was established, with reproductive rights as one of its major concerns. At the same time groups of clergymen, physicians, and civil liberties advocates organized local groups, including the California Committee for Therapeutic Abortion and a similar group in New York. The National Association for the Repeal of Abortion Laws was established in 1968. These groups worked through state legislatures and the courts. As a result of their efforts, 18 states had liberalized their abortion laws by 1972, and court decisions had changed abortion privileges in three jurisdictions. In 1973, the U.S. Supreme Court heard Roe v. Wade, and struck down state prohibitions against first trimester abortions. The Court ruled that during the first three months of pregnancy the decision to abort could be made by the woman and her physician. During the second trimester the states could regulate abortion to ensure reasonable standards of care. Only in the last trimester could abortions be outlawed, but not if they were necessary to preserve the life of the woman. This decision made more restrictive state legislation illegal.
The Supreme Court's decision in Roe v. Wade brought strong reactions from those who opposed abortions on moral and religious grounds, including the leaders of the Catholic church, many fundamental Protestant churchmen, as well as individuals who felt moral repugnance to the idea of abortion. A strong backlash movement followed. Some anti-abortion activity was sponsored directly by churches, but most was coordinated by several different organizations that used the title "Right to Life." The radical fringe of these groups bombed abortion clinics or formed picket lines to block entrance to the doors of clinics. The more mainstream members of the groups worked through the political process. On the legislative front, efforts were made to weaken the right to abortion by passing restrictive state laws. Some of these laws required husband's consent; others added parental consent for minors; made public funding illegal; or added procedural requirements, such as waiting periods. Until 1986, the courts generally supported the rights of women to make decisions, but approved some of the restrictions. The situation changed in 1986, primarily because of the efforts of the Reagan administration.
President Ronald Reagan (who served as president from 1980 to 1988) made an anti-abortion stance, the most important selection criterion for federal judges and Supreme Court justices. By 1986, his policy could be felt in the judicial decision-making process because there had been enough turnover of justices to affect the decisions on this matter. President George Bush followed the same policy, making an anti-abortion stance the litmus test for judge selection. The Supreme Court has already allowed states to limit abortions and additional limitations are anticipated in some, but not all of the states.
A countermovement, using the slogan "free choice," has grown up with the National Abortion Rights Action League (NARAL) furnishing leadership. Its major focus is on abortion as a right of privacy for women. NARAL focuses its efforts primarily on the political arena.
Abortion procedures vary by the stage of fetal development. They can be separated into early abortion procedures, first trimester methods, and second trimester methods.
Early abortion procedures are carried out before the fertilized ovum reaches the uterus and attaches to its wall. They are sometimes called postcoital methods, or menstrual regulation. These procedures occur before the pregnancy tests are performed, and they are often used for rape victims. Various hormones have been used for this purpose, including diethylstilbestrol and oral contraceptives that contain estrogen and progesterone combinations. The doses of these hormones when used for early abortions are large enough to cause unpleasant side effects, such as nausea and vomiting, so their use should always be medically supervised. Oral contraceptives have not been approved for this purpose by the U.S. Food and Drug Administration, so federally funded clinics are not allowed to used this method, although it is commonly used in other countries.
The compound RU-486 is also used as a postcoital or abortifacient drug in France. It is one of a family of antiprogestins that can prevent implantation of the egg in the uterus or cause an abortion during the first nine weeks of pregnancy. It has been approved for testing by the Food and Drug Administration in the United States but is not yet available for general use.
Postcoital insertion of a copper intrauterine device (IUD) has also proven effective in regulating menses by preventing implantation of the fertilized ovum in the uterus. The IUD is inserted one to seven days following unprotected intercourse and can be left in place to prevent future pregnancies.
The third postcoital method is menstrual extraction. A canula is inserted into the uterus and a syringe or suction machine is used to extract the uterine lining. The procedure is similar to that used for a suction abortion, but has the advantage of being carried out before the pregnancy is diagnosed, which for some women causes a moral problem. Casual use of the technique is not recommended because there is risk of hemorrhage or infection.
First trimester abortions usually utilize a suction procedure that was developed in Asia, used in the U.S.S.R., and began to be used in the United States in the 1960s. It is the most common abortion procedure, although U.S. physicians combine it with curettage to make sure the uterine lining is completely removed. A dilatation and curettage is used if the pregnancy is late in the first trimester or if the physician feels there is some problem requiring the procedure. The cervix is dilated and a curette is used to scrape the uterine walls. Various techniques can be used to facilitate the dilatation of the cervix, including the insertion of laminaria (i.e., cervical tampons that swell to three or five times their original diameter when placed in a moist environment).
Second trimester abortions usually involve the insertion of a hypertonic saline solution into the amniotic sac. Prostaglandin, which stimulates uterine contractions, is sometimes used in addition to the hypertonic saline solution.
Dilatation and curettage is used for most second trimester abortions, along with the hypertonic saline solutions and prostaglandins, although sometimes a hysterotomy is done. Many second trimester abortions are done because of fetal abnormalities discovered through amniocentesis. Recently, improvements in the technique of amniocentesis make it possible to do the procedure as early as ten weeks, so there will probably be fewer second trimester abortions.
The ethical issue marking the abortion debate focuses on the rights of the fetus. Conservatives argue that the minute the sperm enters the ovum, the ovum has exactly the same moral status as a person and its rights should not be terminated by abortion. Some adherents to this argument hold that this is true even if the fetus is grossly deformed or if several eggs have been removed from the woman for purposes of in vitro fertilization. In this case, all of the fertilized eggs should be saved and as soon as possible be reintroduced into the woman for development. Since the procedure involves the use of fertility drugs that produce multiple eggs and an unlimited number of births can threaten the viability of all of the fetuses, judging how many to reintroduce is difficult.
A liberal view of abortion claims that fetuses are not human beings and have no rights. Liberals argue that abortion on request should be legal and without punishment by moral sanctions. The moderate view holds that fetuses may have some rights after they reach viability, but moderates do not worry about the rights of fertilized eggs. Moderates would allow abortions for a variety of reasons, including anything that would harm the fetus if it becomes a child, as well as for rape, incest, teenage pregnancy, and poor maternal health. Most moderates in the United States do not accept economic deprivation as a criterion for abortion although it is probably the major reason for both legal and illegal abortions in most of the Third World where food is scarce.
This broad spectrum of views can also be identified in the national surveys of public opinion. Gallup polls on abortion repeatedly indicate that the overwhelming majority of Americans favor abortion under certain circumstances, including rape, incest, unmarried minor children, genetic or intrauterine problems, or illness of the woman, but they do not favor granting women the right to abortion under all circumstances. A small group favors outlawing abortions altogether and a small group at the other end of the spectrum favors a free choice for women. Although earlier polls showed Catholics significantly more opposed to abortion, the differences between Protestants and Catholics on the issue have narrowed.
REFERENCES
Baird, R.M., and S.E. Rosenbaum. The Ethics of Abortion. Buffalo, N.Y.: Prometheus Books, 1989.
Bayles, M.D. Reproductive Ethics. Englewood Cliffs, NJ.: Prentice-Hall, 1984.
Bullough, V.L., and B. Bullough. Contraception: A Guide to
Birth Control Methods. Buffalo, N.Y.:
Prometheus Books, 1990.
Calderone, M.S. Abortion in the United States. New York: Hoeber-Harper, 1958.
Franke, L.B. The Ambivalence of Abortion. New York: Random House, 1978.
Lader, L. Abortion. Boston: Beacon Press, 1966; Also Indianapolis: Bobbs-Merrill, 1966.
McCormick, R.A. How Brave a New World: Dilemmas in Bioethics. Garden City, N.Y.: Doubleday, 1981.
Reiterman, C. Abortion and the Unwanted Child; The California Committee on Therapeutic Abortion. New York: Springer, 1971.
Rodman, H., B. Sarvis, and J.W. Bonar. The Abortion Question. New York: Columbia Univ. Press, 1987.
Bonnie Bullough
Sex addiction refers to excessive, obsessive, or compulsive sexual behavior. The term was popularized by Carnes, who describes sex addiction as an obsessional illness that transforms sex into the primary basis for a relationship or need, for which all else may be sacrificed, including family, friends, values, health, safety, and work. Support for this concept has come from many others, including Money, who feels it appropriate to classify the rituals of the paraphilias among the addictions.
According to Carnes, "sex addicts" exhibit a constellation of preferred sexual behaviors, arranged in a definite ritualized order, which are acted out in an obsessional scenario. He describes sex addicts as experiencing little or no pleasure, often feeling despair even in the midst of sex. Carnes views "sexual compulsion" as one component of an addictive cycle, which includes preoccupation (obsessions), ritualization, shame, and despair. He maintains that the addiction concept describes the phenomenon of compulsive sexual behavior because of the distinct similarity of the symptoms or behaviors to alcohol or drug addiction. The term has also been widely used in a number of publications.
Carnes posits three levels of sexual addiction. Level one is socially acceptable, tolerable, or controversial (e.g., masturbation, heterosexual relationships, pornography, strip shows, prostitution, and homosexual relationships). Level two is unacceptable (e.g., exhibitionism, voyeurism, indecent telephone calls, and indecent liberties). Level three is very unacceptable, illegal behavior (e.g., child molesting, incest, and rape).
The genesis of this concept can be traced back to the growth of Alcoholics Anonymous (AA) - a self-help group of individuals who identify themselves as alcoholics. This social movement led to recognition of alcoholism as a separate disease entity, a lifetime disease that can be controlled through treatment but not cured. Medical treatment for alcoholism embraces the 12-step model and traditions of AA. Treatment focuses on helping alcoholics both recognize that they are powerless to overcome their alcoholism and adopt a spiritual program of recovery which involves adhering to AA principles. Many of those who criticize this method of treatment endorse alternative treatment models. However, the success of AA-style treatment, based on the 12 steps and traditions, led to speculation it would also work for other "addictions."
In the 1970s, a looser definition of "addiction" developed, and it became a popular metaphor for other behaviors including those that, in excess, resembled alcohol and other drug addictions. Overeaters Anonymous (modeled after AA) was formed to help compulsive overeaters. Other groups followed, such as Narcotics Anonymous, Smokers Anonymous, Gamblers Anonymous, Spenders Anonymous, Parents Anonymous (for child-abusing parents) - and then Sex Addicts Anonymous, Sexaholics Anonymous, Sex Abusers Anonymous, and Sex and Love Anonymous.
For many sexologists and other scientists, however, the term "sex addiction" is an unfortunate misnomer because people do not become addicted to sex in the same way they become addicted to alcohol or to other drugs. In addition the term obfuscates the complex interplay of biological, social and psychological factors which causes compulsive or excessive sexual behavior. (See also Sexual Compulsion.)
REFERENCES
Carnes, P. Out of the Shadows: Understanding Sexual Addiction. Minneapolis: CompCare Publishers, 1983.
Carnes, P. Don't Call It Love: Recovery >From Sexual Addiction. Minneapolis: Bantam, 1991.
Coleman, E. Compulsive Sexual Behavior: New Concepts and Treatments. In E. Coleman, ed., John Money: A Tribute. New York: Haworth Press, 1991.
Money, J. Lovemaps: Clinical Concepts of Sexual/Erotic Health and Pathology, Paraphilia, and Gender Transpositions in Childhood, Adolescence, and Maturity. New York: Irvington Publishers, 1986.
Eli Coleman
Historical Concepts of Adultery
Modem Concepts and Patterns of Adultery
Swinging
Open Marriage
In legal, religious, and moral terminology, adultery is technically defined as sexual intercourse between a married person and a partner other than the spouse. In modern usage, adultery is a sexual activity of a married person with a nonspouse when that activity is unacceptable to the spouse. This usage distinguishes adultery as an unacceptable extramarital activity, or "cheating" behavior, from consensual extramarital sexual activities that are acknowledged and accepted by both spouses.
Civil laws in the Western world have long prohibited adultery, for example, the Code of Hammurabi, in Babylonia (c. 1790 B.C.E.); Draco, in ancient Greece (c. 620 B.C.E.); and Solon, in ancient Rome (c. 590 B.C.E.). The condemnation of adultery is even more specific in the religious traditions of the Torah, on which much of our current civil legislation is based (Exodus 20:17; Deuteronomy 5:21, 22:22-29; Leviticus 20:10). However, these ancient laws applied only to women, requiring them to limit their sexual activity to one man. Since a woman was viewed as property attached to a particular man, laws against adultery (and fornication - sexual intercourse between an unmarried man and woman) were meant to protect the property rights of husbands and fathers. However, the laws against fornication and adultery generally did not apply to married or single men and their liaisons with unattached women, such as widows, concubines, or servants.
As societal views of women and marriage have changed, so have the concept and dimensions of adultery. The idea of marriage based on romantic love is relatively new. For centuries, marriage was an economic arrangement between families. In ancient Greece, true love could exist only between two men; women were believed to be incapable of truly intense love. Although women were available for men's sexual pleasure, the Stoic tradition frowned on passion and physical love which distracted men from their higher intellectual endeavors.
Christianity rejected homosexual love but adopted the Stoic suppression of physical love. It glorified spiritual celibate love, viewing sexual love as second-rate, tolerated only because it could produce more souls for the Kingdom of Heaven.
The emergence of the concept of courtly love in southern France during the early Middle Ages set the stage for a radical change in the concept of adultery, the extension of adultery to men, and development of the idea of romantic and emotional marital fidelity. Courtly love had four roots: (1) the lusty male-dominated Teutonic values of the Franks, who viewed women as playthings for men's enjoyment; (2) a certain hedonism introduced by Eleanor of Aquitaine; (3) a new interest in and misinterpretation of Ovid's classic Roman poem The Art of Love; and (4) the growing veneration of the Virgin Mary. Medieval knights vied for the honor of their ladies in jousting tournaments and sang of their love. But these ladies were unattainable, the wives of a noble or a king. In addition, sex - the expression of physical love - was considered the mortal enemy of true, noble love. True love was not then linked with sex or with marriage, which was arranged by the family and based on property and power motives or simple practicalities.
During the Renaissance, romantic courtly love began to be imbued with sexual passion. By the 14th century, the extramarital affair was recognizable as it is known today: an illicit sexual and emotional relationship outside marriage. Prior to this, affairs were expressions of male lust without emotional involvement or interest.
The Protestant Reformation (c. 1500 C.E.) produced two social models of the affair and two views of adultery that have dominated in Western societies ever since: a pagan courtly love model and a bourgeois-puritan model.
In the Mediterranean countries and much of France, the traditional economic basis of marriage, the Catholic condemnation of divorce, and the courtly love code combined in a social pattern in which marriage remains primarily an institution designed for social benefit and to create progeny. The exuberance of sex, passion, and emotion is expressed in the extramarital relationship. This tradition has subtle customs and often-unspoken rules that regulate the relationships of married persons and their lovers or mistresses. In Latino cultures today, this tradition implies that a true man, "un hombre completo," is expected to have a wife and children, and one or more mistresses in "la casa chica" (his little homes). By implication, although it is seldom discussed among the men, Latino women are also allowed discreet extramarital relationships. In northern Europe, the aristocracy and royalty adopted this pagan-courtly love tradition. In the United States, it is found among the rich and upper class society.
In northern Europe, the early Protestants fused romantic love with marriage. They rejected the medieval Catholic ascetic view of marriage as an inferior way of life and restored the Jewish view of the importance of sexual love and family as the center of religious life and nurturance. The emerging middle-class families of northern Protestant Europe incorporated the virtues of courtly love into marriage and championed the value of conjugal love and passion, even while leaving intact traditional patriarchal values and attitudes. As the Protestants came to accept divorce, adultery and the extramarital affair became the mortal enemy of marriage and society because they were often the prelude to and cause of divorce. This bourgeois-Puritan tradition flourished through the 19th century and down to the present in American society.
Family historians believe that a major step in the evolution of love and the extramarital affair occurred during the Victorian period in America around 1880. They offer no explanation for the burst of popular literature, novels, poetry, and advice manuals that glorified romantic, marital love, and the expectation that a man or a woman should satisfy all of the partner's needs.
In the 20th century, important social changes have affected the character and incidence of adultery. Women have moved closer to the level of sexual freedom men have enjoyed for centuries as their financial independence, presence in the work force, education, legal rights, control over reproduction, mobility, socio-economic options, and personal expectations have increased. Increasing life expectancy and the reduced proportion of time wives spend in the mother and housewife roles have also strained the traditional values of sexual exclusivity.
The current concept of marital fidelity that has evolved over three thousand years of Western Judaeo-Christian culture is clearly expressed in the marriage ritual's phrase "forsaking all others until death do us part." Today, this concept includes sexual and emotional exclusivity for both spouses. However, the radical social changes mentioned above have created a growing tension in these values.
Traditionally, men have been more active extramaritally than women, but recent surveys indicate some changes. In the 1940s, Alfred Kinsey projected that at least half of all married men would some time experience extramarital sex. One in four married women under age 40 reported having had an extramarital experience. In 1970, a survey of Psychology Today readers showed that 40 percent of the husbands and 36 percent of the wives polled had had affairs. Married men and currently divorced males under age 45 in Hunt's 1974 nationwide survey reported a 47 percent rate of infidelity. A year later, married women age 40 and older, in a Tavris and Sadd survey for Redbook, reported a 39 percent frequency. In Linda Wolfe's Sexual Profile of That Cosmopolitan Girl, 69.2 percent of the married women over age 35 reported having had an extramarital experience. Both the 1975 Redbook and the 1980 Cosmopolitan surveys were of more educated, upper-class women rather than random samples. Such nonrandom surveys are hardly representative of American women in general. It may be that the increasing sexual experience of women in college, especially in college dormitories where parental control is reduced and peer pressures often prevail, predisposes more educated women to view multiple and nonexclusive relationships in a more positive framework than in the past when extramarital sex was considered a male prerogative tolerated by women. Also, many single women prefer having affairs with married men because they want a male who can provide emotional and sexual fulfillment without the pressure to take on the commitment of marriage and family.
Since most surveys of marital infidelity were done before heterosexuals became concerned about AIDS, little can be said about the incidence of adultery in recent years. However, of the persons reporting having had extramarital sex in the recent surveys that have been done, 40 to 50 percent had only one outside partner, 40 to 45 percent had two to five partners, 5 to 11 percent had between six and ten partners, and 3 to 5 percent had more than ten extramarital partners. In some respects, women now seem to be equaling or surpassing the men in extramarital relations. In one study of 200 couples in marital therapy, the affairs of husbands lasted an average of 29 months, compared with 21 months for the affairs of wives. While many studies indicate that an overwhelming majority of Americans consider adultery wrong, some psychotherapists and marital therapists see women's increasing access to sexual choices as potentially positive because it equalizes power within the marriage.
Despite our cultural values and the obvious trauma caused by adultery, marital therapists now rank adultery behind eight other factors in the breakup of marriages, such as poor communications, unrealistic expectations, and power struggles.
In 1982, Atwater found that about 25 percent of the women in her sample had discussed the possibility of having an extramarital affair with their husbands before doing so. But as long as the primary relationship is successful and for the most part satisfying, many tend to ignore that their partner is emotionally or sexually involved with another person.
As Americans become increasingly concerned about the personal and financial costs of divorce and remarriage, various adjustments to sexual exclusivity have become more visible and perhaps more commonly accepted. One form of consensual adultery based on the "togetherness" value of traditional romantic monogamy is "swinging." Swinging is recreational social-sexual sharing among consenting adults. In swinging, two or more couples mutually agree to engage in sex with each other's partners. The extent of swinging is not well documented, but surveys indicate that between two and five percent of American adults have at sometime participated in swinging.
Many couples feel that swinging is a catalyst for positive growth, a sharing activity that promotes understanding, communication, and intimacy in their relationships. They report that it helps free their relationship of routine, sex-role playing, and socially imposed inhibitions. Other writers, principally those involved in marriage counseling, report that swinging was a negative factor in the lives of those they investigated.
The North American Swing Club Association listed over 100 active, organized American swing clubs in its 1991 directory, as well as dozens of publications catering to the swing community. Annual lifestyles conventions in the South, Midwest, and West draw several thousand swingers each year.
Swinging, according to participants, involves much more than sexual activities, with the couples sharing business, emotional, and social interests. Yet, in 1971, Bartell reported that the swingers he interviewed typically limited their swinging with another couple to one or two exchanges and were thus constantly looking for new partners. Several researchers have reported that swingers are generally not liberal or highly educated. They are predominantly conservative or moderate in their politics, and far from permissive on a wide range of social and political issues. Most of the women are housewives, with few outside interests. Swingers also tend to be church-goers. Swingers, however, are not a homogeneous group but come rather from several distinct and very different subcultures.
A second form of consensual adultery, which emerged in the 1960s, reflects contemporary values of equality of the sexes within the pagan-courtly love model. The open marriage described by anthropologists Nena and George O'Neill is based on "an equal partnership between two friends" who respect each other as persons. Open marriages are flexible and allow each partner privacy and room to grow and develop, even in unexpected directions. Within a trusting relationship, the concept of an open marriage accepts the possibility of both spouses having emotionally and sexually intimate friendships within the context of a healthy primary relationship. Blumstein and Schwartz's 1983 study of American couples found that 15 percent of married couples and nearly 30 percent of the cohabiting couples reported they had sexually open relationships. Among the terms used by researchers for consensual extramarital sex based on the sexually open marriage model are intimate friendship, co-marital, or satellite relationships.
In the 1990s, as increasing numbers of married and cohabiting couples become more open about their healthy patterns of sexually open, nonexclusive relationships, some mainstream churches have established special task forces to reexamine traditional sexual values in the context of current lifestyles. Several of these task forces, particularly those of the United Presbyterian Church of the United States and the Episcopal Church, have called for reinterpretation of the traditional sexual values that uphold sexually exclusive monogamy as the sole morally acceptable lifestyle for sexually active adults and condemn all forms of premarital and extramarital sexual relations. Such reinterpretations are based on a redefinition of sexual morality and fidelity in broader terms than sexual exclusivity and heterosexual monogamy. Fidelity, in this new context, means a commitment to the covenant or contract agreed upon. Adultery, which etymologically means "polluting the relationship," is then viewed as any action or behavior that violates the couple's commitment to each other. Where couples have agreed to have a sexually open marriage, the terms "extramarital" and "adultery" are not applicable to relationships that are incorporated within the dynamics of the primary relationship.
If accepted, such reinterpretations would recognize the right of couples to redefine marital fidelity and adultery by creating their own covenant of commitment and fidelity within a liberal context. These efforts, however, are vehemently denounced and strongly opposed by the majority of church members and leaders.
In civil law, a charge of adultery was, until the 1960s, a common and widely accepted ground for granting a divorce in the United States. In some states, adultery was the only legal ground for a divorce, so that couples often concocted evidence of this felony. In 1961, Illinois adopted a consenting adult law that abolished criminal penalties for adultery and fornication. At present, few states still have laws prohibiting adultery between consenting adults, and those that do seldom, if ever, arrest or prosecute offenders.
REFERENCES
Atwater, L. The Extramarital Connection: Sex, Intimacy, and Identity. New York: Irvington, 1982.
Bartell, G. Group Sex. New York: Wyden, 1971.
Blumstein, P., and P. Schwartz. American Couples: Money, Work and Sex. New York: Pocket Books, 1983.
Hunt, M. The Natural History of Love. New York: Minerva Press, 1967.
Hunt, M. The Affair: A Portrait of Extramarital Love in Contemporary America. New York: New American Library, 1973.
Lampe, P.E. Adultery in the United States: Close Encounters of the Sixth (or Seventh) Kind. Buffalo, N.Y.: Prometheus Press, 1987.
Lawrence, R.J. The Poisoning of Eros: Sexual Values in Conflict. New York & Roanoke, Va.: Augustine Moore Press, 1989.
O'Neill, N., and G. O'Neill. Open Marriage: A New Lifestyle for Couples. New York: Evans, 1972.
Ramey, J. Intimate Relationships. Englewood Cliffs, NJ.: Prentice-Hall, 1976.
Singer, I. The Nature of Love. Vols. 1-3. Chicago: Univ. of Chicago Press, 1984a, 1984b, 1987.
Robert T. Francoeur
Since the 1960s, whenever the media have focused on changing sexuality in Western societies, adolescents and young adults have usually been spoken of. However, there has been just as much change, in attitudes and perhaps in behavior, in the sexuality of the mature - men and women in middle age (40-60) and late life (over 60). Over the past few decades, the normal life span has increased almost 20 years; in most economically advanced nations, it is now 80 or more. Thus age 40 has changed from the threshold of decline to the midpoint of life. At the same time knowledge about mature sexuality has increased enormously.
Furthermore, more people in middle and late life are now fit, active, youthful-looking, and able to avoid or control debilitating diseases. More of them are likely to think of themselves as romantic and sexual participants in life. They are also conscious of becoming a larger and more influential segment of society. When the much discussed baby boom that followed World War II has entered middle age, at the turn of the 21st century, the United States will have as many mature people as youngsters.
As the duration and quality of life increase, public and private attitudes toward mature sexuality will doubtless continue to change. In fact, it has already become difficult to imagine just how taboo the subject of later-life sexuality was when the sexual revolution of the 1960s got under way. The mass media never discussed it. No serious book on the subject appeared for general readers until the middle 1960s, and information remained sparse until the next decade. In television and films, when mature sexuality was treated at all it was treated as an aberration or a joke. Even sex researchers were slow to shed light on sex and aging. Reliable baseline data on sexual aging did not appear until the landmark work of Masters and Johnson was published, in 1966.
If one believed public discourse, one would have thought that sometime between the ages of 40 and 50 most people became asexual. It was not true, of course, but the pretense was widespread, and many people viewed the exceptions as comic or repulsive. What was considered virile or seductive at 25 was called lecherous or repulsive at 55. Many young people did not - and still do not - accept the reality that people the age of their parents and grandparents still feel sexual desire, passion, and pleasure. Even many middle-aged and old people, who knew better, felt ashamed of what today would be called normal mature sexuality.
Aging is not a unitary and consistent process. It differs from person to person, and within each individual it varies from one organ system to another. The skin, circulatory system, bones and joints, kidneys, eyes, ears, and brain may each age relatively early or late, quickly or slowly. Furthermore, environmental and nutritional factors, general fitness, and health care may all minimize or exaggerate various aging processes.
But eventually all people and organ systems do age; the reproductive and sexual systems are not exceptions. The changes are similar in many ways in women and men, but there are also significant differences. Because the male system has fewer reproductive functions to perform and is therefore less complex, its aging process is more simply defined and measured. Moreover, since the majority of men usually experience orgasm with predictable regularity from puberty until middle age, frequency of orgasm is one of several good indicators of male sexual aging.
In terms of physical capacity for erection and orgasm, most males reach the height of their sexual functioning in their late teens. A gradual decline in male steroid hormones becomes measurable by age 30 and continues throughout life. As these hormones decrease, so does the frequency of arousal and orgasm. There is also an increase in the refractory period, the interval from orgasm until erection is possible again. These changes remain slight, even imperceptible, in most men for a decade or so.
As men reach age 40, they are almost sure to have noticed some decrease in sexual function; it is rarely great or dramatic. By 50, changes are unmistakable. Although there is great individual variation, a man of 50 is likely to be about half as active sexually as he was at 20. For instance, if he normally had orgasmic sex four times a week at age 20, he probably does so about twice a week at 50.
Through the 50s and after, erection and orgasm require more time than in the past. Ejaculation becomes less forceful, and the refractory period lengthens. However, there is no subjective decline in pleasure. For the great majority of men, sex remains an important and gratifying part of life.
Sexual desire and response continue to slow with the continuing decline in hormone levels in the 70s and 80s, but in the majority of men they never disappear. The urgency of desire declines, and erection and orgasm require more stimulation but the capacity for sexual activity and pleasure remains. Although they may produce fewer sperm, some men remain fertile and capable of fathering children into advanced old age.
Most women's sexual frequency is more variable than men's; it tends to lack an independent, long-term regularity. It depends less on hormonal regulation and more on personality, social learning, and the quality of sexual relationships. The capacities for desire, arousal, and orgasm do not, as in men, peak in late adolescence or early in young adulthood. In fact, many women's sexual expression does not peak until their 30s or even later. However, a decline in female hormones does begin to affect women's ability to conceive and carry a healthy fetus to term. There is individual variation, but some changes in reproductive potential are usually evident by age 40.
A dramatic and important event in female sexual aging is the menopause, usually between the ages of 45 and 55 (or earlier as a result of radical hysterectomy or other pelvic surgery). A fall in relative estrogen levels brings an end to ovulation, menstruation, and fertility. In the past, some people assumed that menopause meant the end not only of fertility but also of desire and pleasure, and the discomforts of this "change of life" were viewed virtually as an illness.
A minority of women do experience severe discomfort at menopause; often it can be reduced medically. For the majority, the discomforts are transient and not debilitating, and menopause does not affect sexual interest or pleasure. Some women actually find that it brings heightened or renewed eroticism, perhaps because of freedom from worry over unwanted pregnancies.
In women, as in men, hormonal decline does make some sexual tissues and responses less vigorous. The vaginal wall starts becoming thinner and less elastic after menopause. From the 50s on, arousal and orgasm may take longer than in the past. Vaginal lubrication, which signals arousal, becomes scantier. Prolonged or unaccustomed genital stimulation may irritate the vagina and clitoris, especially in women whose sex activity is infrequent. However, these changes need not interfere with a pleasurable sex life; for many women, systemic or local hormone therapy combats aging changes.
Other aging processes come to both men and women - changes in skin tone, body contours, body image, and overall strength and endurance. They can directly or indirectly reduce sexual frequency or pleasure. However, a list of aging changes can suggest a less satisfying picture than exists in reality.
In recent years, studies have shown just how tenacious a force sex is in middle and late life. The great majority of people over 50 are still sexually active, mostly through coitus, oral-genital intercourse, and masturbation. Although sex is less frequent and eventually less intense than in youth, it may become more tender, more satisfying, and less inhibited.
A large-scale study by Brecher found that most happily married older people still find sex an important part of their relationships; two-thirds of the unmarried over age 70 are sexually active. A smaller, more recent study of people from 80 to 102 years of age found that half of them said sex was at least as interesting and important to them as in the past.
For the sexually active mature person, sex may not only reflect health but promote health. The sexual system, like other organ systems, stays more fit if it is used. Masters and Johnson found that postmenopausal women who remain regularly active (through coitus, masturbation, or otherwise) show less vaginal thinning and more vaginal lubrication than the sexually inactive. They are less likely to feel discomfort when they engage in sex than are the infrequently active. In short, in sex as in most physical and mental activities, one tends to "use it or lose it."
Other health issues are important in sexual aging. From midlife on, major and minor illnesses can take a sexual toll; so can many widely used medications. Decreased mobility or endurance can be a hindrance. However, Brecher's survey found that even severe health problems affect many people's sex lives only modestly. Greater awareness of this by older people and their health-care providers could further reduce the impact of sexual aging.
It is true that some people retreat from sex in middle or late life. Some were never very interested. Some always associated sex with shame, guilt, fear, or inner conflict. Menopause, slower arousal, or illness in themselves or their partners gives them a welcome excuse to bow out. Some people retreat from sex because they feel wounded or humiliated by aging or by a partner's lack of sexual interest. Entrenched relationship conflicts, power struggles, or sexual habituation makes some couples drift into a pattern of mutual avoidance that assumes a stubborn life of its own. Such problems may yield to skillful counseling at any age.
Some of these people say they are content with a life lacking sexual pleasure or a sexual relationship. There is no arguing with personal choice or with individual definitions of happiness. But most people - old or young, male or female, straight or gay - find that an important part of health and happiness is a lasting, loving sexual relationship.
Other people actually blossom sexually in midlife or even later. With child rearing and the peak of work and financial pressures behind them, they have more time for their relationships. Emotional maturity may have taught them more healthy self-assertion along with more empathy and flexibility toward others. The tendency toward sexual adversary relationships, so common in adolescence and early adulthood, often dwindles. It may not matter that the urgency of desire has declined; from late middle age on, some people are satisfied with pleasurable sex even if it does not always culminate in orgasm. Greater self-acceptance and acceptance of others can reduce the need to give a performance, in others' eyes or one's own.
It is no surprise, then, that many mature people say their sex lives are warmer and more rewarding than before. Some women lose the sexual inhibitions and conflicts of youth; some men learn a less demanding, more empathic appreciation of their partners, evoking a warmer response. The fading of old emotional power struggles can allow greater trust, affection, and relaxed pleasure.
Even habituation, eventually a major or minor problem in many or most mateships, need not interfere seriously with sex. When psychiatrist Olga Knopf was in her 80s, she wrote that people who have spent a lifetime together "see each other not only as they are but also retain an image of how the other looked in the early days, like a double exposure that hides to a large extent the telltale signs of the passage of time."
Some of time's worst effects on mature sexuality come from depression, loneliness, and isolation. This is a growing problem as life is extended and patterns of marriage and divorce change. More and more people find themselves single in middle or late life. This is a more difficult problem for women, because they live longer than men; with the passage of years, their chances of finding new partners decline more rapidly than men's. Moreover, for older people of both sexes, lack of a regular partner tends to reduce erotic desire and activity. Finding a new partner often restores lost sexual interest.
Unfortunately, many mature people were raised to see their own sexuality as unseemly or repellent. Even if they were not, they may meet strong emotional resistance to their sexuality in reactions of friends, children, grandchildren, health-care workers, and sometimes potential partners. Many people still believe that sexuality, and sexuality education, are for kids. They do not see sex as a healthy and healthful part of the entire life cycle.
Therefore, it remains necessary to remind people that we never outgrow the need for emotional intimacy and physical pleasure, the desire to touch and be touched. For people of any age, sexuality can be a tonic, a personal affirmation, a tie to other people and to life. It can bring heightened confidence and a strengthened sense of competence. As more people live longer, old and young will both benefit from appreciating how great an antidote sexuality is for the forces that can rob later life of health, joy, and meaning.
REFERENCES
Brecher, E. M. Love, Sex and Aging. Boston: Little, Brown, 1984.
Bretschneider, J. G., and N. L. McCoy. Sexual Interest and Behavior in Healthy 80- to 102-Year-Olds. journal of Sex Research, Vol. 17 (1988), pp. 109-29.
Butler, R., and M. Lewis. Midlife Love Life. New York: Harper & Row, 1988.
Doress, P. D., and D. L. Siegal. Ourselves, Growing Older. New York: Simon & Schuster, 1987.
Knopf, O. Successful Aging. New York: Knopf, 1975.
Masters, W. H., and V. E. Johnson. Human Sexual Response. Boston: Little, Brown, 1966.
Weinstein, E., and E. Rosen. Sexuality Counseling: Issues and Implications. Pacific Grove, Calif.: Brooks/Cole, 1988.
Winn, R. L., and N. Newton. Sexuality in Aging: A Study of 106 Cultures. Archives of Sexual Behavior, Vol. 11 (1982), pp. 283-98.
Zeiss, A.M. Expectations for the Effects of Aging on Sexuality in Parents and Average Married Couples. Journal of Sex Research, Vol. 18 (1982), pp. 47-57.
Arno Karlen
Prevalence
Testing
Research and Treatment
Psychosocial Aspects of AIDS
Treatment Groups
Other Issues of Economics and of Public Policy
AIDS and Politics
Legal and Ethical Issues
A Cross-Cultural View
AIDS and the Future
AIDS (acquired immune deficiency syndrome) is caused by infection with the human immunodeficiency virus, commonly called HIV. HIV enters the body in two main ways: (1) through bodily fluids (e.g., blood or semen) in anal or vaginal intercourse, or through oral genital contact; or (2) through sharing drug needles with infected persons. It can also be transmitted to infants either in utero or during birth. Occasionally, it has been transmitted through breast milk. One may also become infected by receiving HIV-infected blood or certain blood products, as do surgical patients, accident victims, and hemophiliacs. In rare instances, transmission has occurred through receiving bone grafts or organ transplants from HIV-infected donors.
AIDS is a progressive destruction of the immune system leading to opportunistic infections that would not be successful in attacking those with healthy immune systems. HIV infection is an "equal opportunity" disorder, striking young or old; male or female; homosexual, bisexual, or heterosexual; rich or poor; Anglo or person of color. Former Surgeon General of the United States C. Everett Koop stressed this in his 1988 report Understanding AIDS: " [W] ho you are has nothing to do with whether you are in danger of being infected.... What matters is what you do." But Koop also stated that AIDS is not transmitted by donating blood, from everyday casual contact, from insect bites (including those of mosquitoes), nor from tears, saliva, sweat, nonbloody urine or feces, nor from kissing.
AIDS was first identified in the United States in 1981, among homosexual and bisexual men. Since then it has spread to virtually all segments of the population. The various infected groups represent shifting percentages of known AIDS cases and of those infected with HIV. HIV infection ordinarily leads to AIDS and to its resultant opportunistic and life-threatening infections (e.g., Kaposi's sarcoma and pneumocystis carinii). Also included are central nervous system effects of HIV infection, primarily in individuals already symptomatic.
By 1991, the Centers for Disease Control stated that nearly 196,000 cases of AIDS had been reported in the United States and that 65 percent of those diagnosed had died of AIDS-related diseases. The percentages of cases were divided among groups as follows: 58.6 percent homosexual or bisexual males; 22.4 percent heterosexual intravenous drug users; 6.5 percent male homosexual and bisexual intravenous drug users; 5.7 percent heterosexuals; 3.7 percent "undetermined"; 2.2 percent recipients of transfusions; and 0.8 percent hemophiliacs. At least 40 cases of infection of health care workers contracted by blood from infected patients were reported, with more such cases suspected. Apparently, only one case of transmission had occurred by 1992 from caretaker to patients. In that case, a Florida dentist was reported to have infected five of his patients while engaging in procedures such as tooth extraction. It is absolutely crucial to recognize that these percentages have varied over time and will no doubt shift again. For example, a sharp escalation has occurred in the number of heterosexual cases, including those among women, since the Centers for Disease Control first began keeping statistics on AIDS incidence and fatalities. Undoubtedly also, many cases have gone unrecognized or unreported for various reasons. A compelling example is that many physicians fail to think of, or to test for, HIV infection in women with such symptoms as recurrent yeast infections and pelvic inflammatory disease, sometimes indicative of AIDS. Already there is evidence of increased infection through heterosexual transmission, including teenagers, a group of great concern because of its complacent "it can't happen to me" attitude. Heartening perhaps, a Los Angeles Times poll, taken shortly after a major sports figure, Earvin "Magic" Johnson, announced he had tested positive for HIV in the fall of 1991, sampled 1, 709 adult Americans nationwide. It found that 23 percent of those polled responded that they had changed their sexual behavior after hearing this news. On a more pessimistic note, however, Eleanor Singer, a senior research scholar at Columbia University and a polling specialist, observed that "when you compare [actual] behavior and response... the likelihood is... that very little change has taken place."
At about the same time, the Geneva-based World Health Organization reported that at least eight million cases of HIV infection were officially reported worldwide.
Among those who should consider being tested for exposure to HIV, some experts say, are people who have multiple sex partners and those whose partner's HIV status is not known; those who have unprotected sex outside of a stable monogamous relationship extending back perhaps, at least 15 years; all others who have unprotected sex with partners; and finally, all intravenous (IV) drug users who share needles. It might be more accurate and inclusive to say anyone who could possibly be at risk should be tested.
To determine HIV status, the most widely used test as of 1992 was the ELISA (enzyme-linked immunoabsorbent assay). While there are some false negatives or positives, the ELISA test was incorrect in less than one percent of samples. To be doubly sure, a further test, called the Western blot test, can be used after the ELISA. While even this two-step testing process is not perfect, it is more accurate than most medical screening procedures.
HIV infection is believed by some to have originated in Central Africa. A widely accepted theory is that it was transmitted from monkeys infected with a different strain of virus to humans (a not unusual cross-species occurrence for viral transmission). The African green monkeys that test positive for the presence of the similar strain, unlike humans, do not show evidence of compromised immune systems, so far as can now be determined. Put simply, in humans the virus attacks, among other cells, the T cells that play a dominant role in helping the body ward off infections. A compelling reason for the especial virulence of HIV infection is that it invades the core of the cell, where it becomes part of the cell's genetic structure.
As the body attempts to fight other infections, the immune system eventually weakens until it becomes vulnerable to assorted "opportunistic" infections that it cannot overcome. HIV infection may proceed rapidly to a diagnosis of AIDS, but more typically it has a markedly long latency in which infected persons may feel quite healthy. At present, the median latency appears to be about ten years. With the passage of time since the recognition of HIV, and with the invention of increasingly effective treatments, this latency may be far longer, perhaps even as long as one's (otherwise usual) life span.
By 1992, the most commonly used drug to combat AIDS was the antiviral drug zidovudine, commonly known as AZT. There has been considerable disagreement over when, in the course of HIV infection, treatment should begin. Increasingly, physicians and medical researchers lean toward earlier treatment with AZT, as well as with other drugs that enhance the immune system's performance. While AZT may produce adverse side effects, including anemia, more serious side effects are experienced primarily by those in more advanced stages of AIDS. In October 1991, federal health officials announced that they had approved use of another AIDS antiviral drug, DDI (i.e., dideoxyinosine and didanosine). This drug provides alternative treatment for persons with AIDS for whom the adverse effects of AZT are too devastating. In addition, it may be used by those for whom AZT has been (or has become) ineffective. It is not unusual for AZT to lose effectiveness after two or three years of treatment, so the development of alternative drug therapies remains a top priority.
Such antiviral drugs are of special importance because they directly attack the HIV infection rather than the resultant opportunistic infections and cancers that attack the body because of immune system damage. As with AZT, DDI suppresses HIV infection in previously uninfected "helper" cells. An advantage of DDI over AZT is that it apparently increases the number of these T4 helper cells. While it was not yet known whether DDI prolongs survival, or whether it might make possible still longer latency before opportunistic infections develop, its approval by the U.S. Food and Drug Administration was a landmark in that it signaled a willingness (under heavy lobbying from interested citizens and from health professionals) to be more proactive and timely in responding to those who urgently need immediate treatment.
Meanwhile, research and testing of possible effective vaccines against HIV continues, with the prediction by some of the possible discovery of an effective vaccine by the year 2000. In addition to the scientific challenges presented by the complexities of this viral infection, other constraints placed on research are due to outright hostility toward certain target groups leading "disapproved" lifestyles. Reactionaries both inside the government and among the public are not only judgmental, but also carry the misperception that only "they" get AIDS, and when they do, "they deserve it" (a position hard to maintain as people from all groups get AIDS). Also, it is difficult to compete for research funding in a mismanaged and overstressed economy, no matter what the need. It is a tribute to the organization and activism of the gay community especially, that AIDS has received the attention it has. There is always the danger of public apathy stopping the momentum for funding of AIDS research and treatment if such activists do not remain energized or if the burden of pressing for action is not taken up by many others who are likewise increasingly at risk.
Medical aspects of AIDS have understandably received considerable attention in the scientific community. Since HIV was first identified, there has been a growing awareness of the need for psychosocial research to assist in understanding and treating HIV infection. This includes research into the psychosocial factors affecting whether an individual seeks testing or treatment in the first place. It also includes finding better means of helping individuals and their loved ones deal with the emotional, physical, and economic consequences of AIDS, as well as counseling the "worried well." Also, research must deal with optimally assisting health care providers and the public to cope with the consequences of HIV infection, which touches all members of the community, whether directly or indirectly.
A 1991 survey by the American Medical Association (AMA) found that nearly a third of primary care physicians surveyed do not assume they have a responsibility to treat persons with AIDS. These 2,000 internists and general and family practitioners show an attitude that is decidedly contrary to medical ethics. To some degree, this was related in self-reports to disapproval of homosexuals and of IV drug users. Those who conducted the study attributed the doctors' positions to bias against the groups thus far hardest hit by the epidemic. One physician commented that homosexuals are "a threat to many of our basic social institutions." Respondents specifically evidenced homophobia and discomfort with IV drug users. Half of these physicians said they would not work with AIDS patients if they had a choice. In an accompanying editorial, AMA officials stated: "[P]ractitioners are not free to ignore [their ethical duties] simply because it entails a small degree of personal risk" or because they do not like their patients. "Nor can physicians expect less medically sophisticated members of the public or government officials to react to health care crisis with reason and compassion when they themselves do not demonstrate these characteristics."
As to what role the psychological profession might play in dealing with the AIDS epidemic (in a 1984 interview, a few years after the first AIDS-related opportunistic infections were recorded), San Francisco Director of Health Mervyn Silverman was quoted as reflecting a far more enlightened view than the majority of physicians in the above 1991 AMA survey:
I think because AIDS has impacts far beyond the medical issues, it is most important for individuals who are going to be working with people with AIDS... to first of all understand the disease and try to have an understanding of what mental processes are associated with it. The mental health concerns include not only fear of death, but also [of] ostracism, a whole number of reactions from peers, and the reaction of the general community. We need very understanding people in the mental health field, very understanding [psychotherapists] who comprehend the political and social ramifications and who understand the disease [syndrome].Loved ones too, are affected by the medical, economic, and mental health challenges accompanying AIDS. They also experience anxiety and distress and can benefit greatly from support, both from members of the medical community and from other health care professionals.
Another category of people requiring support and assistance is the health care professionals who work intensively with AIDS patients and those who are HIV positive. These AIDS "experts" are at considerable risk of "burnout" and stress-related illnesses, both physical and psychological. Growing close to patients and to their loved ones while watching their diseases slide in what seems an inevitable downhill progression can be extremely debilitating for overworked professionals. This is especially so because many of their peers avoid participating in AIDS-related care. The workers need a periodic "time off' and the opportunity to participate in group sessions so that they can share events and feelings about their work and personal experiences as caregivers.
The "worried well" may also require support and empathy from others. Numerous individuals, even those not objectively at risk, are anxious or even phobic about AIDS. When well-meaning experts, politicians, or members of the media conjure up images of the war against the "plague" of AIDS, they evoke counterproductive feelings of pessimism and distress, even among optimistic persons. These themes have persisted throughout the course of the "AIDS experience."
Although all persons with AIDS are vulnerable to serious infections, some face unique challenges as well.
The term "pediatric AIDS" is an unfortunate choice. It can be misused by some, who are homophobic or otherwise judgmental, to distinguish HIV-infected infants and children from other HIV-positive persons. This makes possible a (false) distinction between "the innocent," deserving of care and public concern, and "the guilty," whose HIV status is the result of purported sinful behavior, thus of little concern to the self-righteous. Having said this, it is true that infants with AIDS have their own needs as to treatment modalities.
For older children with AIDS or HIV-positive status, the Centers for Disease Control guidelines recommend that the children lead normal lives insofar as possible. It is convinced that the psychosocial and educational benefits of the classroom experience outweigh the risk of infection from other children.
In general, AIDS has gone hand-in-hand with negative community reactions to persons known or presumed to be HIV infected. This has included cases of stigmatization in the school environment, where HIV infected children are ostracized at a time when interaction with peers is crucial for their social and emotional development. This is especially distressing in light of the (typically) relatively long period in which hemophiliacs (which includes most of these children) are asymptomatic. While such behavior is not only cruel and irrational but also illegal, some families have found that stigmatization and ostracism are so painful that it is preferable to undergo the emotional upheaval and expense of relocating.
Not surprisingly, research to date indicates that adolescents as a group are not only often ill-informed about cautionary guidelines that may prevent HIV infection, but also frequently feel "immune from AIDS." Although adolescence is, historically, a life stage in which teenagers usually feel immortal, they are prone to many high-risk behaviors, including drug use and sexual experimentation in a country where influential church leaders and political right-wing minorities vigorously oppose the availability of sex information or condom distribution to young people. Just as the United States generally experiences the highest rate of unplanned teen pregnancy, abortion, and teenage sexually transmitted diseases (STDs) in the Western world, so too it can expect a sharp escalation in HIV infection among teens in the future, unless the "just say no" position is abandoned. The Centers for Disease Control reports that the number of adolescent AIDS cases has been rising steadily since 1985. Physicians and educators are especially alarmed because studies indicate that this age group is becoming sexually active at ever-younger ages. National data indicate that the highest rates of syphilis and chlamydia, as well as of gonorrhea ("markers" for estimating future HIV infection), show that females ages 10 to 14, and 15 to 19 have the highest rates of STDs compared with older age groups. For minority adolescents, the incidence is even higher. Given the typically long latency from HIV infection to a diagnosis of AIDS, there is indeed cause for alarm.
For heterosexual men and women, it may be projected that HIV transmissions will continue to rise as more individuals are infected by partners who have engaged in high-risk sexual behaviors in the past. Thus far, the government and public health agencies have been especially negligent in addressing the issue of women and AIDS. Short sightedness and the mis-perception that AIDS is a disease associated only with prostitution and intravenous drug use among women have unfortunately provided a rationale for neglect of women among judgmental political conservatives. Future educational and other AIDS-related programs must recognize that AIDS is a health issue for all and certainly not an issue that should be approached from a morally judgmental position. Further, vigorous outreach to racial and ethnic groups, whose culture or religion usurps women's reproductive rights, must be accompanied with sensitivity to cultural differences.
Homosexual and bisexual males are particularly burdened in coping with AIDS because of frequent homophobia, even among physicians. In too many cases, these men must cope not only with the debilitating physical and psychological effects of AIDS, but also with the isolation imposed by unsympathetic relatives and acquaintances and with the stresses of trying to conceal their sexual orientation from others. Given mistreatment of companions by some families of deceased persons with AIDS, it is imperative that persons with HIV-related infections legally set forth their wishes to prevent such injustices in an uncertain future. Men living alone are especially likely to find themselves totally isolated, depending exclusively on health care professionals for human contact.
Intravenous drug users are a singular population in that they are involved in the spread of HIV infection not only through sharing needles and syringes, but also through sexual transmission, and transmission from mother to child. Drug users are also a frequently stigmatized group, often poor, without shelter or support, and dependent on an overloaded public health system whose representatives may be both disapproving, uncaring, or both. In this highly individualistic society, there is little compassion for those who are not self-sufficient and certainly none for those who engage in a disapproved lifestyle.
The reluctance of policy makers (based on the belief that it will encourage drug abuse) to endorse the distribution of free bleach, alcohol, and clean needles and syringes compounds the escalation of IV-related infection. "Street-wise" outreach programs are required to teach IV drug users how to sterilize their equipment and to provide basic AIDS information. It is laudable that such outreach programs exist in San Francisco and in New York City, though most other major cities have shown considerable reluctance to initiate them. The challenge of reaching out to those in the drug community is exacerbated by the fact that death occurs frequently for IV drug users, and did so long before the emergence of AIDS.
The problems of minorities, such as African-Americans and Latinos, are compounded by their over representation among inner-city IV drug users; by lack of access to social services for the poorer segments of these populations; by high levels of unemployment and discrimination; and by cultural or religious pressures discouraging contraceptive use. Additionally, African-American and Latino children are overrepresented in the public school systems, which are not known generally for vigorously promoting sex education or for making available to students contraceptive information and/or condoms. Early onset of sexual activity and the absence of adequate sex information contribute greatly to the high rates of STDs in general among inner-city youths. Unless the situation improves, undoubtedly these groups will continue to acquire HIV infection disproportionate to their representation in the total population. A serious threat is posed by the spread of crack cocaine use among drug users, including inner-city teens as well as adults. (Crack is a relatively inexpensive and readily available street drug, which is often smoked as an accompaniment to sexual activity.)
Finally, both the disabled and the severely mentally ill are often overlooked by the medical and health care communities, by the educational system, and to some extent, by AIDS-related researchers. Both economic and moral constraints operate within these groups. Health care professionals and families of the disabled or mentally ill are strongly inclined to treat those thus afflicted as asexual. Indeed many are repulsed when confronted with the sexuality of these people.
For the transient or homeless, who include some of the two groups just mentioned, it has been difficult to assess, much less to help curb, the spread of HIV infection they are experiencing. There has long been an urgent need to find the best ways to educate and assist these individuals to stop behaviors that increase their risk of becoming HIV infected. Many of them are, sometimes understandably, suspicious of those who attempt to help them. They avoid others because they do not want to be stigmatized or because they wish for privacy.
Policy makers at the federal, state and local levels have been justly criticized for concentrating on prevention of infection to the detriment of already infected persons who either need care immediately or will in the future. The gay community, perhaps because of insufficient or untimely official response, stands as a model of coordinated volunteer effort for all citizens.
When the government does act, too often it is with counter productive and sometimes unconstitutional efforts to control infected individuals (as through talk of quarantine of HIV-infected persons). AIDS may be used as an excuse to push a conservative agenda over such issues as availability of contraceptive information to teenagers, legalization of drug use, and women's reproductive rights. A conservative political climate at the time that HIV infection was discovered until the present has allowed the federal government to refuse to make AIDS a top priority. This has extended from reluctance to fully fund research to the refusal to fund education and public health care programs directed at persons with AIDS. It has extended also to neglect of their caretakers and their loved ones. Assorted economic, legal, and moral issues have also been neglected. These issues include drug dissemination and testing, health insurance needs, confidentiality for those who are HIV infected, and the rights of infected people in the work place and as U.S. citizens.
The need for improved health care benefits and for related services is acutely felt among virtually all citizens today, but even more so among persons with AIDS. As a result of the vacuum left by the lack of specific government programs to deal with AIDS, much of the responsibility has been left to reluctant and sometimes negligent private health care insurers, to city budgets, to state Medicaid programs, and, perhaps most regrettably, to infected individuals and their loved ones, friends, and volunteers.
Perhaps the most successful response at the local level has been that of San Francisco, with a diversity of both funded and organized volunteer efforts directed to meeting the needs of persons with AIDS and organized services directed at general community outreach.
The need for public education to have a more active role in dissemination not only of AIDS information, but also of contraceptive and overall sex education, was addressed earlier. In addition, the efforts of public schools to provide facilities for HIV testing and for condom distribution in a confidential setting have been woefully inadequate, where they exist at all.
Training in cultural sensitivity and in factual information about AIDS must be addressed for public officials and others who may have contact with HIV-infected individuals in their daily work. Law enforcement personnel particularly must be prohibited from behaving prejudicially toward persons with AIDS or toward those who are suspected to be HIV-infected.
Despite all that has been learned about HIV infection and its transmission, and about AIDS-related diseases, each time a medical professional visibly overreacts to the threat of infection by, as in one case, resigning from surgical practice, a powerful and destructive message is sent to the general public and to others who look to such professionals as role models. Policies addressing health care professionals especially require an assumption of some risk in dealing with most infectious diseases, as has been the case through much of medical history until the recent discovery of antibiotics and vaccines. Some physicians have not yet acknowledged the historically accepted commitment of medicine to the acceptance of risk, however remote, in the course of patient care. These groups, as are all service providers, are rightly held to a standard of service even under difficult circumstances. It is both unethical and unprofessional for well-compensated workers to refuse to deal with HIV-positive individuals. This is especially true for those on the "front lines," as are members of the health professions.
Addressing the regulation of health care insurers, both federal and state governments have been for the most part over protective of the insurance industry, especially since the pro-big-business decade of the 1980s. Richard Mohr, in Gay Community News, wrote eloquently in 1986 of the plight of persons with AIDS when faced with an intransigent insurance industry. Little has occurred since that time to negate his observation: "Insurance companies come to the AIDS crisis with dirty hands.... They make their money from the statistical norm, and so they suppose that is also the moral norm. They mistakenly think they are promoting something normal, something American, when they have discriminated against gays." This statement might be applied more broadly to all who share positive HIV status, and even to those who live in Zip Code areas reflecting heavy concentrations of groups significantly affected by AIDS in the past.
Turning to AIDS in the work place, a 1988 Wall Street Journal article reported that to that date only five percent of U.S. employers had developed an AIDS policy. This was attributed to concerns about image, client relationships, or the appearance of endorsing homosexuality or IV drug use. More companies have taken positive action since then, notably IBM, which mailed copies of a Centers for Disease Control AIDS brochure to all of its U.S. employees. The mailing included a letter from IBM's medical director, who wrote, "IBMers affected by AIDS will be encouraged to work as long as they are able, and their privacy will be respected." The issue of AIDS in the work place was still not uniformly resolved by the end of 1992. AIDS-related income losses in the work place have wide implications that extend to the nation's economy, including possible social security deficits and bankruptcy of some pension plans.
AIDS emerged as a public health issue at a time of conservative national government. President Ronald Reagan established an agenda based on diminished federal responsibility in addressing social needs. A pro-business, elitist philosophy created much uncertainty regarding the health needs and other social requirements of those who are vulnerable. While the government has strengthened national leadership since that time, it continues to stop short of much public support of those who are HIV infected. So long as religious and political conservatives maintain a disproportionate hold on the national agenda, there is reason for serious concern. In an attempt to move toward a comprehensive national strategy for addressing AIDS, the Presidential Commission that issued The Human Immunodeficiency Virus Epidemic Report in 1988 recommended:
1. replacement of the obsolete term "AIDS" (Acquired Immunodeficiency Syndrome) with the term "HIV infection"In its report, the Commission blamed societal and governmental apathy for the failure to develop a national strategy and estimated that fatalities from HIV-related diseases would grow to 350,000 early in the 1990s. The report stated, "Our nation's leaders have not done well." The White House "has rarely broken its silence" on AIDS and Congress "has often failed to provide adequate funding for AIDS programs" [despite developing some important AIDS legislation]. As of 1992, a number of these recommendations had not been formally addressed by the federal government.2. early diagnosis of HIV infection
3. increased testing to facilitate understanding of the incidence and prevalence of HIV infection
4. treatment of HIV infection as a disability under federal and state law [s]
5. stronger legal protection of the privacy of HIV-infected persons
6. immediate implementation of preventive measures, such as confidential partner notification
7. prevention and treatment of intravenous drug abuse
8. implementation of drug and alcohol abuse education programs
9. establishment of federal and state scholarship and loan programs to encourage nurses to serve in areas of high HIV impact
10. extension and expansion of the National Health Service Corps
11. aggressive biomedical research
12. more equitable and cost-effective financing of care for HIV-infected persons
13. addressing the concerns of health care workers
14. federal assurance of the safety of the blood supply
15. undertaking all reasonable efforts to avoid transfusion of another person's blood
16. development and implementation of education programs
17. addressing the problem of HIV-infected "boarder babies" (i.e., those left in the hospital nursery)
18. addressing the problem of high-risk adolescents
19. addressing ethical issues raised by the HIV epidemic
20. support and encouragement of international efforts to combat the spread of HIV infection.
Mandatory testing for AIDS is not recommended by the Centers for Disease Control. It is questionable on several legal grounds as well. It constitutes a physical intrusion that challenges the Fourth Amendment, especially for an infection not easily communicable compared with other infectious diseases. Further, there is the question whether the government or other agencies should have access to personal information gathered during mandatory testing. Instead, the Centers for Disease Control stresses that testing be offered anonymously insofar as possible. Enforcement of confidentiality contributes greatly to encouraging participation in voluntary testing. Current public health practice is to protect the privacy of the HIV-infected individual and to maintain the strict confidentiality of health records. The issue of confidential testing becomes even more compelling as new life-prolonging drugs are discovered. The threat to civil rights and the abuses that might occur among insurers, in the work place and elsewhere, make mandatory testing a very questionable policy. In addition, given the length of time that may pass before HIV antibodies appear in blood samples after infection, initial false negative results may cause tremendous harm to the well-being of the individual and of possible partners. Also, testing is no guarantee for the safety of caretakers, who may be falsely assured about HIV status during the early stages of infection.
Addressing research involving HIV-positive persons, such studies are subject to the Department of Health and Human Services Regulations for Protection of Human Subjects. In addition, the Department sets forth three ethical considerations that must be observed in conducting AIDS-related research:
1. There must be fairness in the distribution of both risks and benefits of research.Issues of personal ethics and AIDS include the question of trust between partners. A study by Susan Cochran and Vicki Mays, published in 1990 in The New England Journal of Medicine, cautions that significant percentages of both males and females lie, or would lie, about past sexual experience and HIV status to prospective partners. From these results, one may conclude that condom use in sexual activity is a wise choice, barring a decision to remain abstinent.2. Possible benefits of the research must be maximized and possible harms minimized.
3. The rights of research subjects to make choices based on informed judgments must be respected.
As noted above, the World Health Organization reported in late 1991 that at least eight million adults worldwide had been reported as HIV- positive. Some estimates of all HIV infections, reported and unreported, may extend to more than ten million worldwide, including six million in Africa alone, and one million in the Caribbean and South America, added to one to one and one-half million in the United States, with the remainder in Asia and Europe.
In Africa, heterosexual transmission is quite prevalent. Several studies characterize African persons with AIDS as having had multiple partners, as among the better-educated, as urban dwellers, having sexual contacts while traveling a good deal, and as typically having a history of other STDs.
In Haiti and the Dominican Republic, HIV infection is prevalent among heterosexuals. There is also significant evidence of infection among infants and children.
In Japan, it was not until mid-1986 that the government mandated screening of all donated blood for HIV antibodies. Japan has had to overcome a long-standing policy of not informing patients with life-threatening diseases of their health status. This policy is now fast-changing in light of the advent of AIDS.
HIV in Latin America has received less worldwide attention than has the infection in either the United States or Africa. While AIDS appeared relatively later in Latin America, the rate of infection is growing alarmingly in such countries as Mexico and Brazil. Cases are in the thousands in these two countries. While homosexual transmission predominated early on, it seems likely that the social pressure to lead an apparently heterosexual life style will lead to further increases in heterosexual transmission as time goes on.
The World Health Organization predicted in late 1991 that 40 million people would be HIV infected by the 21st century. While research on, and the development of, new drugs continue, many experts doubt there will ever be a cure.
Of considerable concern is a 1990 finding by the American Civil Liberties Union (ACLU) that AIDS-related discrimination was rising in the United States and that it was directed not only at those who are infected but at their families and caregivers as well. One expert concluded: "This report suggests that we are far less reasonable and compassionate than we... care to believe." Discrimination also extended to employment, housing, insurance, delivery of government benefits, and access to health care from private dentists and other providers. The ACLU recommended further efforts to educate health care workers about their legal and ethical responsibilities, expanded legal services, and increased training of lawyers in legal issues relating to AIDS. It also recommended more vigorous enforcement of antidiscrimination laws and greater regulation of the insurance industry so as to "create a system in which all Americans are assured access to health care."
REFERENCES
Bayer, R. Private Acts, Social Consequences. New York: Free Press, 1989.
Bullough, V. L. AIDS: Avoiding Witch Hunts. SIECUS Report, Vol. 14 (Jan. 1986), pp. 1-3.
Cohen, P. T., M.A. Sande, and P.A. Volberding, eds. The AIDS Knowledge Base. Waltham, Mass.: The Medical Publishing Group, 1990.
Corless, I. B., and M. Pittman-Lindeman, eds. AIDS: Principles, Practices, and Politics. New York: Hemisphere Publishing, 1989.
Grossman, M. Pediatric AIDS. In I. B. Corless and M. Pittman-Lindeman, eds., AIDS: Principles, Practices, and Politics, op. cit.
McKenzie, M. F., ed. The AIDS Reader: Social, Political, Ethical Issues. New York: Meridian, 1991.
Masters, W., V. Johnson, and R. Kolodny. Crisis: Heterosexual Behavior in the Age of AIDS. New York: Grove Press, 1988.
Pierce, C., and D. VanDeVeer, eds. AIDS: Ethics and Public Policy. Belmont, Calif: Wadsworth Publishing, 1988.
Scott, J., and S. Harris. The Times Poll: Johnson Case Raises AIDS Concerns If Not Caution. Los Angeles Times (Nov. 28, 1991), pp. 1, 32, 42.
Shilts, R. And The Band Played On: Politics, People, and the AIDS Epidemic. New York: St. Martin's Press, 1987.
Sontag, S. AIDS and Its Metaphors. New York: Farrar, Straus & Giroux, 1988.
Sprecher, Susan. The Impact of the Threat of AIDS on Heterosexual Dating Relationships. Journal of Psychology and Human Sexuality, Vol. 3 (1990), pp. 3-23.
Veronica Diehl Elias
Scripture and Tradition
Historically, organized religion has responded to societal crises according to the teachings and tradition of the particular faith. When faced with matters of the general health of the community, religious institutions have characteristically responded with compassion and pastoral concern. On the one hand, the AIDS (acquired immune deficiency syndrome) crisis presents an occasion for supportive concern by religious groups; on the other hand, it raises questions and challenges organized religion to examine teachings about illness and morality. Since AIDS can be sexually transmitted, religious institutions have been required to examine their attitudes and teachings about sexual morality, sexual orientation, and sexual behavior. The AIDS crisis also has required church groups to reexamine their teachings on homosexuality.
This entry examines how organized religion in the Judaeo-Christian tradition interfaces with the religious response to AIDS and the issue of sexual orientation. This discussion explores traditional religious attitudes toward homosexuality and current interpretations and responses by church groups to gay AIDS victims.
The plight of the gay AIDS patient (who, for purposes of this discussion, has acquired the virus through sexual contact) has called attention to the impact that a religious belief system has on a person suffering with a disease. Persons afflicted with AIDS, a life-threatening illness, can respond only within the psychological and spiritual frameworks of their total life experience. That religious system impacts on the person's sense of self-worth and feelings of well-being. Most gay persons are usually aware that many, if not most, organized mainstream religions share a negative and often condemnatory stance on homosexuality. It is the internalization of the negative aspects of religious teachings about homosexuality that makes the spiritual dilemma of the AIDS victim at times so acute. Some of those teachings and traditions are examined below.
A number of organized religious groups confronted their traditional attitudes about homosexuality in the late 1980s and early 1990s as part of their general conventions and official proclamations. Most of them were negative in content. The Methodist Church reaffirmed its position that homosexual behavior is "incompatible with Christian teaching." The Southern Baptist Convention saw homosexuality as "an abomination in the eyes of God." The General Convention of the Episcopal Church was unable to reach a consensus on many sexual issues, including homosexuality, and remained "non-judgmental."
Since at least 1975, the Roman Catholic Church has opposed homosexual behavior as "intrinsically disordered and in no case to be approved of." In a 1986 letter to the bishops of the Catholic church, the Vatican Congregation for the Doctrine of the Faith reminded Catholic bishops of the traditional teaching against homosexual behavior. Despite a pastoral call for compassion, little change is expected in church teaching. In the letter, Biblical interpretations that Scripture "has nothing to say on the subject of homosexuality" are viewed as "gravely erroneous." In fact, the document states that it "is likewise essential to recognize that the Scriptures are not properly understood when they are interpreted in a way which contradicts the Church's living tradition. To be correct, the interpretation of Scripture must be in substantial accord with that tradition."
This is the same Vatican document that directs Catholic bishops to exclude proactive gay groups from using church facilities for their meetings or worship, since "no authentic pastoral program will include organizations in which homosexual persons associate with each other without clearly stating that homosexual activity is immoral." Such a stance is the church's right to proclaim, and it has placed a burden on sexually active Catholic gay men and women by excluding them from the use of church facilities. They often have moved their place of worship to more supportive non-Catholic churches.
Catholic theologians, including feminist reformers, are also criticizing traditional Church views on homosexuality. In a book commissioned by the Catholic Theological Society (however, not officially approved) Father Anthony Kosnick and his colleagues reassessed Catholic sexual ethics that focus on procreation, natural law, and specific sexual acts: "Wholesome human sexuality is that which fosters a creative growth towards integration. Destructive sexuality results in personal frustration and interpersonal alienation." This view allows for a holistic approach to human sexuality that is more relationship-oriented than arts-centered.
It is within the mainstream Protestant churches that some range of opinion on sexual issues exists and some balance is noticed. For example, the New York Times reported in 1988 that the United Church of Canada had voted to admit gay men and women in the clergy in its statement that "all persons regardless of their sexual orientation, who profess faith in Jesus Christ and obedience to him, are welcome to become members of the United Church. All members of the Church are eligible to be considered for the ministry."
Another example of acceptance of gay sexual orientation is reflected in a statement by the English Quakers: "[O]ne should no more deplore 'homosexuality' than left-handedness.... Homosexual affection can be as selfless as heterosexual affection and therefore we cannot see that it is in some way morally worse."
Judaism has long affirmed sexuality as a good gift from God and does not emphasize the body-soul dualism that underlies Christian tradition. In brief, Orthodox Judaism opposes homosexuality, while Conservative and Reformed Jews are more questioning of traditional condemnation of homosexuality. Gay synagogues have existed in the United States since the 1970s.
Ethicist James Nelson, who has written eloquently on sexuality and homosexuality, summarizes the views of different churches on homosexuality into four major categories: (1) rejecting and punitive, (2) rejecting and nonpunitive, (3) qualified acceptance, and (4) full acceptance. Nelson asserts that only full acceptance of homosexual orientation can lead to the view that same-sexed relationships can express a divine humanizing intention. He feels that any lesser view places the gay person in a bind that accepts the person but condemns the behavior. Accepting the person but condemning the behavior is what the Catholic Church and many Protestant denominations have been doing.
The review of denominational teachings on homosexuality is a reflection of the way Judaeo-Christian tradition has interpreted and understood homosexuality for generations. It is the primarily condemnatory view of homosexual behavior that has made the AIDS issue so prominent a task for church groups to face. A great part of church tradition rests on the accepted interpretation of biblical references to homosexuality. It is here that more literal interpretation of the words of Scripture can be cited to condemn homosexual behavior. Over the generations, both gay and nongay people have shared a more literal interpretation of biblical reference to homosexuality along with the consequent prejudices that attain to it.
Modern biblical scholarship has allowed a wider interpretation and understanding of Scripture relating to homosexuality. These modem approaches are not without critics, and there is genuine disagreement about the meaning of scriptural texts. However, by departing from the literalist interpretation, the Scriptures can be viewed in terms of what was being said within the context of biblical times. For example, some modern authors agree that homosexuality as a sexual orientation is not addressed in the Bible. One view is that biblical injunctions cannot be made into eternal truths independent of historical and cultural contexts. Therefore, it is essential to first understand the meaning as seen by the writers in their own concrete situation.
For scriptural references to have meaning today, some feel that the biblical statement must be consonant with the larger, major theological and ethical judgments that lie at the heart not only of Scripture but of the historical church. In addition, the context today must be reasonably similar to the context of the statement at the time it was written. Following this line of reasoning, for example, even if St. Paul's judgments in his epistles are eternally valid, they remain valid only against what he opposed. Biblical references, then, cannot be generalized without risk of violating the integrity of the text. Thus, the question for some scholars is not whether the Bible is authoritative but whether it addresses the issue involved (i.e., current understanding of homosexual orientation and behavior).
These principles can be applied to understanding the basic biblical texts, which are relatively few, that have been used as examples to condemn homosexuality. The Old Testament has three references traditionally linked with homosexuality: the Sodom and Gomorrah passage in Genesis 19 and the two denunciations in Leviticus (18:23, 20:13). Principal New Testament references are St. Paul's letters: Romans 1:24-27, I Corinthians 6:9-10; and Timothy 1:8-11. The New Testament provides no words of Jesus on homosexuality.
No reference to, or understanding of, homosexuality as a sexual orientation is mentioned in biblical passages. Rather, specific same-sex acts are at issue. The Scriptures were written at a time when heterosexual nature was considered "natural" and the need for procreation in a male-dominated society was paramount.
A closer look at traditional biblical passages illustrates the point. A more modem interpretation of the destruction of Sodom and Gomorrah (Genesis 19) is that of a punishment for the violation of standards of social justice and hospitality. The prospects of violent gang rape or intercourse with a divine messenger - rather than a prohibition of homosexual orientation or consenting behavior between adults - can be seen as being condemned. The two references in Leviticus are part of the Holiness Code which includes many other prohibitions on diet and behavior, many of which are ignored in common observance today. Taken as a whole, the purpose of the Code, as seen by some scholars today, was to keep the Jews pure and separate from the practices of pagan influences and practices.
As for St. Paul's comments about same-sex behavior, current scholarship suggests that he may have been reacting against same-sex acts expressing idolatry and undertaken in lust. Pederasty was common among the Romans in St. Paul's time and often involved young male prostitutes. When this is considered, his words appear to address the unnaturalness of an adult heterosexual male engaging in homosexual acts.
As mentioned before, the concept of sexual orientation was foreign in biblical times. Loving, caring, and committed same-sex relationships are not dealt with in Scripture, although there are examples of strongly bonded same-sex relationships. Placed within the context of the times, both the Old and New Testaments were written in cultures battling foreign influences that threatened a religious way of life. Procreation was for the Jews essential for survival; exclusive homosexuality was nonprocreative. Pagan cult practices threatened Jewish purity. New Testament writers were influenced by Greek philosophy and avoided contamination by sexual excesses ascribed to Greek and Roman practices.
In the following early Christian centuries, the foundation of Greek dualism eventually became a part of Christian theology in the development of the conflict between the body and the spirit. The writings of Sts. Augustine and Jerome, and their negative view of man's sexual nature, had great influence even then (and still does today). Later, St. Thomas Aquinas's arguments based on Natural Law became the foundation for traditional Catholic teachings on sexual matters. As mentioned, literalist interpretation of Scripture also serves as the foundation for current negative views on homosexual orientation and behavior by many church groups. Such are the seeds of the current and traditional attitudes about homosexuality which, when linked causatively with the development of AIDS, have inflicted so much pain on both victims of AIDS and their religious denominations.
Whatever present or future pronouncements contain about the attitude toward homosexuality and AIDS, few gay AIDS victims and certainly not all clergy or committed believers are aware of both the history of the religious teachings on homosexuality and the more recent scriptural and theological research. What remains is that an important part of the struggle and spiritual dilemma of the gay AIDS victim may be neglected. The religious response of the AIDS patient is important in the overall response to the illness. It provides both an opportunity and a challenge to face and understand long-standing conflicts regarding sexual orientation and behavior. If accepted, this opportunity and challenge can lead to greater personal comfort in religious support, on the one hand. On the other hand, it can result in a feeling of even deeper alienation not only because the denomination condemns the behavior that perhaps led to fatal illness, but also because those with AIDS may feel personally condemned because of their nature.
The initial religious response of a person who contracts AIDS through homosexual activity is usually a recognition that they must confront their homosexuality in the context of their earlier religious experiences. This response frequently means that the AIDS victim has rationalized his sexual identity, lived with the cognitive and spiritual dissonance, and far too often has accepted the role of a social outcast. The frequent result is that the gay AIDS patient experiences a resurgence of his or her own homophobia. While this is understandable, the situation calls for pastoral sensitivity by church groups, family, and friends.
The term "spiritual" is important here, since it suggests a difference between the formulation of earlier church-related experiences of organized religion and a more universal experience of mankind that is not necessarily associated with a particular denomination or doctrinal system. The dilemma of the AIDS victim is indeed spiritual, even if the person professes no formal religious orientation. The person faces a journey that goes beyond religion to roots that give a sense of meaning and belonging. This sense of achieving a feeling of grounding is even more important for the gay AIDS patient who feels particularly alienated from organized religion. The journey must still be undertaken.
Terms such as "sinner" and "unnatural" can over the years result in feelings of guilt and even social withdrawal. What is important for spiritual healing is embracing a positive attitude toward the body and sexuality. The holistic approach emphasized by Nelson can help a person integrate his or her sexuality and spirituality in a satisfying way; he contends that too much time has been spent defending and justifying sexual orientation.
Today, some denominations are providing support to their gay members within a religious context: Integrity (Episcopalian), Dignity (Catholic), Reformation (Lutheran), Affirmation (Mormon). The Fellowship of Metropolitan Community Churches was founded by a gay minister to serve the gay community.
The pastoral support by various religious denominations for AIDS victims has been compassionate, merciful, and consistent with religious teachings of the responsibility toward the sick and needy. It is the emotionally laden issue of sexual orientation and sexual behavior as they relate to the incidence of AIDS that remains a challenge for all and a cause for further study and dialogue.
REFERENCES
Congregation for the Doctrine of the Faith. Letter to the Bishops of the Catholic Church on the Pastoral Care of Homosexual Persons. In J. Gramick and P. Furey, eds. The Vatican and Homosexuality. New York: Crossroad, 1988.
Fortuanato, J. AIDS, The Spiritual Dilemma. San Francisco: Harper & Row, 1987.
Gramick, J., and P. Furey, eds. The Vatican and Homosexuality, op. cit.
Kosnick, A., et al. Human Sexuality: New Directions in American Catholic Thought. New York: Paulist Press, 1977.
Nelson, J. Embodiment: An Approach to Sexuality and Christian Theology. Minneapolis: Augsburg Publishing House, 1978.
Nelson, J. Religious and Moral Issues in Working With Homosexual Clients. In J. Gonsiorek, ed., Homosexuality and Psychotherapy. New York: Haworth Press, 1982.
Nelson, J. Sexuality Issues in American Religious Groups: An Update. Marriage and Family Review (1983), Vol. 6:3/4, pp. 35-46.
Scroggs, R. The New Testament and Homosexuality. Philadelphia: Fortress Press, 1983.
Julian W. Slowinski
The term "ambisexuality" was first published by Erwin J. Haeberle in 1978 in his textbook "The Sex Atlas" as an alternative, more precise term for "bisexuality". Masters and Johnson adopted the term in 1979, but used it to describe men and women who had frequent sexual interaction with members of both genders but who reported absolutely no preference for one or the other. Sexual interaction was viewed as simply a matter of sexual release. They defined the term ambisexual therefore as "a man or woman who unreservedly enjoys, solicits, or responds to overt sexual opportunity with equal ease and interest regardless of the sex of the partners, and who, as a sexually mature individual, has never evidenced interest in a continuing relationship."
The terms ambisexual and bisexual are used to describe the relationship between heterosexuality and homosexuality. Alfred C. Kinsey produced a scale that classifies human psychosexual and behavioral response into seven categories ranging from exclusively heterosexual (the Kinsey 0) to exclusively homosexual (the Kinsey 6). The numbers 1 through 5 represent a ratio between homosexual and heterosexual behavior.
The criteria established by Masters and Johnson for the identification of an ambisexual are (1) that the individual express no preference in terms of sexual partner selection either through personal history or by subjective description, (2) that he or she [is] currently living an uncommitted ambisexual lifestyle and [has] never as an adult evidenced any interest in a continuing relationship, and (3) that the behavior of the man or woman in question could be rated close to 3 in Kinseys rating scale (this would be the midpoint on the scale). Fantasy patterns were not considered a part of Masters and Johnsons definition. After a national search of about eight months in 1968, only six men and six women were found who fit the criteria. They said that their sexual preference was "that of the partner of the moment." These numbers are too small to allow generalizations about ambisexuality as defined by Masters and Johnson. The term "ambisexuality" is often equated with the term "bisexuality," a designation that has been used in many ways that have very little precise meaning. The original Kinsey scale was established using as criteria both overt sexual behavior and purely pschychic reations (desire, sexual attraction, fantasy). In other words, Kinsey rated behavior in the widest possible sense (overt and covert), but he did not rate persons. Indeed, he avoided and disapproved of using terms like homosexual or heterosexual to describe persons. Kinseys scale represents a continuum, and an individual's rating may change over time. That is, his behavior may be rated 2 at one time and 5 at another; therefore, the rating should not be viewed as being final or as predicting future behavior.
Given the indefinite character of the Kinsey 1 through 5 ratings, perhaps ambisexuality rather than bisexuality is the better term to use. Ambisexuality would recognize the continuum and be defined as "a persons ability to eroticise both genders under some circumstances," since equal attraction to males and females is virtually nonexistent.*
*This entry was corrected by the online editor E. J. Haeberle
REFERENCES
Blumstein, P., and P. Schwartz. Bisexuality in Men. Urban Life, Vol. 5, No. 3 (1976), pp. 339-358.
Blumstein, P., Bisexuality: Some Social Psychological Issues Journal of Social Issues, Vol. 33, No. 2 (1977), pp. 30-45.
Haeberle, E. J. The Sex Atlas. The Seabury Press, New York 1978.
Masters, W. H., and Virginia E. Johnson. Homosexuality in Perspective. Boston: Little, Brown, 1979.
Masters, W. H., Virginia E. Johnson, and R. C. Kolodny. Human Sexuality (3rd ed.). Glenview, Ill.: Scott, Foresman, 1988.
Reinisch, J. M. The Kinsey Institute New Report on Sex. New York: St. Martin's Press, 1990.
James D. Haynes
The anus is the opening to the lower end of the digestive tract and is surrounded by two sets of muscles called the anal sphincters. A person can learn to control the contractions of the outer sphincter. The anal opening leads into the short anal canal and the larger rectum. Perineal muscles support the area around the anus and are in close contact with the bulb of the penis in the male and the outer portion of the vagina in the female. All of these tissues are well supplied with blood vessels and nerves. The inner third of the anal canal is less sensitive to touch than the outer two-thirds, but is more sensitive to pressure. The rectum is a curved tube about eight or nine inches long and has the capacity, like the anus, to expand.
One form of anal intercourse involves the insertion of an object into the anus. The object may be a finger, penis, dildo, or other objects. Some people engage in "fisting," which is the insertion of the hand and sometimes part of the forearm into the anus and rectum. The pleasure derived from penetration of the anus is both physical and psychological. Psychological satisfaction may be derived by the feelings of dominance and submission produced in the participants. Fantasy is often an important factor in achieving satisfaction. The stimulation of the nerve endings in the tissues and muscles, the bulb of the penis, and connections to the vagina; the feeling of fullness in the rectum; and the rubbing against the prostate gland in the male create physical pleasure in many people. Various objects may be used to stimulate the anus during masturbation. This may be done by one person using the object (often a dildo), or by mutual masturbation during group sex in which a partner inserts the object. One person may also insert a finger or fingers into the anus while rubbing the penis or clitoris. Some people insert "butt plugs" into their anus and wear them during the day to prolong a feeling of sexual pleasure. A butt plug is similar to a dildo, but may be shorter and thicker in diameter. It is usually composed of flexible rubber and may be molded into various shapes. It is held in place with straps that attach to other clothing or wrap around the waist.
The anus is also used sexually in ways that do not involve penetration. The rubbing of the external sphincter and the flexing of the muscle during masturbation are common. Anilingus (i.e., the kissing, licking, sucking, and insertion of the tongue into the anus) is not uncommon.
Contrary to popular belief, anal sex is not an activity exclusive to the male homosexual, nor is it the activity most often practiced by him. Although statistics on this subject are suspect, some investigators report that 47 percent of predominantly heterosexual men and 61 percent of the women have tried anal intercourse. Thirteen percent of married couples reported having anal intercourse at least once a month. Approximately 37 percent of both men and women have practiced oral-anal contact. A study of homosexual men revealed that only 20 percent had experience as inserter and 18 percent as insertee.
Anal sex has been known since records of human sexual activity have been kept. Depending on the culture, or even on the time of the evolution of the culture, the practice has been tolerated, accepted, expected, or condemned. Definite roles were sometimes assigned to the participants. For example, it was common in many cultures for the insertor to be an older man teaching the insertee, a young man. In other cultures, the participants were of equal status and alternated roles. It was considered unusual by the people in those cultures if such relationships did not exist. Anal intercourse was sometimes used as an act of dominance over a conquered enemy or to exert superiority over women. It has also been used as a means of birth control and as an alternative to vaginal intercourse during menstruation. In some instances, partners in a heterosexual relationship engage in anal penetration because they find it more satisfying. Women have also used dildos and other objects to penetrate their male and/or female partners. In some societies, men assumed the roles of women (the berdache) and held honored places within the society.
In some cultures, men would insert fingers during certain rituals, or wear butt plugs while meditating. Anal sex has often had mystical significance. The berdache was often thought to have magical powers. In China, anal intercourse with a wife was permitted because it was thought that by doing so the husband could get the essence of yin. Even gods of ancient Egypt, Seth and Horus, practiced anal sex as a means of establishing dominance.
Anal sex was often punished by hanging, burning, decapitation, and mutilation in societies where it was not accepted. Participants were sometimes banished or publicly disgraced. The Judaeo-Christian ethic began to exert a very negative influence on the acceptance of anal sex. Words such as "buggery" or "sodomy" became strongly pejorative. The fear of being considered homosexual lent a strong negative connotation to anal sex, although the insertor could retain his masculinity more easily than the insertee. The idea that the anus was somehow dirty or disgusting led to further denial of anal sex.
Certain precautions must be followed if practicing anal sex, but it is not as dangerous as often thought. Penetration should be done slowly and carefully by a penis or a soft rubber object that has no sharp edges or points. Anything inserted into the anus should be well covered by a water-based lubricant. The pain of insertion can be overcome by the insertee by practicing relaxation techniques, and, if done properly, there should be no tearing of the soft anal tissues. Positioning of the inserted object is important because of the curve of the rectum. Fisting is an activity that should be practiced, if at all, with great care. Few people are capable of relaxing enough to accommodate something as big as a fist in their anus, and there is real danger of damage to the delicate rectal tissues.
Disease-causing organisms can be transmitted during anal sex. These include syphilis, gonorrhea, nongonococcal urethritis, herpes, anal warts, hepatitis, and various organisms that cause intestinal infections. They can also be transmitted from anus to mouth or to vagina if a penis or dildo is not thoroughly cleaned before it is inserted into those openings. Since about 1979, AIDS has produced a new danger for those who practice anal sex. The causative organism, HIV, is most often transmitted sexually through anal intercourse. Because the disease is so deadly, special consideration must be given to anal penetration by a penis. The penis should be covered by a condom that contains a spermicide and should be well lubricated with a water-based lubricant. Great care should be taken that there be no tears in the anal tissue or in the penis or condom. Precautions should be taken to ensure that blood-to-blood or semen-to-blood mixing not take place. Anilingus (rimming) is another activity that presents an avenue for transmission of disease-causing organisms. At least one study reports that there is an association between the frequency of anal intercourse and the occurrence of certain kinds of cancer of the rectum.
REFERENCES
Bullough, V. L. Sexual Variance in Society and History. New York: Wiley-Interscience, 1976.
Morin, Jack. Anal Pleasure and Health (2nd ed.). Burlingame: Down There Press, 1986.
James D. Haynes
Male Anatomy and Physiology
Female Anatomy
In simple terms, the male reproductive system consists of a pair of testes that produce sperm and hormones, a network of ducts designed to transport the sperm from the testes to other points on their journey, a variety of glands that produce semen, and the penis. The testes are egg-shaped structures located in the scrotum, a sacklike structure that hangs outside the male body at the base of the penis. Physiologically, the testes are located in the scrotum because it is cooler than the abdominal cavity, where the higher temperature would (as it does in the undescended testicles) destroy the sperm.
The average testicle measures one to one and a half inches in length, and each manufactures and secretes the hormone testosterone as well as small amounts of estrogen, the female hormone, and androsterone, another male hormone. Within the scrotum, each testis (or testicle) is suspended at the end of what is called the spermatic cord. The cord contains blood vessels, nerves, a sperm duct called the vas deferens, and a thin muscle called the cremaster muscle, which encircles each testicle and raises it closer to the body in response to fear, cold, anger, and sexual arousal. Each testicle contains hundreds of structures called seminiferous tubules where sperm is produced. If these tightly coiled tubules were stretched out, they would extend one to three feet in length. At the back portion of each testis is the epididymis, a storage and excretory unit for sperm. Its smooth walls contract when ejaculation takes place, moving the sperm out into the connecting tube or vas deferens. The two vas deferens (both of which are severed when a male is sterilized) run along the testicle, up into the abdominal cavity, and around the bladder before emptying into the ejaculatory ducts, which enter the prostate gland. It is here that sperm from each testicle is combined with fluid from the prostate gland to produce the semen that enters the urethra. The urethra in the male serves double duty, functioning as a carrier not only of the semen but also of urine.
The sexual process starts with arousal, which causes the penis to change from its flaccid resting state to an erect condition called tumescence. This is possible because the penis includes two cylinders, corpora cavernosa, made up of spongy tissue. Cells in this tissue have spaces between them, and arousal causes the space to fill with blood. With further stimulation of the tumescent penis from intercourse or other sexual activity, ejaculation occurs and the semen is expelled from the urethra.
The ejaculate of the average male contains from 200 million to 400 million sperm, but the sperm account for only about 1 percent of the total volume of the semen. In addition to fluid from the epididymis, the seminal vesicles, and the prostate gland, semen also contains secretions from the Cowper's glands. These glands flank the urethra and empty into it through tiny ducts. It is believed that the secretion of the glands helps neutralize the acidity of the urine in the urethra, thus making possible the survival and mobility of the sperm. Cowper's glands also contain a small number of sperm (proportionately smaller, though the number is still in the millions), and this preejaculatory fluid can impregnate a woman even if the man withdraws before ejaculation takes place. (See illustrations of the male reproductive system.)
The female reproductive system is not as visible as that of the male. It consists of a pair of ovaries, two Fallopian tubes, a uterus, cervix, vagina, and vulva. The ovaries are almond-shaped organs located in the pelvic cavity, nestled in the curve of the Fallopian tubes. Ovaries are the female counterparts of testes and develop from similar tissue during the fetal differentiation between male and female, a process that takes place early in the development of the fetus. Both ovaries and testes produce reproductive cells (eggs in the case of ovaries) and both secrete hormones. The ovaries primarily produce estrogen and progesterone, although they also secrete small amounts of masculinizing hormones, including testosterone. At birth, the ovaries contain between 230,000 and 400,000 ovarian follicles, clusters of nutrient- and hormone-secreting cells with an immature egg in the center. Only 400 to 500 of these eggs, or ova, will be released from their follicles, usually one each month, from puberty to menopause.
Each Fallopian tube, which is connected to the uterus, is about four inches long. The end of the Fallopian tube nearest the ovary is not connected to it directly. Instead, it has a funnel-like opening tube with fingerlike edges (called fimbria) that help the ovum enter the tube through a process not yet fully understood. Inside the tube are hairlike structures known as cilia that sway in the direction of the uterus and guide the ovum. The tube also contracts to help push the ovum along. Fertilization, if it takes place, occurs in the Fallopian tubes near the entrance closest to the ovaries.
The uterus resembles an upside-down pear and is held suspended in the pelvic cavity by a series of ligaments. It is located between the bladder and the rectum. It shifts and contracts in response to pregnancy, the filling or emptying of the bladder or rectum, and sexual intercourse. The walls are partially composed of smooth muscles; it is the contraction of these muscles that occurs during orgasm, childbirth, and menstruation. The contractions during menstruation are more pronounced (and painful) in some women than in others.
At the lower end of the uterus is the cervix, which extends into the vagina. It has an opening or mouth (referred to as the os) through which sperm can enter the uterus and travel up to the Fallopian tubes. It is also the opening through which childbirth takes place. The cervix has glands that excrete varying amounts of mucus. This mucus plugs the entrance to the cervix and forms a barrier against the entry of sperm during most of the menstrual cycle. During ovulation, the mucus is thinner and more permeable.
The vagina is a thin-walled muscular tube that extends from the uterus to the external opening, the introitus. The walls contain many blood vessels that become engorged with blood during sexual excitement and during childbirth. Under congestion or pressure from the blood, small amounts of fluid are squeezed through the cell walls. This fluid acts as a lubricant during sexual intercourse and delivery. The process is very similar to that which leads to arousal in the male.
"Vulva" is the term usually given to the external genitalia of the female, including the mons pubis, the outer and inner lips (labia), the clitoris, the introitus or vaginal opening, and the urinary opening (entrance to the urethra). The mons pubis is a cushion of fatty tissue covering the pubic bone. It is covered with pubic hair and has a large number of touch receptors. The labia majora (outer lips) cover the external genitalia; they merge with the rest of the body skin at the back at the perineum, the area between the anus and the labia, and in the front they come together a small distance above the clitoris. The labia majora are similar to the scrotum in the male (in male-to-female transsexual operations, the scrotum is used to form the labia) and have fewer touch and pressure receptors than the mons. The labia minora (inner lips) are the inner covering of the entrance to the vagina. They are thinner than the outer labia and have no hair on them. They enclose both the vaginal and the urethral openings as well as the ducts of the Bartholin glands, which produce a small amount of mucus. The clitoris is composed of two small erectile, cavernous bodies enclosed in a fibrous membrane and ending in a glans, an exposed head homologous to the penile glans. It is one of the most erotically sensitive parts of the female body and is permeated with both pressure and sensory receptors.
The female reproductive system undergoes two physiological processes, menstruation and childbirth, which are exclusive to the female. All other physiological processes are shared in common between the sexes. Unlike male fertility, which is relatively constant during the reproductive years, female fertility is cyclical and involved with the menstrual cycle. (See illustrations for details of female reproductive anatomy.) For physiological changes during menstruation, childbirth, and orgasm see the discussions elsewhere in this encyclopedia.
Vern L. Bullough
Introduction
Orgasmic Response
Preorgasmia or Primary Anorgasmia
Secondary Anorgasmia
Summary
Anorgasmia, or the inability to obtain orgasm during a sexual encounter, affects about ten percent of women. Generally defined as resulting from not having learned how to achieve an orgasm, this condition is classified as either preorgasmia or primary anorgasmia. Secondary anorgasmia is the loss of ability to have an orgasm. Situational and random anorgasmia are types of secondary anorgasmia. Figure 1 shows a range of orgasmic activity.
|
Figure 1: Range of Orgasmic Responses |
||||
|
Total Anorgasm |
Orgasm with masturbation |
Orgasm with some sexual activity |
orgasm with a portion of sexual
encounters |
100% Orgasmic |
|
Can be primary |
Situational |
Random |
Absolute |
|
Physiologically, orgasm results from the release of vasocongestion and myotonia. During the orgasmic phase, there is a release of myotonia through contractions of muscles of the pelvic floor that surround the lower third of the vagina. Between five to 12 contractions occur at about one-second intervals. Vasocongestion is relieved as the vaginal muscles contract against the engorged vessels forcing out the trapped blood. Contractions of the uterus begin at the fundus and progress to the lower segment. Orgasmic pleasure is related to both the intervals and the intensity of the contractions.
Extragenital orgasmic responses are seen in several other body systems. Seventy-five percent of women have a sexual flush. The intensity of the flush appears to parallel the intensity of the orgasm. Both respiratory and heart rates increase, with respiration going as high as 30 to 40 breaths per minute while the pulse rate ranges from 110 to 180 beats per minute. There is also an elevation in blood pressure of between 30 to 80 mm/Hg systolic to 20 to 40 mm/Hg diastolic. The rectal sphincter also experiences muscle contractions similar to those of the vagina.
Preorgasmia is a term used to describe a person who has never achieved an orgasm through any type of sexual encounter. The inability to achieve orgasm can be complicated by a culture that is sexually inhibiting. For example, expectations that a female lover be compliant and self-sacrificing are still common. This passive sexual role for women can be repressive and lead them to deny sexual desires and experience inhibition of their sexual response cycle.
Most sexual therapists believe a woman can learn to be orgasmic. While learning to achieve orgasm may be relatively easy, learning to do so in every desired situation is more difficult.
Women with preorgasmia usually experience some sexual excitement. They may feel that intercourse is pleasant, but most of their pleasure comes from touching, holding, kissing, and caressing. They feel rewarded by the attention and approval they receive. If the level of sexual arousal is high, women may find the experience frustrating. High levels of muscle tension and pelvic engorgement without orgasmic release can lead to emotional irritability, restlessness, and pelvic pain.
Several factors appear to be related to preorgasmia. Sociocultural inhibitions that interfere with normal masturbation experimentation may prevent a woman from understanding what sexually excites her. Since orgasm is a learned response that contains both sensory and motor components, self-sexual exploration is an excellent way to learn this response. Providing a safe, secure, and supporting environment in which to explore their sexuality can enhance the chances that women can learn to have an orgasm.
Misinformation or a lack of factual information about sex and sexuality can also interfere with normal sexual development. Much success in treating preorgasmia has been obtained by using both educational and behavioral learning strategies. The first step in treating preorgasmia may be an educational program that teaches facts and corrects misconceptions. Understanding the normal sexual response cycle is important in learning to achieve orgasm. In addition, the presence of a sensuous, sexually knowledgeable woman as a role model (instead of one who is self-sacrificing and compliant) can contribute to the ability to achieve orgasm.
Partners with their own sexual problems (e.g., erectile difficulties and/or ejaculatory problems) can also be a factor in the orgasmic difficulties of women.
A woman can learn to become orgasmic alone or with a partner. For some, practicing self-stimulation may greatly enhance the learning process. An environment that maximizes stimulation while minimizing inhibition provides the greatest opportunity to learn. However, a woman who has never masturbated may need specific instruction on self-pleasuring. Self-stimulation can be performed manually or by using such devices as a vibrator or a pulsating steam of water. In some cases, counseling may be needed to help the woman become comfortable with her sensuous and sexual being.
After the woman has achieved orgasm through self-stimulation, the next step is for her to teach her partner what types of stimulation lead her to orgasm. Used with coital thrusting, a success rate of 83.49 percent in treating women with preorgasmia has been reported with this method.
Situational Anorgasmia
Random Anorgasmia
Secondary anorgasmia is the loss of ability to achieve orgasm. Its occurrence usually coincides with a "causal event." The causal event may be related to: alcoholism or drug addiction, depression, grief, medications, chronic or acute illness, or estrogen deprivation. Violation of sexual values, and loss of self-esteem are also factors that could be related to the causal event.
To regain the ability to achieve orgasm, both the biophysical and psychosocial needs of the woman must be met. Once these needs are recognized and fulfilled, orgasmic function generally returns. Treatment of secondary anorgasmia involves helping identify the unmet needs and formulating a plan to fulfill those needs. Needs may be as simple as a comfortable, warm, and private place in which to engage in sexual activities or as complex as confirming the trust and respect of the woman's partner.
Situational anorgasmia describes the condition of a woman who is orgasmic in some but not all sexual situations. Situational anorgasmia can take several forms. One form is the ability to reach orgasm through one type of sexual activity but not another (e.g., achieving orgasm through manual stimulation rather than the penis in vagina intercourse). A second form is the ability to achieve orgasm with one partner but not another. The ability to achieve orgasm in only one place or after a specific type or amount of foreplay is another form. These variations in orgasmic function may fall within the normal range of sexual expression and are usually not considered pathological. But a woman who experiences situational anorgasmia and wishes to extend or to change her current sexual patterns may find this condition problematic.
To learn to manage situational anorgasmia, the woman should first examine situations in which she achieves orgasm. If she can identify the factors that promote orgasm, she may be able to transfer them to her nonorgasmic encounters. The opposite is also helpful. A woman should explore her nonorgasmic situation and try to identify certain factors (e.g., fatigue, anxiety, or stress) that interfere with her sexual pleasure. In general she should try to improve communication, avoid performance anxiety, focus on sensation not cerebration, and use voluntary muscle contractions.
The woman must learn to bridge the difference between orgasmic and non-orgasmic situations. Bridging is the use of a successful sexual stimulation technique with the desired sexual technique so that the body learns to associate orgasm with the desired technique. An example is to perform manual stimulation of the clitoris simultaneously with penile thrusting so that the body begins to associate thrusting as well as manual stimulation with excitement and orgasm.
When a woman is dissatisfied with the number of sexual encounters in which orgasms occur, she is said to have random anorgasmia. Because there is no fixed number of encounters in which orgasm should be achieved, random anorgasmia is present only if the woman is unsatisfied with her orgasmic response. For many women, a sexual encounter can be gratifying and enjoyable even when no orgasm occurs, so the fact that each encounter is not orgasmic is not a problem for them.
When random anorgasmia occurs, it may be followed by performance anxiety. By focusing on whether she will have an orgasm, a woman can become tense and unresponsive; she must learn to focus on sensation rather than cerebration. Some women with random anorgasmia find it difficult to give up control of their sexual feelings and allow sensation to take over. Their treatment should include helping them give up the need to control their sexual feelings.
Achieving orgasm involves both physical and psychosocial factors. To be orgasmic, a woman's needs must be met within her sexual value system. While most women can learn to be orgasmic, transferring that ability to every sexual situation may be more difficult. Treatment includes behavioral therapy, education, and psychotherapy. Orgasm, however, is only one part of a gratifying sexual encounter.
REFERENCES
Annon, J. S. The Behavioral Treatment of Sexual Problems. Vol. 1. Honolulu: Mercantile Printing, 1974.
Barbach, L. For Yourself: The Fulfillment of Female Sexuality. Garden City, N.Y.: Anchor Press, 1976.
Heiman, J., L. LoPiccolo, and J. LoPiccolo. Becoming Orgasmic. New York: Prentice-Hall, 1976.
Hite, S. The Hite Report. New York: Macmillan: 1976.
Masters, W., and V. Johnson. Principles of the New Sex Therapy. American Journal of Psychiatry, Vol. 133 (May 1976), pp. 554-84.
Weisberg, M. Physiology of Female Sexual Function. Clinical Obstetrics and Gynecology, Vol. 27 (1984), pp. 697-705.
Sarah B. Freeman
The Culture of Anthropology: Its Paradigm
Methods, Findings, and Interpretations
Contemporary Perspectives and Concerns About Anthropology, Sex, and Culture
Central to the definition of anthropology as a discipline is the concept of culture. This concept pervades the diverse directions of research in the subfields of anthropology: physical anthropology, archaeology, linguistics, social-cultural anthropology, and psychological anthropology. The culture that underlies anthropology guides the questions it asks or does not ask, the concepts it employs, the content areas on which it focuses, the methods it uses, and the interpretation of information it collects. More specifically, it has guided the unique way in which anthropologists have investigated and analyzed human sexuality.
The first part of this discussion defines culture, establishes its importance to anthropology's paradigm as a discipline, and indicates the ways this paradigm has influenced anthropologists' approaches to human sexuality. The second part considers the ways in which the anthropological paradigm has shaped the research methods and the interpretation of findings about human sexuality.
Tylor, the founder of social anthropology, proposed culture as the central concern of anthropology in 1871, defining it as "that complex whole which includes knowledge, belief, art, law, morals, custom, and any other capabilities and habits acquired by man as a member of society." Fundamental to this definition are the attributes of holism, sharing in a social context, and tradition. Since then, definitions of the term have proliferated so much that the distinguished anthropologists Kroeber and Kluckhohn devoted their 1953 book Culture to a critical review of concepts and definitions. Their concluding definition is this:
Culture consists of patterns, explicit and implicit, of and for behavior acquired and transmitted by symbols, constituting the distinctive achievement of human groups, including their embodiments in artifacts; the essential core of culture consists of traditional (i.e., historically derived and selected) ideas and especially their attached values; culture systems may, on the one hand, be considered as products of action, on the other as conditioning elements of further action.In other words, the defining attributes of culture are that it is (1) patterned; (2) a basis for interpreting behavior and experience; (3) symbolic, containing many layers of meaning; (4) traditional, passed down from one generation to the next through learning; and (5) shared by members of a group. These core attributes of culture still define its domain. While art, music, and literature express and are a part of culture, the concept reaches beyond these domains to include ideas and beliefs that shape and interpret any behavior. Therefore, culture is different from society, which refers to shared patterns of behaving and interacting in a group. Culture relates to the meaning of behavior; society relates to the patterns of behavior. Clearly, the two overlap, but it is essential that they not be confused. Patterns of behavior can be observed, but the meaning is not apparent, although meaning can be inferred, analyzed, or derived from asking the participants to interpret their behavior.
Culture centers on knowledge, beliefs, and interpretation of behavior. The distinction between cultural and social factors is even more crucial to interpreting behavior because people's behavior (social aspect) and people's beliefs, ideas, and knowledge (cultural aspect) are not necessarily consistent with each other. The lack of consistency between them is just as interesting to research as their conformity with each other. To mesh them together is to lose an understanding of how culture functions in human societies. For example, a couple may know (a cultural factor) that they should use condoms during intercourse to lower the chances of contracting a sexually transmitted disease. However, they do not use a condom (a social factor). In this case, knowledge does not translate to behavior. Why? Judgment may be impaired because of drug use (a biological factor); a woman may not suggest condom use because of a belief that women are not supposed to be knowledgeable about sexual matters (a cultural factor); or a woman's partner may refuse to wear a condom because he says intercourse would be more pleasurable if he did not use one (a social factor).
A specific example of culture is Kuhn's concept of the paradigm, which he introduces in The Structure of Scientific Revolutions to describe ideas in the scientific community that define acceptable ways of conducting research and developing theories. What is acceptable depends on the assumptions of the era that underlie the methods, concepts, and interpretation of behavior, that is, the culture. Therefore, the way a discipline like anthropology applies a concept like culture to a topic like human sexuality is partly a product of its own culture - its traditions, its beliefs, and its symbols. A full understanding of the ways in which anthropologists interpret the link between culture and human sexuality depends on an appreciation of the ways in which the anthropological paradigm shapes its research methods and analyses. This helps to explain why some questions are focused on and others are not considered, and how human sexuality is conceptualized and interpreted.
Anthropology developed during the 19th century, a period of tremendous social and cultural change in the West: expansion of the British empire, the movement of settlers west in the United States, industrialization, and the impact of Darwin's theory of evolution. Explorers, government officials, missionaries, travelers, and intellectuals had been exposed to the social, cultural, and physical diversity of human beings. Questions revolved around how to order and interpret this diversity. Darwin's On the Origin of Species (1859) suggested an explanation for the diversity of life forms that he observed and became a basis for academic and popular interpretations of other kinds of diversity. His theory turned the guiding assumptions of 19th century Western culture on their head, shifting their bedrock from a spiritual to a natural view. Darwin asserted that all species are subject to natural laws; just as physical scientists had established physical laws of nature, Darwin was suggesting that biological life was governed by underlying natural laws that could be investigated and discovered.
The idea challenged traditional coventions that humans are special creations of God. In effect, it introduced a new worldview into the culture, postulating that there is a pattern underlying the physical, behavioral, and mental life of living things. This led to the development of new disciplines, including anthropology. Physical anthropologists began to investigate the evidence for human evolution, analyzing fossil remains and comparing the anatomy and physiology of humans with those of other animals. Archaeologists complemented the work of physical anthropologists by unearthing and analyzing artifacts (material remains of culture) of prehistoric humans. Because Darwin's evolutionary theory relied on natural selection rather than creation by God to explain the emergence of humans, science rather than God was positioned at the helm of the Western world's philosophical ship. Theorists of social evolution applied the principles of biological evolution to social and cultural groups; they eased the transition from a model of special creation to one of natural laws, because they hypothesized that there was a progression from primitive to civilized societies, a type of social evolution that gradually separated humans from other animals and resulted in the pinnacle of civilization: Western society, characterized by a monogamous nuclear family, superiority of males over females, belief in one God, and technological sophistication.
The initial anthropological framework for interpreting sexual behavior and customs was derived from the more general culture of the late 19th century: an emphasis on science and naturalistic explanations, evolutionary theory, ideas that would maintain social order in the face of a changed worldview, and explanation for diversity. The core tenets of anthropology fit in with that culture, as did anthropological approaches to sex.
Early anthropologists interpreted sex in evolutionary terms, primarily as a way to distinguish primitive from civilized societies. If humans were subject to natural laws, like other animals, it was more comforting to assume that some humans were less connected to animals than others. Social evolution provided a convenient buffer zone for "civilized" humans. Nineteenth-century theorists like Morgan used sexual behavior to define different stages of social evolution. Documented variations in customs in different societies could be incorporated into this view; societies with fewer restraints on sexual behavior were more primitive, closer to other animals, while those with more restraints and containment of sexuality in a monogamous marriage and family context were more civilized. The study of primitive societies gave clues to the origins of, and to the earlier forms of, human society. In a sense, these theories provided new creation myths based on natural social processes. Degree of control of sexuality was an essential aspect of these theories and overshadowed the study of sexual behavior itself.
A search for the origins of Western institutions, thought to be the height of civilized human existence, guided the theory and research at the time. Tylor's classic 1889 article "On a Method of Investigating the Development of Institutions" sought to explain the shift from matrilineality to patrilineality. Westermark's History of Human Marriage (1891) delved into the origins of human marriage by looking at the behavior of "lower" animals and "primitive" peoples, documenting how marriage evolved into the human family. Unwin's 1934 cross-cultural study, Sex and Culture, suggested that limitations on opportunities to gratify sexual desires are accompanied by a rise in "cultural condition." The emphasis on the institutional containment and regulation of sexuality has persisted in anthropology.
A general cultural commitment to maintaining order in the face of social and cultural changes encouraged a reinforcement of stable sex roles and a denial of sexual variations that could disrupt the social order. Darwin's theory of evolution supported current sexual biases by focusing on sexual selection as a process in which males actively competed for and initiated sex with females, who passively responded to advances. As a natural order replaced a spiritual one, it was women's place to remain subservient to men; reproductive functions sapped women of intellectual parity with men. Nevertheless, Birkin points out in Consuming Desire (1988) that Darwin may have been the first sexologist, because he did acknowledge the importance of female desire and choice, especially in shaping male secondary sexual characteristics (e.g., larger size, body hair, musculature); however, Tanner notes in her book On Becoming Human (1981) that when Darwin applied this principle to humans "male choice is now assumed, and it is female beauty that is seen as attracting the male" because, according to Darwin, "man is more powerful in body and mind than woman." Furthermore, although the middle-class, public version of sexual decorum was sexual restraint, the private world of sexual behavior teemed with prostitution, homosexuality, and nonmarital sex. In other words, the cultural proscriptions and the social behavior were at odds with each other. Why, then, was there such an effort to suppress acknowledgment of nonreproductive sexual behavior?
Denial of nonreproductive sex was consistent with the Christian tradition that was part of the social fabric of Europe and the United States. An ideal of sex within a context of heterosexual, monogamous marriage, bound by rules against premarital and extramarital sex, prevailed. To acknowledge some of these spiritual views would soften the transition to a more natural way of looking at the world. An emphasis on the danger and fear of sex has lingered, not only in anthropology but also in the educational system. Foucault's The History of Sexuality suggests that the avoidance of discourse about sex invested it with power over the imagination. In addition, fear and danger of sex could derive from its apparent ability to burst the confines of institutions, in a primal show of strength, and thus challenge the stability and order that theorists of the time were striving so valiantly to compose.
Finally, an emphasis on scientific investigation diverted direct attention from the erotic. Guided by principles of observation and objectivity, scientifically committed anthropologists would find it difficult to study what Western societies regarded as a private, subjective realm.
In sum, there is a clear relationship between the culture of the 19th century and the anthropological paradigm that has guided sex research. Concepts of culture, holism, and variety recur. Culture could explain varieties of belief and behavior, whether incorporated into an evolutionary theory or not. Holism could address concerns about the link among biological, social, cultural, and psychological aspects of human existence. Together, culture and holism could suggest an orderly way to interpret different kinds of variety. Sex was embedded in this theoretical context, transformed from sexual acts, desires, and attitudes into respectable theories, rules, and institutions.
Participant Observation: Method
Participant Observation: Findings and Interpretations
Cross-Cultural Research: Method
Cross-Cultural Research: Findings and Interpretations
According to Pelto and Pelto's Anthropological Research (1978), methodology is "the structure of procedures and transformational rules whereby the scientist shifts information up and down the ladder of abstraction in order to produce and organize increased knowledge." In other words, methodology defines the steps between the "real world" and general theory; the rules, procedures, and models provide a firm basis for believing that conclusions are sound. Methods derive from beliefs (i.e., cultural factors) about adequate evidence for thinking that something is true. This means that culture not only affects the paradigms of so-called objective scientists but also influences the type of methodology that is used to implement the goals of the discipline. In socio-cultural anthropology, the central concepts of the discipline have guided the types of methods that anthropologists have used to acquire knowledge. The advantages and constraints of these methods affect the kinds of information that anthropologists acquire for analysis, they have particularly affected whether and how anthropologists have gathered information on human sexuality.
The foundation of anthropological methodology was formed with its central concepts, culture and holism, and designed to explain the focus of anthropological research, an explanation for variety, whether it is physical, social, cultural, or psychological. One major method overshadows all others in cultural anthropology— participant observation. Important, but given much less attention in the discipline, is the cross-cultural method. The following discussion considers each of these methods, their application to research on human sexuality, and the types of analyses based on them.
Cultural anthropologists strive to understand shared meanings as they relate to physical events, individuals, and groups. Therefore, they enter the "field" (i.e., the social context or site of research) for a specific purpose — to observe, document, describe, and interpret the culture of the people in the field. Individual anthropologists endure physical hardship, psychological disorientation, and cognitive challenges in their attempts to glean meaning out of their new context, just as people in the 19th century tried to construct meaning in the face of social and cultural changes. Anthropologists in the field become explorers of shared meanings, as well as social and cultural detectives who articulate and construct the worldview and social organization of a group. Usually, the results of this method appear as an ethnography (i.e., a specific description of a culture and its social organization) or as a case study emphasizing a particular aspect of a group's existence. The primary task of the anthropologist is to be a participant observer — to straddle the line between objectivity and subjectivity by becoming involved enough to be a participant in the group yet distant and objective enough to describe the ideas and behaviors of the group. Consequently, anthropologists try to enter the field without many preconceived ideas of what they will find so that they will be open to the new beliefs and behaviors that they want to describe and interpret. The seeming lack of guidelines for a field experience is a deliberate attempt to counter bias and explore meaning.
The tenets of participant observation limit the investigation of sex even further. Canons of science encourage observation and objective description, but much of sexual behavior is private and not easily observed. Therefore, the anthropologist is likely to focus on more observable manifestations of sexual behaviors and attitudes, in economic life (e.g., the division of labor), in religion (e.g., rituals, gods and goddesses), in marriage and the family, in kinship categories, and in public sex roles. In addition, obtaining information about sex could require more time in the field to secure the trust of those providing such information. Also, the values of the anthropologist could deter him or her from obtaining information by engaging in sex with the people being studied. To have sex with an informant could be immoral and bias interpretations according to subjective experience. Finally, the gender of the anthropologist could affect the domains of experience in which she or he could participate. For example, men rarely observe childbirth, and women are not privy to aspects of men's initiation ceremonies. Therefore, beyond the constraints of the method, the field context could significantly limit the exploration of sexuality. The physical anthropologists Jane Goodall and Dian Fossey conducted research in a different kind of field: the primate habitat of chimpanzees and gorillas, respectively. Their research examines the similarities and differences between some of our closest primate relatives and human beings. Sexual behavior and a range of social interaction are more readily observed in this context than among humans.
Holism is another anthropological theme that has affected methodology. First, its influence emerges in the types of groups that anthropologists study. Usually, anthropologists study small communities or segments of larger societies so they can analyze the role that culture plays in the entire social context. This is advantageous in studying sexuality, because it enables the anthropologist to investigate nuances of meaning that a large-scale study would not permit. It also accentuates the diversity of contexts within which sexuality functions. Second, holism means that anthropologists are supposed to balance their descriptions of cultures by including a variety of information. Consequently, descriptions of sexual behavior and customs are likely to be integrated into an overall characterization of culture and not given central attention. However, they are likely to reveal connections to other aspects of social life that more specialized investigations are not likely to uncover.
Detailed descriptions of one or a few cultures and their social organization provide valuable information on the ways that sex is integrated into the culture and society. They also establish the variety of behaviors, customs, and nuances of meaning associated with sex. Finally, they allow anthropologists to prove in detail the ways in which order is established within one context. The interpretations and uses of this information vary according to the scope of the investigation, the goals of the researcher, and the reception of others.
Detailed Ethnographies and Case Studies. Malinowski, the father of fieldwork, established the tone for later studies in the field. He advocated meticulous investigation of the culture and the social organization, particularly how each aspect contributed to the functioning of the group. He viewed sex as more than a physical connection between bodies; it is a "sociological and cultural force" that cannot be studied apart from its cultural context. Beyond description, Malinowski had a theoretical agenda to confirm, that is, that culture and social organization function to fulfill human needs. Despite its sensational title, The Sexual Life of Savages (1929) deals more with institutions like marriage and the family than with descriptions of sexual behavior, all of which are interpreted as contributing to the coherence of the group's functioning.
Gregor's Anxious Pleasures (1985) is another illustration of the fruits of participant observation. Gregor did not intend to focus on sexuality when he went to Brazil to study the Mehinaku. However, his openness to meaning in the culture gave him no choice but to study sexuality, because it was "an organizing metaphor" for their lives; to describe their sexuality was to describe their culture. Suggs had a similar experience when he described the degree of sexual freedom and variety among the Marquesans in Marquesan Sexual Behavior (1966).
Some anthropologists provide insight into a culture by focusing on the life of an individual. Shostake does this in Nisa (1981), the biography of a !Kung Bushman woman whose life is enriched and exciting as she shifts from one man — husband or lover — to another just as other !Kung enjoy sex throughout the life cycle.
Other anthropologists focus their field research on a specific type of behavior or cultural category that they want to understand. For example, Mead focused on the nature of adolescence in Coming of Age in Samoa (1928). Spiro concentrated on the way culture modifies biology through acculturation in his monographs on the Israeli kibbutz — for example, Children of the Kibbutz (1958) and Gender and Culture (1979). Herdt studied why Sambian culture in highland New Guinea seems to encourage homosexual behavior before marriage in Guardians of the Flutes (1981) and continued his inquiry by focusing on the development of masculinity in Rituals of Manhood (1982); The Sambia: Ritual and Gender in New Guinea (1987) contextualizes the descriptions of the previous studies. Martin probes the symbolic significance of reproduction in The Woman in the Body (1987). Bolin studies the transition of transsexual males into women in In Search of Eve (1987). In The Zuni Man-Woman (1991) Roscoe explores the meaning of gender categories, as does Nanda's study of the hijras of India, Neither Man Nor Woman (1990). The linguist Tannen investigates the communication styles of men and women in U.S. society as part of their gendered subcultures in You Just Don't Understand (1990).
Comparative Studies. Some anthropologists conduct field research or use the case studies and ethnographies of others to establish the variety of customs, categories, and beliefs that relate to a specific domain of culture. Comparison with other groups is informal. For example. Mead compared sex roles among three New Guinea groups (Arapesh, Mundugumor, Tchambuli) in Sex and Temperament in Three Primitive Societies (1963) to demonstrate that sex roles and attitudes are not inborn but are a product of learning. In Women and Men (1975) Friedl explores how technological levels of society constrain sex roles. Marshall and Suggs's edited volume of case studies, Human Sexual Behavior (1971), is intended to derive comparative similarities and differences and then develop generalizations about influences on sexual behavior.
Often, collections and monographs concentrate on comparing cultures in terms of specific topics. For example, Gilmore's Manhood in the Making (1990) concentrates on cultural concepts of masculinity worldwide; Williams investigates the berdache and similar phenomena in The Spirit and the Flesh (1986); Kerns and Brown's edited volume, In Her Prime (1992), deals with women in midlife; and Buckley and Gottleib's edited work, Blood Magic (1988) explores the meaning of menstruation. Feldman's edited book, Culture and AIDS (1990) as well as Herdt and Lindenbaum's The Time of AIDS (1992) emphasizes the relevance of culture to understanding AIDS (acquired immune deficiency syndrome). All these works illustrate the variety of meanings that apply to different aspects of sexuality.
Some anthropologists use fieldwork and ethnographic data to establish consistency of meaning across cultures rather than to illustrate variety. For example, the physical anthropologist Symons draws on primate and comparative data in The Evolution of Human Sexuality (1979) to confirm his hypothesis that natural selection has produced marked sex differences in sexuality, extending to behavior, attitudes, and feelings. He thinks that selective pressures have produced consistent human patterns (e.g., male sexual jealousy, intense intrasexual competition among males, males' desire for a variety of sexual partners, females' tendency to be more conservative and selective about sexual partners). In contrast, the physical anthropologist Hrdy draws on her field data and other primate studies in The Woman That Never Evolved (1981) to demonstrate that sexually passive, noncompetitive, all-nurturing females are not a part of our primate heritage; competitive, sexually assertive, independent females were probably the norm. Fisher's The Sex Contract (1983) focuses on the evolutionary basis for male-female bonding, and cultural anthropologist Fox's The Red Lamp of Incest (1980) explains the widespread occurrence of the incest taboo as a human adaptation. All these studies address the link between biology and culture, primarily within a framework of sociobiology, where selective pressures guide the development of specific sexual behavior (e.g., mating patterns) as well as cultural and social forms (e.g., marriage, divorce, incest taboos). These perspectives are sometimes referred to as "essentialist" because they posit invariant aspects of human sexual behavior, attitudes, and feelings.
Cases as Examples. Ethnographic data often become part of a catalog of information on human sexuality, designed to illustrate its malleability and variety. Mantegazza's early Anthropological Studies on Sexual Relations of Mankind (1932), as well as Gregersen's more recent Sexual Practices (1983), illustrate this approach.
Ethnographies and case studies are extremely valuable bases for establishing the way in which culture is patterned and organized in a specific society, for highlighting the intricacies of meaning that culture entails, and for establishing the variety of sexual beliefs and behavior. However, they are not sufficient by themselves to generate valid generalizations about sexual behavior. They may be suggestive and compelling cases but are indicative rather than conclusive statements about general trends in human sexuality. A less popular but relevant method for dealing with patterns of human sexuality is the cross-cultural method. Ideally, it complements participant observation by using ethnographic data to establish which behavior and ideas are specific to a cultural context and which span across cultural contexts. However, anthropologists who have participated in fieldwork often argue that the cross-cultural method strips behavior and ideas of their meaning, while those who use the cross-cultural method say that case studies are not a sound basis for generalization about social and cultural life.
The cross-cultural method began with Tylor's classic article, "On a Method of Investigating the Development of Institutions" (1889) in which he classified, tabulated, and statistically analyzed data on 300-400 peoples to test his hypothesis about the development of marriage and rules of descent; Murdock's Social Structure (1949) was a major articulation of the main principles of the method and its usefulness in testing hypotheses about culture and social organization, particularly as they apply to the link between marriage, family, and sexual behavior. The elements of the method included (1) a classification of information to be compared, (2) a sample of societies, and (3) a statistical analysis. By examining variables in different combinations in a large and representative sample of societies drawn from different historical periods and geographical regions, cross-culturalists try to determine whether patterns of ideas and behavior can be substantiated statistically.
The steps of the method reveal important dimensions of the meaning of cultural categories and the aspects of human sexuality that have been investigated on a large scale. First, comparative categories have to be defined. This means that concepts often taken for granted by the investigator have to be articulated and defined in such a way that they can be identified in a wide range of contexts. For example, marriage does not always include a ceremony, a change in residence, or rights to children born of the union. Frayser found that a useful definition of marriage was a relationship in which having children is approved and encouraged; other attributes of marriage had to be investigated, not assumed. In this sense, this method is a corrective to investigators' ethnocentrism; cross-culturalists confront their biases with a range of cultures, while field workers confront it in their personal experience with one culture. Second, the researcher selects a sample of societies worldwide (at least 30) from which to obtain information. This ensures that different types of cultures are examined. Finally, appropriate statistical analyses are used to establish confidence in the patterns elucidated by this method. Trying to factor out what is consistent or variable across groups provides information about the dimensions of meaning attributed to a concept. Systematic cross-cultural research also has the benefit of identifying areas of human sexuality that have been neglected by field researchers - and many have, including homosexuality, forms of sexual stimulation, kinds of sexual interaction, the meaning of erotica, and interpretations of the body. Many of these gaps in the literature can be explained by the sexual paradigm of anthropologists that derives from a Western tradition steeped in beliefs about the fear and danger of sex.
Overviews. Unwin's Sex and Culture (1934) looked for grand patterns of sexual behavior in "uncivilized" cultures, while Murdock's Social Structure (1949) examined sexual behavior in relation to the development of patterns of descent, marriage, and the family. Ford and Beach's Patterns of Sexual Behavior (1951) combines a cross-cultural perspective with findings in biology to establish varieties of sexual life worldwide; the variables examined include sexual technique, homosexuality, and sexual partnerships. Frayser's Varieties of Sexual Experience (1985) goes beyond a description of sexual patterns to establish a model of human sexuality as a system in and of itself, related to but not incorporated by institutions like marriage, the family, and the economy. She establishes patterns of beliefs and behaviors that cluster together and apply across a range of societies, attempting to explain how social and cultural aspects of reproductive and nonreproductive sexuality relate to each other and to biological aspects. Naroll's The Moral Order (1983) summarizes findings from a variety of cross-cultural studies on sexual behavior, the family, and child abuse.
Specialized Topics. Most cross-cultural studies of human sexuality are much less inclusive than the ones previously mentioned and concentrate on specific topics. For example, Schlegel looks at the configuration of power and authority between men and women in Male Dominance and Female Autonomy (1972), and Sanday examines the fundamental question of why cultures select different styles of interaction between the sexes in Female Power and Male Dominance (1981). In Female of the Species (1975), Martin and Voorhies use cross-cultural data to demonstrate the ways in which sex differences relate to subsistence type and to illustrate that culture rather than biology is a more crucial determinant of sexual differentiation. Schlegel and Barry's Adolescence (1991) studies variations and consistencies in adolescence as a socially demarcated stage of life. Frayser and Whitby's Studies in Human Sexuality (1985) provides informative abstracts of monographs in a variety of fields that indicate the ways in which the concept of culture has been influential in the study of sexuality.
The original themes that guided anthropological research on human sexuality have not changed. Holism, the use of the concept of culture to establish the meaning of unfamiliar customs and beliefs, and an emphasis on documenting and explaining diversity are still with us. However, the conceptualization of human sexuality has changed over the last 100 years as the life, social, and behavioral sciences have contributed more research and data on the topic. Human sexuality does not refer to anatomy and physiology but to a complex whole of psychological, social, cultural, and biological attributes. Reproductive and nonreproductive aspects of sexuality are being studied as well as the way in which scientists have conceptualized sexual categories and behavior. Therefore, contemporary anthropological research on human sexuality is marked by a great deal of reflection and analysis focused on some familiar themes: (1) the impact of the biology of sex on the social, cultural, and psychological aspects of sex; (2) the social construction of concepts relating to sexuality, particularly ideas about gender, and the methods used to explore them, especially scientific ones; and (3) the meaning of consistent patterns of sexual behavior and beliefs worldwide (i.e., how to reconcile general trends with particular cultural contexts).
Feminist and gay anthropologists have been particularly productive and creative in their approaches to sexuality. For example, since the mid-1970s feminist anthropologists have examined the construction of sexuality itself, but have differed in what they think is constructed (e.g., acts identity, object choice, community). Rosaldo and Lamphere's Woman, Culture, and Society (1974); Ortner and Whitehead's Sexual Meanings (1981); Snitow, Stansell, and Thompson's Powers of Desire (1983); Vance's Pleasure and Danger (1984); and Ginsburg and Tsing's Uncertain Terms (1990) are notable collections of feminist discussions of sexuality as a social construction. Herdt and Stoller's Intimate Communications (1990) suggests a new method, clinical ethnography, as a way to study erotic aspects of life, and Bolton has recommended new uses of semantic-domain analysis and participant observation in the study of gay sexuality.
Nevertheless, as Vance says in her recent article "Anthropology Rediscovers Sexuality: A Theoretical Comment," "Anthropology as a field has been far from courageous or even adequate in its investigation of sexuality." The discipline still bears the burden of Western culture's ambivalence about sex and "appears to share the prevailing cultural view that sexuality is not an entirely legitimate area of study." Until this ambivalence is resolved on a wider level, anthropologists who study human sexuality will remain on the margins of the discipline.
REFERENCES
Birkin, L. Consuming Desire: Sexual Science and the Emergence of a Culture of Abundance, 1871-1914. Ithaca, N.Y.: Cornell Univ. Press, 1988.
Bolin, A. In Search of Eve: Transsexual Rites of Passage. South Hadley, Mass.: Bergin & Garvey, 1987.
Buckley, R., and A. Gottleib, eds. Blood Magic: An Anthropology of Menstruation. Berkeley: Univ. of California Press, 1988.
Darwin, C. On the Origin of Species by Means of Natural Selection, or, The Preservation of Favoured Races in the Struggle for Life. London: Watts, 1859.
Feldman, D.A., ed. Culture and AIDS. New York: Praeger, 1990.
Fisher, H. E. The Sex Contract: The Evolution of Human Behavior. New York: Quill, 1983.
Ford, C. S., and F. A. Beach. Patterns of Sexual Behavior. New York: Harper & Row, 1951.
Foucault, M. The History of Sexuality. Vol. 1, An Introduction. New York: Vintage, 1990.
Fox, R. The Red Lamp of Incest. New York: Dutton, 1980.
Frayser, S. G. Varieties of Sexual Experience: An Anthropological Perspective on Human Sexuality. New Haven, Conn.: Human Relations Area Files Press, 1985.
Freidl, E. Women and Men: An Anthropologist's View. New York: Holt, Rinehart & Winston, 1975.
Gilmore, D. D. Manhood in the Making: Cultural Concepts of Masculinity. New Haven, Conn.: Yale Univ. Press, 1990.
Ginsberg, F., and A. L. Tsing, eds. Uncertain Terms: Negotiating Gender in American Culture. Boston: Beacon Press, 1990.
Gregersen, E. Sexual Practices: The Story of Human Sexuality. New York: Franklin Watts, 1983.
Gregor, T. Anxious Pleasures: The Sexual Lives of an Amazonian People. Chicago: Univ. of Chicago Press, 1985.
Herdt, G. Guardians of the Flutes: Idioms of Masculinity. New York: McGraw-Hill, 1981.
Herdt, G. The Sambia: Ritual and Gender in New Guinea. New York: Holt, Rinehart & Winston, 1987.
Herdt, G., ed. Rituals of Manhood: Male Initiation in Papua, New Guinea. Berkeley: Univ. of California Press, 1982.
Herdt, G., and S. Lindenbaum. The Time of AIDS: Social Analysis, Theory, and Method. Newbury Park, Calif: Sage, 1992.
Hrdy, S. B. The Woman That Never Evolved. Cambridge, Mass.: Harvard Univ. Press, 1981.
Kerns, V., and J. K. Brown. In Her Prime: New Views of Middle-Aged Women. Urbana: Univ. of Illinois Press, 1992.
Kroeber, A. L., and C. Kluckhohn. Culture: A Critical Review of Concepts and Definitions. New York: Vintage, 1953.
Kuhn, T. S. The Structure of Scientific Revolutions. Chicago: Univ. of Chicago Press, 1962.
Malinowski, B. The Sexual Life of Savages of North-Western Melanesia: An Ethnographic Account of Courtship, Marriage, and Family Life Among the Natives of the Trobriand Islands, British New Guinea. London: Routledge & Sons, 1929.
Mantegazza, P. Anthropological Studies of Sexual Relations of Mankind. New York: Anthropological Press, 1932.
Marshall, D.S., and R. C. Suggs, eds. Human Sexual Behavior: Variations in the Ethnographic Spectrum. Englewood Cliffs, N.J.: Prentice-Hall, 1971.
Martin, M. K., and B. Voorhies. Female of the Species. New York: Columbia Univ. Press, 1975.
Mead, M. Coming of Age in Samoa. New York: William Morrow, 1928.
Mead, M. Sex and Temperament in Three Primitive Societies. New York: William Morrow, 1963.
Morgan, L. H. Ancient Society. 1877. Reprint. Cambridge, Mass.: Belknap, 1964.
Murdock, G. P. Social Structure. New York: Macmillan, 1949.
Nanda, S. Neither Man Nor Woman: The Hijras of India. Belmont, Calif: Wadsworth, 1990.
Naroll, R. The Moral Order: An Introduction to the Human Situation. Beverly Hills, Calif: Sage, 1983.
Ortner, S. B., and H. Whitehead. Sexual Meanings: The Cultural Construction of Gender and Sexuality. Cambridge: Cambridge Univ. Press, 1981.
Rosaldo, M. Z., and L. Lamphere, eds. Woman, Culture and Society. Stanford, Calif: Stanford Univ. Press, 1974.
Roscoe, W. The Zuni Man-Woman. Albuquerque: Univ. of New Mexico Press, 1991.
Sanday, P. R. Female Power and Male Dominance: On the Origins of Sexual Inequality. Cambridge: Cambridge Univ. Press, 1981.
Schlegel, A. Male Dominance and Female Autonomy: Domestic Authority in Matrilineal Societies. New Haven, Conn.: Human Relations Area Files Press, 1972.
Shostake, M. Nisa: The Life and Words of a !Kung Woman. Cambridge, Mass.: Harvard Univ. Press, 1981.
Snitow, A., C. Stansell, and S. Thompson, eds. Powers of Desire: The Politics of Sexuality. New York: Monthly Review, 1983.
Spiro, M. E. Children of the Kibbutz. Cambridge, Mass.: Harvard Univ. Press, 1958.
Spiro, M. E. Gender and Culture: Kibbutz Women Revisited. Durham, N.C.: Duke Univ. Press, 1979.
Suggs, R. C. Marquesan Sexual Behavior. New York: Harcourt, Brace & World, 1966.
Symons, D. The Evolution of Human Sexuality. New York: Oxford Univ. Press, 1979.
Tannen, D. You Just Don't Understand: Women and Men in Conversation. New York: William Morrow, 1990.
Tanner, N.M. On Becoming Human. Cambridge: Cambridge Univ. Press, 1981.
Tylor, E. B. On a Method of Investigating the Development of Institutions: Applied to Laws of Marriage and Descent, Journal of the Royal Anthropological Institute, Vol. 18 (1989), pp. 245-69.
Tylor, E. B. Primitive Culture. Boston: 1871.
Unwin, J. D. Sex and Culture. London: Oxford Univ. Press, 1934.
Vance, C. Anthropology Rediscovers Sexuality: A Theoretical Comment. Social Science and Medicine, Vol. 33 (1991), pp. 875-884.
Vance, C. S., ed. Pleasure and Danger: Exploring Female Sexuality. Boston: Routledge & Kegan Paul, 1984.
Westermark, E. History of Human Marriage. New York: Macmillan, 1981.
Williams, W. The Spirit and the Flesh: Sexual Diversity in American Indian Culture. Boston: Beacon Press, 1986.
Suzanne G. Frayser
Aphrodisiacs
Anaphrodisiac
The word "aphrodisiac" derives from "Aphrodite," the name of the mythical Greek goddess of love and beauty. The Greeks considered her the personification of the sexual urge. The definition, and therefore the scope, of the word aphrodisiac varies among authors. In a limited sense, an aphrodisiac is a substance that either produces penile erections or, without other sexual stimulation, increases sexual desire. This definition differs from more expansive concepts of the word both in what is considered to cause the desired effect and in the effects desired. In its broadest sense, aphrodisiacs may be divided into two main categories:
1. Aphrodisiacs that are thought to have primarily a direct biochemical effect. This includes material that is ingested (e.g., certain foods, drugs, medicines, fluids), injected or inhaled into the body (e.g., certain drugs, fragrances, medicines), or applied onto a surface of the body (e.g., certain ointments, lotions).Under the broad definition of an aphrodisiac, the desired or supposed effect may arouse sexual feelings by stimulating genitals, increase sexual awareness, relax inhibitions, augment physical energy, strengthen the gonads or other glands involved with sexual activity, improve sexual health, increase the production of semen, overcome or delay sexual exhaustion, prevent premature ejaculation, prolong sexual life, recapture lost virility, reduce ejaculatory failure, increase pleasure during sexual activities, enhance sexual attractiveness, produce orgasms, or attain sexual mastery over someone.2. Aphrodisiacs that are thought to have primarily a psychophysiological effect. This includes material that is seen or heard (e.g., erotic art, erotic dance, certain emotional music) or stimuli that are otherwise experienced (e.g., certain moving religious experiences, erotic fantasies, magic practices, high-risk adventures).
Throughout recorded human history people at various times and in various cultures have used a wide variety of things to attempt to enhance aspects of their own sexual vigor or sexual desire or sexual desirability, or to enhance one or more of those factors in a desired other person. Early on, people became acutely aware of the importance of the continual renewal of the life forces they depended on: their crop and game food, the seasons, and their family, tribe, and eventually, their larger community. Failure to continually renew any of these threatened disaster to the individual and to the larger group. It was only natural for ancient peoples to seek some means of gaining some control over the inevitable renewal failures that could and did occur in all of those life forms.
Having little or no understanding of the actual physical and biological mechanisms involved in replenishing life forms, individuals and groups developed systems of belief about what was going on and why. And they began developing beliefs about what they could do to ensure their continued sexual successes and reproductive functioning. Early in human history, people who felt the need for such help sought the assistance of what they perceived to be superior powers: they worshiped naturalistic gods, invoked magic, and experimented with natural substances.
Stretching over such a long time and involving such diverse cultures, the list of items that have been tried and promoted as aphrodisiacs is immense. They range from the simple and the innocuous to the odious, the esoteric, and the harmful.
Among the earliest known aphrodisiacs were certain edible foods thought to resemble human sex organs (e.g., clams, oysters, cucumbers, asparagus, bananas, rhinoceros horns). Ingesting these foods, a practice that has not entirely abated even today, was based on the belief that God put a mark on all food to indicate its purpose. It was thought that the appearance, color, shape, or smell of a plant or other substance indicated its link to, and usefulness regarding, a particular ailment or body part. The logic being, why else are they thus? A 16th-century scholar dubbed that concept the "Doctrine of Signatures."
When families and clans evolved into larger groups, the interest of group survival became so important that something so vital as the reproductive success of the group could no longer be left to the inconsistent intellectual abilities of its individual members. Also, as is true even today, the power of knowledge and of control over the sexual and reproductive functions of a group directly translates into social and political power. Control of that power became important to group leaders.
Those are some reasons why, as established groups grew and evolved into civilizations, the accumulated group knowledge of aphrodisiac "cures" and "remedies" devolved to and became part of the province of the members of the priesthoods that had also developed by then. With that transition came more complex "recipes." Magic (or "divine" intervention) often became important in many aphrodisiac mixtures, both in their preparation and in their administration. Often the rules governing the preparation of the concoctions were a study in complexity steeped in mysticism. For example, one potion consisted of a compound of the brains of a cat and of a lizard, the menstrual blood of a whore, human semen, the womb of a bitch in heat that had been denied the companionship of dogs, the entrails of a hyena, and the left skull bone of a toad.
A concept that appealed to ancient minds, as it still does to some modern minds, is the idea that there is curative, generative, or strengthening power in the genitals of animals. Two other themes that appear throughout much of the recorded history of aphrodisiacs are the persistent use of the waste products and the blood and semen of both humans and animals. The writings of Paulinus, which were popular during medieval times, are useful examples of these customs. They recognized the supposed efficacy of various animal genitals (e.g., testes of the hare and of the stag, and the donkey penis), of various animal waste products (e.g., bull urine, poultry excrement, vaginal discharges from sows), and of sparrow blood and the semen of various animals.
Many concoctions have been designed to be applied to the surface of the sexual organs. Through supposed magical powers, through chemical action, or through both, the potions applied were thought to increase the recipient's sexual desire or sexual organ functioning, or cause a desired increase in fecundity or other sexual power. The chemical action of some of the compounds causes irritation and increased blood flow to the application area, and some cause mild or serious injuries.
All forms of nourishing and not-so-nourishing foods have been recommended at times as aids to sexual vigor and interest. Long before the chemistry of food and the nutritional needs of humans were understood, it took only simple observational skills to recognize that the intake of certain foods would normally give one an energy boost and enhance one's overall sense of well-being, especially for someone whose regular nutritional intake was poor. It is therefore not surprising that two of the most common foods used for their perceived aphrodisiac effects are honey and milk.
The early authorities who extolled the aphrodisiac virtues of what are known today to be nourishing foods of various kinds were recognizing the health-enhancing benefits of adequate nutrition. In the process, at one time or another, items purported to have aphrodisiac qualities include many, if not most, of the known fruits, grains, vegetables, meats, edible herbs, and nutritional fluids.
In public libraries today one can find books on how to grow a whole garden of purported aphrodisiac herbs or aphrodisiac vegetables. Books also exist that describe how to cook meals said to turn on or turn up the libido, or to strengthen one's sexual capacities.
One striking fact emerging from the literature on aphrodisiacs is the dearth of reported studies on proclaimed aphrodisiacs that have used accepted scientific methodology. Hence, the efficacy of all but a very few purported aphrodisiacs is obscured in a cloud of unproven legends, magic rituals, folktales, and individual anecdotes; a placebo effect being apparent in some of them.
A person's response to an experience — such as an intake of food or a drug, or an emotional event — may be affected by many things. These include the individual's expectations; the accompanying environment; the strength, amount, and duration of the substance or event; one's preexisting conditions; and the interaction of other substances or events that are being or have been experienced. The methodology used by the researcher to measure and evaluate results may also affect the validity of conclusions. Seldom have all of these been adequately controlled in studies of a supposed aphrodisiac.
Recent reports in scientific literature concerning some substances indicate that they appeared to have an aphrodisiac effect in some individuals. Libido has been reportedly augmented by oral administration of L-dopa, of nomifensine, of chlomipramine, and of a compound made from extracts of avena sativa (oats) and urtica (nettles), and by intracerebral injection of acetylcholine. Fenfluramine (used to treat bulimia) and trazodone (used as an antidepressant) have reportedly caused an increased libido effect in some females. Three aliphatic nitrites — amyl, butyl, and isobutyl — have been shown to subjectively increase the pleasure of orgasm and to enhance sexual performance in some persons who inhale the substance during sexual activity. Some reports hold that the intake of cocaine acts as an aphrodisiac in some cases, but that too appears to be dose-related and individual specific.
It is now well established that some compounds when injected into the penis will in all but rare cases cause an erection. Such substances include papaverine (sometimes combined with phentolamine) and prostaglandin E 1.
The U.S. Food and Drug Administration (FDA) issued a ruling in 1989 stating that any aphrodisiac drug product for over-the-counter human use is not generally recognized as safe and effective and is misbranded. The FDA warned of the serious health risks of some alleged aphrodisiacs, such as cantharides (Spanish fly), and ruled that the safety and effectiveness of ginseng, golden seal, gotu kola, nux vomica, Pega Palo, yohimbine, and strychnine as aphrodisiacs are unproven. The FDA stated: "Individuals suffering from decreased libido and impaired sexual performance should seek professional medical care or counseling."
Broadly defined an anaphrodisiac is any substance or experience that decreases sexual desire, sexual desirability, general sexual health, or sexual functioning. More narrowly defined, the word means any substance that decreases sexual desire or sexual functioning. Other terms sometimes used are antaphrodisiac, antiaphrodisiac, and refrigerant (Roman).
As they did with aphrodisiacs, the ancients also had a cornucopia of anaphrodisiacs. People have used as anaphrodisiacs a multiplicity of foods, plants, secretions and parts of humans and animals, chemical compounds, and magic. Ranging from the benign (e.g., cold baths) to the unpleasant (e.g., a drink made from pounded willow leaves) to the harmful (e.g., hemlock tea), many of the old remedies no doubt reduced sexual ardor by making the recipient uncomfortable, ill, or worse.
Ethyl alcohol has long been recognized as sometimes being a disinhibiting aphrodisiac when consumed in small doses but producing many anaphrodisiac effects when consumed in increasing volume.
In modem times, chemists have devised many compounds for humans to consume in their search for better health or recreation or mental escape. Some seem to have an anaphrodisiac effect, if only in certain doses or in certain people.
Amphetamines are drugs used for a variety of purposes, including mood elevation, depression control, alertness, and appetite suppression. Dose-related anaphrodisiac effects have been reported in some cases. There have been similar reports about other types of antidepressants (e.g., such as amitriptyline hydrochloride, imipramine, tranylcypromine, and mianserin).
Barbiturates are sedative or hypnotic drugs used to reduce tension or to induce sleep. In the few studies of their effects on sexual desire or functioning, there are some reports of an anaphrodisiac effect in some people from continued use.
Drugs used to treat various blood-related disorders, such as high blood pressure, may in some individuals cause diminished sexual functioning (e.g., reduced penile or vulval engorgement).
Medroxprogesterone acetate (Depo-Provera) and flutamide combined with an LHRH agonist are two chemical treatments sometimes purposely administered to a male in order to alter his criminal or antisocial sexual behavior by reducing the level of his naturally produced androgen hormones or by blocking some of the effects on his body of those hormones. The results of an effective treatment may range from a general lowering of libido and no alteration of erectile ability to a near or total loss of libido and erectile ability.
REFERENCES
Sabatier, R., trans. Magica Sexualis. New York: Falstaff Press, 1934.
Taberner, P. V. Aphrodisiacs: The Science and the Myth. London: Croom Helm, 1985.
Walton, A.H. Aphrodisiacs: From Legend to Prescription. Westport, Conn.: Associated Booksellers, 1958.
Wedeck, H. E. Dictionary of Aphrodisiacs. New York: Philosophical Library, 1961.
Joan K. Dixon
Dwight Dixon
Western Christian Tradition
Growth of Erotic Art
It is a truism that people have always tended to humanize and sexualize their universe. Among paleolithic people, this was often done through giving sexual meaning to natural objects. An interesting example is found at Le Portel, one of a series of caves in southern France and northern Spain, where a protuberance on a cave wall is used as a phallus for a figure crudely outlined in red. There is also more deliberative art, exemplified by the so-called Paleolithic Venuses, female figurines with enormous breasts hanging heavily above a swelling belly and with enormous hips, buttocks, and thighs. One of the more famous of these figures is the Venus of Willendorf, found in Austria and dating from about 30, 000 B.C.E.
As civilization developed, more sophisticated representations appeared. Egyptian tomb paintings, statues, and papyrus drawings often include scenes of sexual intercourse. Min, a god with bull-man attributes, is portrayed as clasping his phallus in various statues. The flooding of the Nile was identified with the semen of Osiris, and his phallus dominated some of the ceremonies associated with this annual event. Throughout the ancient world, amulets for love, magic, and fertility often included the cowrie shell, a vulva symbol.
In the Tigris-Euphrates valley, another center of early civilization, there are numerous terracotta reliefs depicting copulation from behind, although it often is not clear whether vaginal or anal intercourse is depicted. Surviving from ancient India are many representations of the lingam (penis) combined with the yoni (vulva), the most common being a round-topped cylinder standing in a shallow circular basin with a spout to one side. Indian temples are full of sculptures of women in a variety of sexual postures. A variety of positions of sexual intercourse are also depicted. Much of ancient Chinese art and literature is based on the coming together of the yin and the yang, the female and male principles, a union which is best achieved through sexual intercourse.
In ancient Peru, the early Mochica civilization, a predecessor to the Incas, was extremely prolific in its ceramic reproduction of sexual scenes. About 1 percent of the surviving cups and bowls are molded to form couples or individuals in various sexual poses. Aztec codices from Mexico include numerous sexual scenes. In fact, wherever one turns either in ancient civilizations or among contemporary primitives, sex seems to form a dominant feature of the art, and the miracle of procreation seems to be a dominant theme in the legends and religions of all peoples.
The theme of sex continued among the founders of Western culture, in the civilizations of Greece and Rome. Popular mythology recounting the love stories of the gods served as both erotic inspiration and symbolic representation of fertility in nature. The story of Leda and her swan lover is often portrayed in marble relief, and nude images of goddesses such as Aphrodite are common. However, the major sources of sex scenes in the Greek world are vase paintings which have survived in great quantity and include representations of almost every aspect of sexual activity from masturbation to homosexuality to bestiality. There is also widespread distribution of small, often crude erotic figurines of the gods, and many of the male gods have a massive phallus. In Rome, the cult of the phallus was part of the Roman religion, and penises are depicted literally everywhere—in floor mosaics, tombs, and amulets that have survived in great numbers. Lamps were formed in the shape of a phallus, and there were even phallic shrines. Initiation into various mystery religions involved the concept of rebirth, and various representations of female genitals were an essential part of such rituals. Often explicit sexual scenes were also part of the temple art, particularly that devoted to the god Dionysus, some of which survives in the Temple of Mysteries at Pompeii. Here the scenes vary: the god gently caresses the goddess Ariadne; a figure of a woman brandishes a whip, while another dances in the nude; they are what one author chose to label as portrayals of "sexual abandon." Also surviving from Pompeii are brothel scenes and various amulets depicting sexual intercourse in a variety of positions.
With the triumph of Christianity, the nature of sexual representation in art in the West changed. Whereas sexuality had played a major part in pre-Christian religions and sexuality was very much an element of the religious ceremony, sexuality tended to be something to be avoided and repressed in early Christian thinking. The nude, which had been the prime erotic figure, no longer appeared except in almost asexual representations of Jesus on the cross. When sexual and erotic art begins to appear again, it is equated more with humiliation and shame, at least on the official level. Undoubtedly, ordinary people kept alive some of the more erotic and sexual ideas, but little of this has survived. In fact, much information about sexuality known to earlier peoples seems to have been repressed or passed on only through oral rather than written traditions. Still, some sexual artifacts have survived, mainly articles of value owned by the rich. Jewelry, decorated furniture, and illustrated manuscripts with erotic scenes are examples. A set of silver plates in the Hermitage Museum, a 9th-century ivory casket from Italy in the Victoria and Albert Museum, and a 13th century gilt mirror in Frankfurt's Städelinstitut are all decorated with scenes of love making. The manuscripts, usually from a later period, depict allegories such as the fountain of youth, the garden of love, and the garden of earthly delights, all themes that allowed the artist to include illustrations of sexual activity. Examples of such manuscripts are the Douce Manuscript in the Bodleian Library, Oxford, and the Trés Riches Heures du Duc de Berry, which has been reprinted in modem copies.
Since the church was the main patron of the artists, there were restrictions on what could be portrayed. Two different forms of sexual themes did appear, however, the more public one seen by all, and the more secretive or less public one known to a few. Among the more visible are the religious carvings found in the public parts of buildings, such as those surrounding doorways and facades. Many of the depictions of sexuality in these areas center around the story of Adam and Eve, the sin of unchastity, and the representation of the Last Judgment. Such portrayals are most evident in the new-style Gothic cathedrals of the 12th and later centuries.
Since the purpose of such art was to educate, inevitably it is not the sins of unchastity that are shown, for example, but the punishments that result from them—the breasts and vulva of the women being penetrated and eaten away by serpents and toads. Similarly, the Last Judgment emphasizes the sins of sexual intercourse taking place in hell, and portrayals of Adam and Eve show them covering their nudity.
There are, however, less public parts of the building, such as the rooftop gargoyles or the undersides of the seats in the choir stalls (misericord), where medieval artists could give freer expression to their erotic and scatological impulses. Among gargoyle representations that have survived are drainpipes that channel water through the anus of various figures or create the illusion that a female figure is urinating.
Many churches also include representations of what are called Shelah-na-Gig fertility figures, that is, figures of nude women exposing their vulvas. They are believed to be artifacts, or even a medieval continuation, of pre-Christian religious beliefs and were preserved as a sort of transition to the new religion of Christianity, part of a church policy not to destroy the idols of the heathen but to incorporate them into the Christian tradition. In some churches in Spain, couples are even shown engaged in intercourse.
The depictions of sexuality on the underside of the seats in churches are generally light-hearted— for example, showing dancing women whose garments are flying and exposing parts of their bodies. One favorite kind of carving is of devil figures with enlarged phalluses. Such carvings were usually seen only by the clergy, and knowledge of them was restricted.
Gradually, toward the end of the Middle Ages, the nudes became more realistic and erotic, particularly in northern Europe, where they were shown with pubic hair and, in the case of women, sometimes with a vulva as well. Some major artists, such as Hieronymus Bosch (1450-1516), Pieter Bruegel (1525-1569), and Albrecht Dürer (1471-1528), frequently used erotic themes in their drawings, woodcuts, and engravings. Particularly daring was the Swiss goldsmith Urs Graf (1485-1527/8), who is noteworthy for his lively and uninhibited drawings of prostitutes.
Climaxing this growing northern European tradition of eroticism were Lucas Cranach (1472- 1553) and Hans Baldung (also called Grien; 1484-1545). Cranach's eroticism is most evident in his mythological panels of Venus, the Graces, the Judgment of Paris, and others, where his nudes are clothed in necklaces, transparent veils, and often large picture hats. Baldung, in contrast, has a penchant for the gruesome and macabre and often links sexuality and death. In his paintings, drawings and engravings, woman is the personification of lust and Death is her most frequent companion.
In Italy, the 15th and 16th centuries saw a return to the ideals of classical Greece and Rome in a period usually known as the Renaissance. Here the nude does not have the perverse element present in the north, but rather a kind of sensual eroticism. A number of Venetian painters were particularly important, including Giovanni Bellini (1430/40-1516), whose painting The Feast of the Gods emphasizes the increasing stress on eroticism. Two of his pupils, Giorgione (1475-1510) and Titian (1487-1576), carried on the tradition. Giorgione's Fête Champêtre is the prototype of the erotic pastoral idyll in European art, while his Venus and Titian's Venus of Urbino are the first in a long line of calmly erotic nudes.
In Florence, Donatello (1386-1466), the sculptor whose David is the first freestanding bronze sculpture cast since antiquity, portrays an erotic celebration of the adolescent body. Many of the Florentine artists had erotic and even pornographic themes in their work. Michelangelo (1475-1564), for example, included a man wearing a phallus on his bonnet in a drawing in the Vatican collection, and in an engraving, The Dream of Human Life, there is a mysterious giant hand grasping a huge phallus as well as a disembodied phallus floating in the sky. Botticelli (1445- 1510) emphasized erotic nudeness in his group of the Three Graces, while Leonardo da Vinci (1452-1519), in a painting now lost, recreated the erotic myth of Leda and the swan, the first re-creation since antiquity. Leonardo's sketches, however, survive. Raphael (1483-1520), in La Fornarina portrayed his mistress with her breasts bared, marking a new type of painting, the erotic portrait. Raphael also designed the erotic frescoes of Venus and Cupid, Cupid and Psyche, and Vulcan and Pallas for the bathroom of Cardinal Bibbiena in the Vatican, although the actual painting was done by Raphael's pupils. Few, however, have seen the paintings, since permission, until recently, was rarely given, and some of the frescoes were later whitewashed.
This new sensuality did not go unchallenged. One result of the new morality associated with the Protestant and Catholic reformations was the so-called breeches makers, individuals who put clothing or fig leaves on nude representations in public places. When pants seemed unsuitable, fig leaves were painted on or attached to sculptures, and in Spain the nude itself was more or less perpetually banned. Even Michelangelo's frescoes on the ceiling of the Sistine Chapel were called obscene; Pope Paul IV, in 1555, was so concerned about this accusation that he ordered them removed from the chapel, an action which would in effect have meant destroying them. When his decision became public, such a storm of protest arose that he retracted his order and instead directed that clothes be put on the heavenly hosts in The Last Judgment, and on the Virgin Mary and the angels surrounding her. Michelangelo's picture of Leda and the Swan, on the same theme as the one by Leonardo, was burned by the French.
Artists became more daring in spite of reaction, and a few painted or sculpted specifically sexual scenes. The market for these works grew as the first mass market for art developed from the possibility of making copies of originals through engraving. Giulio Romano (1499-1546), a pupil and later assistant to Raphael, undertook to portray 16 different postures of coitus in a series called Posizione to illustrate some verses by Pietro Aretino (1492-1556). When Romano completed them in 1524, he turned to the new technique of engraving to have copies made on a wide scale. When these engravings came to the attention of Pope Clement VII, he expressed shock that such pictures could not only be published in Rome but be painted by an artist often employed by the Church. Ultimately, Romano, his engraver Marcantonio Raimondi, and the poet Aretino had to flee Rome. The original pictures were destroyed, but the engravings survived.
Engraving, in fact, opened up greater opportunities for more sexually explicit art, since it allowed the artist to circulate his work more or less underground. One artist who took advantage of this was Agostino Carrachi (1557-1602), who did a series of paintings on the theme of Love in the Golden Age, that shows various nude couples making love in a variety of different and detailed landscapes. His most famous erotic work is a series of engravings known as Lascivie, of which a dozen or so prints have survived. Until recently, they were kept in the locked collections of various museums. One print, owned by the British Museum, shows a satyr having intercourse with a nymph against a tree trunk. Most of the prints depict nymphs and satyrs and show, among other things, a masturbating satyr and a satyr whipping a nude nymph. They also include biblical subjects such as Lot committing incest with his daughters, a religious theme that lent itself to explicit sexuality.
Usually, however, it was safer to use classical themes rather than biblical ones since the artist could claim to be simply representing pagan customs. Francesco Mazzola Parmigiano (1503- 1540), for example, did a series on Loves of the Gods, some of which (e.g., Mars having intercourse with Venus) has survived in the collections of the British Museum. Witches were also a favorite subject of erotic engravings, since they were seen to have particular sexual powers, and it was these sexual powers that made them such a threat to true believers. One engraving of Parmigianino, also in the British Museum and entitled Witches Sabbath, shows a witch riding a giant phallus.
Generally, artists were reluctant until the end of the 16th century to anger the church publicly by using forbidden sexual themes, since the church was a major patron of the arts. As more secular buyers appeared, however, erotic themes became less disguised and more open. Major artists often sketched figures engaged in sexual activities either for their private customers or for their own edification, even if in their more public works they avoided sexual scenes. Rembrandt (1606 -1669), for example, did several such sketches, including Monk in a Cornfield in which the monk is having intercourse; Sleeping Shepherd, in which a couple is engaging in sexual intercourse while the shepherd sleeps; and Ledakant, in which a couple is having intercourse on a large bed. Ledakant is believed to represent the artist and his mistress-model, Hendrickje Stoffels. Peter Paul Rubens (1577-1640) was the first artist who dared to paint an erotic portrayal of the woman he loved, Helen Fourment in a Fur Cloak, without concealing it behind a biblical or mythological story. Rubens had a powerful sensual technique, which played to advantage in such erotic scenes as The Rape of the Daughters of Leukippos, again a classical legend used to justify a sexually explicit work. In the painting, a crowd of nude girls is being attacked by sexually excited men.
Caravaggio (1573-1610), who had many of his religious commissions rejected on the ground of indecorum, also made many paintings of nude male saints that, in spite of their strong suggestions of homoeroticism, somehow passed the censors. In Spain, censorship was carried out by the court, upon which increasing numbers of artists depended for support; however, eroticism and sexuality still managed to make an appearance, though often subterfuges were used to disguise them. For example, Velazquez (1599-1660), a court painter, painted a nude Venus, known as the Rokeby Venus, but from the rear rather than the front, supposedly to circumvent sexual prohibitions. Still, the eroticism somehow manages to express itself in the buttocks, and some have regarded the Rokeby Venus as a particularly sensuous and erotic portrait. Francisco Goya (1746-1828) adopted another alternative in his nude painting of the Naked Maja, a courtesan in a full frontal position. It was painted to be enjoyed in private because it was hidden behind another painting of the woman in the same position but clothed (Clothed Maja). Goya also made sexually oriented etchings, many with sadistic and masochistic themes, which could be circulated privately.
Royal or noble mistresses often served as models for some of the more erotic paintings, a genre encouraged by various French royal patrons. Usually, the mistresses were used to illustrate various classical legends, which allowed them to appear nude or in various erotic positions without raising religious objections. Among the more erotic of the French court painters was Francois Boucher (1703-1770) who in the terms of one scholar was "passionately devoted" to the beauties of the female figure and made thousands of nude sketches. One of his favorite themes was Loves of the Gods, the same theme so widely used in the 16th century to escape censorship. He also painted the nude Venus in many different sexual poses, usually selecting a different mistress from among the many he had as a model for each. Madame de Pompadour, mistress of Louis XV, commissioned him to paint the highly erotic four Loves of Venus in 1754, in the hope of arousing the king, whose affections were beginning to stray. Boucher's erotic pictures were openly sexual, and many have not survived in their original form; the most famous of his erotic works, six rustic scenes that were destroyed by fire in 1871, survive only in photographic copies made shortly before the fire. The scenes include two of nude couples copulating on a bed, a girl buying a winged phallus from a man and playing with her vulva, a man having sex with a nude woman from behind, a man about to have intercourse with a partly unclothed woman whose breasts and genitals are exposed, and a girl with her hand on a boy's erect penis.
Another court painter was Jean Honorë Fragonard (1732-1806), who is today chiefly remembered for his erotic canvases such as The Swing, where a woman clothed in yards of pink and blue silk has kicked up her legs and revealed her satin stockings to an excited young man lying among the roses in the foreground. Fragonard, however, specialized in bedroom scenes, many of which were destroyed in the 19th century because they were regarded as indecent; sketches and prints remain of some of them.
In England in the 18th century, William Hogarth (1697-1764) made vice his specialty. He got away with much of his eroticism because in his engravings he presented what he called moral topics. In a series such as The Harlot's Progress, he attempted to tell the story of a young girl who takes up prostitution and dies within the year. Though his eroticism led to the cancellation of a royal commission, his popularity with the masses was great. One of his drawings, Boys Peeping at Nature, perhaps reflects his own feelings about the false "delicacy" of English taste, since he portrays a boy looking under the skirt that has been put around a statue of a nude woman.
Much more deliberately erotic was Thomas Rowlandson (1767-1827), who abandoned oils for water colors and etching. He had a taste for the bawdy, and most of his works were apparently commissioned by the Prince of Wales before he became King George IV. Rowlandson's work falls into two main categories, one celebrating the sexual pleasures of ordinary people from all walks of life, with such scenes as soldiers whoring or a wife making time with her lover while her husband is absent. The second category is devoted to the upper classes. Included in this latter group of erotic works is a portrayal of a couple having intercourse on horseback, while another picture shows a couple having intercourse in a carriage. Both were part of a series published posthumously for the artist's friends and accompanied by a descriptive poem entitled "Pretty Little Games for Young Ladies and Gentlemen." Many of his prints, paintings, and drawings convey an almost voyeuristic element.
Also active at this period was Henry Fuseli (1741-1825), a Swiss artist, who spent much of his life in London. He produced hundreds of erotic drawings, many of them rather obscene and probably done for his own edification. This makes them more personal than most erotic art and they reveal his own obsession with lascivious, haughty, and dominating women. He explored various forms of sexuality, and among his drawings is one illustrating a young lesbian couple that represents a breakthrough into new topical areas.
By the 19th century, with the ability of artists to sell to a larger variety of patrons and customers, erotic art became more plentiful than ever before. Sexuality, or rather repressed sexuality, was a strong undercurrent in the Victorian period, and with it came the artist to satisfy the need for sexual arousal. Many prominent artists painted erotic and sexual scenes either for their own edification or for select customers. J. M. W. Turner (1775-1851), for example, famous for his sea pictures and landscapes, was a major producer of erotica, much of which was destroyed by his executor, John Ruskin, because it was considered objectionable. Still, many works survived, most of them still unpublished but found in his sketchbooks in the British Museum. They show very explicit erotic scenes. Numerous men with an erection are shown copulating with women or fondling them, and women are shown performing fellatio on men; other pictures are more detailed showing a penis entering a woman's vagina or a man kissing a woman while manipulating her vulva with his fingers.
The number of artists who dealt with erotic themes increased so much that only a few can be mentioned. They range from Jean Ingres (1780-1867), to Ferdinand-Victor Delacroix (1798-1863) and F. Rops (1833-1898). Rops, in fact, concentrated his whole vision on human sexual behavior as it existed in the world of prostitutes, cabarets, and cafes. Rops might be considered a minor artist, but covering the same theme and with more artistic effectiveness was Degas (1834-1917), although many of his sketchbooks were destroyed at his death. Better known for his paintings of the race course and the ballet. Degas executed about one hundred monotypes of brothel scenes. He referred to some of his art as "keyhole" art, and its eroticism is clearly evident.
Henri de Toulouse Lautrec (1864-1901) had much the same fascination with prostitutes as Rops and Degas, although he was more intrigued by the physical appearance of the brothels. Among his illustrations are the luxurious rooms in the better known brothels, as well as the torture rooms, which give another insight into brothel prostitution. Toulouse Lautrec was also fascinated with lesbianism and illustrates it with some of his studies such as the Kiss, or Two Friends. Much of his brothel art was not formally exhibited in his lifetime but was kept in back rooms for special purchasers— a fate that awaited many artists who turned to sexually explicit subjects.
Some examples of the art of this period are more titillating and erotic than others. The nudes of Renoir (1841-1919) seem to be more celebrations of female beauty than exploitations of women as sex objects for men. Similarly, the nudes and bathing scenes of Paul Gauguin (1848-1903) are not particularly erotic. Even when Renoir or Cezanne (1839-1906) use such classical themes as Leda and the swan, they are much less erotic than some of their predecessors. Vincent Van Gogh (1853-1890) produced three paintings of a nude girl sitting on her bed as well as three paintings of a nude girl reclining on her bed, none of which are particularly erotic. It seems that as nudity came to be more accepted as a fact of existence, what had once become eroticized became much less so. Instead, sexuality became more explicit, and several artists produced what might be called titillating work as a sideline to their major commissions. One such artist was Peter Fendi (1796-1842), the Austrian court painter, whose water colors show intercourse taking place in almost every position possible. Mihaly Zichy, who held a similar position in the court of Tsar Alexander II of Russia, produced a set of 40 prints entitled Love, tracing the sexual life of the artist from infancy to fatherhood. These pictures are much more delicate than those of Fendi, whose illustrations by comparison are almost crude.
Photography became an art form during the last part of the 19th century and the photographer often turned both to explicit sexual scenes and to sexual topics. E. J. Bellocq, a New Orleans photographer of the first part of the 20th century, spent much of his spare time documenting the life of the prostitute in the Storyville district of New Orleans. New art forms such as lithography also opened up new potentials for eroticism. One was the erotic picture postcard or souvenir card, many of them not suitable for mailing, issued by various commercial enterprises. The cards, whether engravings or touched-up photographic representations, came in the American idiom to be known as French postcards. The pre-20th century examples were what might be called innocently erotic, but the longer they remained on the market, the more explicit they became. By the 1930s, even overtly lesbian cards were on sale, although no cards depicted male homosexuality, since in the English commonlaw countries such representations were considered both illegal and obscene.
Even art forms that had remained less overtly sexual than others—such as sculpture, perhaps because it was usually done for wide public viewing—became more sexually oriented in the 20th century. Auguste Rodin (1840-1917), best known for his sculpture, at first turned to lithographs to illustrate both heterosexual and homosexual couples in intercourse. His eroticism, however, spilled over into his sculpture, particularly his own belief that women were violent and demanding creatures who wanted to possess the male. His viewpoint is most evident in his sculpture of Christ and the Magdalen, in which he depicted the nude figure of Mary Magdalene pressed against the nude Christ crucified on the cross in a clearly sexual embrace. Much of his later life was taken up with his project The Gates of Hell, which comprised individually sculpted figures demonstrating Rodin's vision of the terrors of physical passion.
Increasingly in the 20th century, artists were less likely to hide their erotic and sexual productions but rather to openly display and publicize them. Each generation of artists seemed to find a new way of expressing themselves. Thus, a number of 20th-century figures such as Pablo Picasso (1881-1973) and Henry Moore (1898-1986), two giants of 20th-century art, did explicit sexual work. Picasso felt that art and eroticism were the same. Depending on the progress of his love life, Picasso's productions varied from a lyrical, tender eroticism to a view of women as brutal, menacing, and destructive. In some of his engravings from the 1960s, Picasso appears as an old man watching a young couple engaged in sexual intercourse, a representation of the fantasies of an old man perhaps recalling his youth. Whereas Picasso was open in his eroticism, Henry Moore remained more traditional. He once told an interviewer, Peter Webb, that he had never set out deliberately to create an erotic work of art, but recognized that his subconscious was probably engaged in making many of his works erotic. He indicated he did not like to examine this aspect of his art and was content to regard his sculpture as an intuitive process. Much less reticent was the Norwegian painter and sculptor Edvard Munch (1863-1944), who spent much of the later part of his life sculpting the behavior of the human family in a park-like setting in Oslo. Much of it is explicitly sexual, although not particularly erotic.
Reticence about sex has not generally been a characteristic of most 20th-century artists, even if forthrightness got them into difficulties with the law or the public. Some seemed to be preoccupied with the erotic, such as Gustav Klimt (1862-1918) and Egon Schiele (1890-1918) were. Klimt was fascinated by the association of sexuality and death, as was Schiele. Both ran into difficulty over their avowed eroticism. The most heavily condemned of all Klimt's works were his ceiling decorations for Vienna University, which were commissioned and rejected by the university and destroyed by the Germans in 1945. The three huge oil paintings depicting philosophy, medicine, and jurisprudence portrayed a procession of starkly nude figures symbolizing varieties of human love and despair. Klimt also made a series of erotic drawings, as did Schiele, who was strongly influenced by him. In fact, Schiele's reputation as a pornographer resulted in his arrest and imprisonment for a time in 1912. He continued his work after his release and is generally recognized as the first major artist of the 20th century to produce a large body of frankly erotic art.
Sometimes sexual themes were used for shock purposes, at other times they were included simply because they were part of life. In the first quarter of the 20th century, for example, Dada was the fashion, and Marcel Duchamp (1887-1968) became famous when Anthony Comstock denounced his Nude Descending a Staircase. Comstock's attack was based more on the title than on the visible content, since Duchamp's picture combined cubism with a kind of iconoclasm known as futurism and was a different type of nude than that produced by Renoir. Dadaism, literally "nonsense," argued that no art could create anything as nonsensical as what went on in the world each day. The movement was short-lived, and its pieces were picked up and reconstituted by the surrealists, who added some of the Freudian ideas of the unconscious to their art. The surrealists set out to describe the aberrations and fantasies of mankind; because these elements were believed, following Freud, to be rooted in unconscious sexuality, most surrealist paintings were deliberately erotic. This was especially true in the works of André Masson (1896-1987), Salvador Dali (1904-1989), Max Ernst (1891-1976), and Andre Breton (1896-1966). Surrealism was in turn followed by pop art, represented in the United States by Larry Rivers (1923-), Tom Wesselman, and Andy Warhol (1927?-1987). Many pop artists viewed sexuality as a form of commercial exploitation. Movements, however, did not last long and often there were several. Also important in the 20th century was New Realism, the purpose of which was to achieve realism beyond that possible by photography by giving slices of absolute reality, specifically the erotic.
Art not only has mirrored the beliefs and assumptions of the time in which it was created, but it has often anticipated trends and developments. Because the artist is human, sexuality, whether conscious or unconscious, has always been an important element. In times of repression, this sexuality seems to be repressed, although it keeps breaking through into art. In the 20th century, as the importance of sexuality in the human personality has become a focus of major interest, artists themselves have become more openly sexual. This openness has often put the artist in conflict with society, not only in the past but also in recent years. In the early 1990s, the National Endowment for the Arts came under heavy criticism for supporting an exhibition by Robert Mapplethorpe that included photographs of homosexual activities, and even for indirectly supporting the performance artists Annie Sprinkle and Karen Finley, who appeared in the nude or engaged in explicit sexual activities on stage. The result of such criticism was presidential intervention and the firing of the director of the endowment. In spite of such setbacks, however, the artist in society has proven to be an accurate reflection not only of actual society but also of the hidden and secretive aspects of society, as well as an anticipator of trends and developments. One of the roles of the artist is to help us face up to ourselves, including our own sexuality.
REFERENCES
Anand, M. R. Kama Kala: Some Notes on the Philosophical Basis of Hindu Erotic Sculpture. Geneva: Nagel, 1962.
Bellocq, E. J. Storyville Portraits. Edited by John Szarkowski and reproduced from prints made by Lee Friedlander. New York: Museum of Modern Art, 1970.
Clark, K. The Nude. Bollingen Series. Princeton, N.J.: Princeton Univ. Press, 1956.
Étiemble, Yuh Yu: An Essay on Eroticism and Love in Ancient China. Geneva: Nagel, 1970.
Fendi, P. Forty Erotic Waterclors. New York: Arlington, 1984.
Grosbois, C. Shuhga: Essays on Erotic Elements in Japanese Art. Geneva: Nagel, 1964.
Hammond, P. French Undressing: Naughty Postcards from 1900 to 1920. London: Jupiter, 1976.
Hoyle, R. L. Checan: Essay on Erotic Elements in Peruvian Art. Geneva: Nagel, 1965.
Kronhausen, P., and E. Kronhausen. Erotic Art: A Survey of Erotic Fact and Fancy in the Fine Arts. New York: Bell, 1968.
Marcadé, J. Eros Kalos: Essay on Erotic Elements in Greek Art. Geneva: Nagel, 1965.
Marcadé, J. Roma Amor: Essay on Erotic Elements in Etruscan and Roman Art. Geneva: Nagel, 1965.
Melville, R. Erotic Art of the West. New York: G. P. Putnam's Sons, 1973.
Oullete, W., and B. Jones. Erotic Postcards. New York: Excalibur, 1977.
Smith, B. Erotic Art of the Masters: The Eighteenth, Nineteenth & Twentieth Centuries. New York: Lyle Smith, 1976.
Smith, B. Twentieth Century Masters of Erotic Art. New York: Crown, 1980.
Surieu, R. Sarva é Naz: An Essay on Love and the Representation of Erotic Themes in Ancient Iran. Geneva: Nagel, 1967.
Tucci, G. Rati-Lilà: An Interpretation of the Tantric Imagery of the Temples of Nepal. Geneva: Nagel, 1969.
Webb, P. The Erotic Arts. Boston: Little, Brown, 1976.
Vern L. Bullough
Sexuality is a powerful, pervasive force in life, and so it is in the arts. Images of nude bodies, sex organs, and erotic acts appeared in the Neolithic cave art of Africa and Australia. Carved phalli and images of fertility goddesses were part of public religious life in ancient Europe, Egypt, and the Near East. China, Japan, and India have long traditions of elaborately detailed erotic paintings and prints. Mochica pottery from ancient Peru shows coitus, fellatio, and anal intercourse. From ancient Rome to medieval India to modern America, poetry and fiction have described every aspect of erotic behavior and sexual relationship.
It would be possible to create a vast museum and library dedicated entirely to artistic renderings of sexuality. There are, in fact, library collections of art and literature and published anthologies of such works from around the world. Readers may find pleasure and enlightenment in consulting them (see References). Here we will limit ourselves mostly to Western culture and to how the arts can enlarge one's understanding of sexuality.
Unfortunately, sexuality textbooks so frequently misuse the arts that it is necessary to begin by saying what not to look for in them. Texts often state something like, "Painters and poets have always been brilliant observers," but fail to point out what artists have revealed that others have not. At most the textbooks proceed to use art merely as illustrations of social history or scientific findings. Actually, the arts are only partial, indirect sources of social history; the knowledge they do offer is unique and goes far beyond observations awaiting scientists' proofs.
Those who use the arts as social history may show such works as a Neolithic female figure, a Greek vase painted with erotic scenes, and an extract from the 18th-century erotic novel Fanny Hill. From these they blithely draw inferences about everyday sexual behavior and beliefs in the ancient Near East, ancient Greece, and 18th-century England. To see the flaw in this, one need only imagine an archaeologist excavating the ruins of, say, Indianapolis in the year 3000. He or she unearths three books - Hawthorne's The Scarlet Letter, Henry Miller's novel Sexus, and a conservative religious tract on "sexual hygiene." One can imagine the grotesque picture the archaeologist would draw of daily sex life in "ancient" America. Of course, the "ancient" Americans would not be there to laugh at it.
As this example suggests, most art does not reproduce common experience directly; usually it does not aim to. It selects details, is rich in fantasy and invention, and presents experience in condensed, symbolic ways. Even so-called realist art is a mixture of things observed and imagined, patterned in ways that make daily life seem chaotic and inconclusive by comparison. The arts may reveal something about sexuality in other times and cultures, but only when studied with caution and along with many other sources.
Artists' observations do sometimes presage scientific research. For instance, in the 1960s, Masters and Johnson discovered that during orgasm many or most people experience carpopedal spasm, a clutching or flaring of the fingers and toes. Centuries earlier, Japanese woodblock artists routinely included this detail in scenes of sexual pleasure.
One could cite other examples, but such details are not what make art convincing, let alone moving, insightful, and instructive. To emphasize them is to suggest that art is "soft" knowledge, a naive precursor of science waiting to be verified by "hard" data. To the contrary, good art is as precise as good science, and it contains unique, irreplaceable knowledge of a different sort. Some people fail to see this because they confuse accuracy with quantification and mistake art for vague emotion. Art, as the poet Ezra Pound said, is "news that stays news." It remains fresh and powerful because it captures people's inner reality with remarkable precision. It cannot be improved or superseded; new discoveries make it no less true. That cannot be said for most science. In fact, if permanence is the test, much art is "harder" than most science.
This does not trouble scientists. They know that most of their work is provisional; a new idea or a new measuring instrument can suddenly make today's accepted facts and theories obsolete. This is progress they welcome. They also know that science works by breaking reality into conceptual fragments that can be tested by replication and prediction. Like all approaches to knowledge, this one has its advantages and limits.
For instance, when science tries to understand so important a part of life as passionate attraction, it breaks reality into testable pieces. Its various branches would have to talk about visual cues, hormones, neurotransmitters, evolutionary trends, personality development, social scripts, communication, and mate selection. The results may be valuable, yet if these pieces are put together, they miss some important part of the original global experience. Compare with such findings what was written about passionate attraction by Sappho more than 2,500 years ago and by William Butler Yeats early in the 20th century.
... as I look at you my voice fails,
my tongue is broken and thin fire
runs like a thief through my body.
My eyes are dead to light, my ears
pound, and sweat pours down over me.
I shudder, I am paler than grass,
and I am intimate with dying—but
I must suffer everything, being poor.Sappho (Seventh century, B.C.E.)"A Last Confession"
Translated by Willis Barnstone
What lively lad most pleasured me
Of all that with me lay?
I answered that I gave my soul
And loved in misery,
But had great pleasure with a lad
That I loved bodily.Flinging from his arms I laughed
To think his passion such
He fancied that I gave a soul
Did but our bodies Couch,
And laughed upon his breast to think
Beast gave beast as much.I gave what other women gave
That stepped out of their clothes,
But when this soul, its body off,
Naked to naked goes,
He it has found shall find therein
What none other knows.And give his own and take his own
And rule in his own right;
And though it loved in misery
Close and cling so tight,
There's not a bird of day that dare
Extinguish that delight.W. B. Yeats
The poems will still be fresh, moving, and true to experience when the terms "neurotransmitter," "social learning," and "mate selection" have been replaced by more useful ones and are known only to historians of science. Unlike such efforts of science, poetry seizes and illuminates human experience in its rich complexity. As a result, people can find through the poems a keener sense of their own and others' lives, a crystallization of what they had vaguely sensed and perhaps tried in vain to express.
The knowledge in these poems cannot be translated into science or even into other arts. If it could be expressed by data or in visual imagery or music, it would have been. For that reason, the experience of seeing Rodin's The Kiss, Michelangelo's David, or the erotic sculpture of medieval Indian temples must remain a visual event, beyond words. An essay such as this one can deal best with art in words, the arts of poetry and fiction.
Literature, fortunately, is rich in understanding of sexuality. It speaks with exquisite precision and detail about the entire range of erotic feelings, events, and relationships. Here are only some of the better known works in Western literature that should be seen as primary sources of knowledge about sexuality in all its expressions:
· Obsessive romantic love, with all its contradictions, has never been described more vividly than by the Greek poetess Sappho and the Roman poet Catullus. No one has captured better the kind of frenzied yearning that grows when it is frustrated or denied.
· No scientific or literary study of prostitution has captured whores, their trade, and their clients as well as the Roman poet Juvenal, in his Satires, and the Russian writer Aleksandr Kuprin, in his novel Yama. Their portraits are unjudging yet unsparing, and remain as lively and immediate as when they were written.
· Chaucer, in Troilus and Cressida, subtly depicts the unintentional betrayal of love. Shakespeare's Othello contains literature's greatest portrayal of the twin passions, envy and jealousy.
· Leo Tolstoi's long, ironically titled story A Happy Marriage is a harrowing account of the pain two people can inflict on each other from need and fear.
· In Pride and Prejudice, Jane Austen explores the power of social convention to shape love and courtship. In Madame Bovary, Gustav Flaubert shows how romantic fantasy can cripple marriage and destroy lives.
· Benjamin Constant's novel Adolphe and Ivan Turgenev's novella First Love are moving accounts of the clash of adolescent passion with adult realities.
· Henry James's novel The Bostonians recounts in subtle detail the struggle between a militant feminist and a traditional man for a pliant young woman. It remains a classic picture of the psychological and social claims on a woman's commitment.
· Vladimir Nabokov's novel Lolita, whose protagonist is drawn irresistibly and exclusively to pubescent girls, tells as much about sexual obsession as any clinical study, and more.
· James Baldwin's novel Another Country captures the nexus in our society of conflicts over race and sex—between white and black, man and woman, heterosexual and homosexual.
Any such list is bound to be partial and somewhat arbitrary. Even a limited library of major writers who have distinctly enriched our knowledge of the sexual experience would also include the poets of The Geek Anthology, Anton Chekhov, Collette, E. E. Cummings, John Donne, James Joyce, D. H. Lawrence, Martial, Henry Miller, Marcel Proust, Theodore Roethke, Stendhal, Arthur Schnitzler, Junichiro Tanizaki, and many poets of ancient China and medieval India.
Clearly, literature, the visual arts, and cinema are not merely adornments of the study of sexuality; they are primary sources of knowledge. They provide discovery and illumination not found anywhere else. They clarify some of the experiences that most powerfully shape our lives - of being male or female, in or out of love, ecstatic or repelled or indifferent. They do so best about matters science is still struggling to apprehend.
REFERENCES
Cole, W. Erotic Poetry. New York: Random House, 1963.
Evans, T., and M. Evans. Shunga: The Art of Love in Japan. New York: Paddington/Gosset & Dunlap, 1975.
Fouchet, M. The Erotic Sculpture of India. New York: Criterion, 1959.
Lucie-Smith, E. Sexuality in Western Art. New York: Thames & Hudson, 1991.
Marcadé, J. Eros Kalos. Geneva: Nagel, 1962.
Merwin, W., and J. Masson. Sanskrit Love Poetry. New York: Columbia Univ. Press, 1977.
Packard, W. Desire: Erotic Poetry Through the Ages. New York: St. Martin's Press, 1980.
Rawson, P. Erotic Art of the East. New York: Putnam's, 1968.
Reynolds, M. Erotica: An Anthology of Women's Writing. London: Pandora, 1990.
Arno Karlen
Asexual reproduction is the ability of an organism to produce offspring without the union of sex cells (i.e., gametes). There are many methods to accomplish this. Asexual reproduction probably occurred before sexual reproduction in the evolutionary history of the earth. Sexual reproduction is the union of two gametes, which may be from the same or from different parents. It need not involve the use of specialized organs.
Some plants and animals, such as many algae and protozoans, produce their offspring by simply splitting into two (fission). Many algae and almost all fungi produce huge numbers of specialized asexual spore that reproduces large populations of the organism. Others, such as yeasts and hydra, may produce unicellular or multicellular buds from the parent cell or adult organism. Individual tiny plantlets may be produced on the leaves of some plants (e.g., kalanchoe), and others may produce new individuals vegetatively from a plant part, such as a leaf or a stem (e.g., African violets), that has reached the proper environmental conditions necessary for growth. Multicellular invertebrates may produce offspring from parts that have been broken off of the parent body (e.g., the arm of a starfish). Grafting is a method to attach a part (the scion) of a desirable plant to a more robust root system (the stock). This method is often used to propagate desirable apples and other fruits. Some organisms produce offspring from unfertilized eggs. In animals, this is called parthenogenesis and occurs in aphids, among others. The process is called agamospermy in plants; the most common example is the dandelion. Cloning is the process in which the parts of a desirable organism are used to asexually reproduce a large population of that organism. All of these methods of asexual reproduction produce offspring identical in those characteristics that are genetically inherited.
The selective evolutionary advantage of asexual reproduction is that huge populations of genetically identical organisms can be produced quickly and without a mate. Thus, an organism can quickly spread throughout a favorable environment. A major disadvantage is that there is no recombination of genetic material, such as occurs in sexual reproduction, and thus there are fewer inherited characteristics upon which the environment can act.
In humans, the only occurrence that could be defined as asexual reproduction is when the zygote splits and produces identical (monozygotic) twins. The zygote results from the union of an egg and a sperm; when it splits, it produces two individuals who are usually genetically identical. This fact has been used by science fiction writers, notably George Orwell in his book 1984. All other forms of human reproduction are sexual. Various methods of getting the egg and sperm together (e.g., in vitro fertilization) have been developed, but the union of egg and sperm, the definition of sexual reproduction, remains constant.
REFERENCES
Arms, K., and P. Camp. Biology. Third Ed. Philadelphia: Saunders, 1987.
Curtis, Helena. Biology. Second Ed. New York: Worth, 1975.
James D. Haynes
Near the end of the 19th century, the pioneering sexologist Havelock Ellis popularized the word "autoeroticism" and defined it as "the phenomena of spontaneous sexual emotion generated in the absence of an external stimulus proceeding, directly or indirectly, from another person." Ellis's definition excludes sexual arousal that occurs in the presence of a beloved person, any sexuality involving someone of one's own sex, and any involving erotic fetishism of any kind. Other authors had previously used such terms as autoerastia, geistige Onanie, onania psychica, monosexual idiosyncrasy, autophilia, self-abuse, and Onanism. Ellis proposed his new word after concluding that all of those in previous use were either erroneous in concept or inadequate in covering all activities he thought should be included in the category for its proper understanding.
Ellis's purpose in making those distinctions was to cast a clearer light on a category of sexual responses that were little understood but that had much in common. To more fully satisfy that purpose, sexologists today generally take a broader approach than did Ellis and define autoeroticism to include erotic responses that occur in an individual in the absence of tactile stimulation emanating from physical contact by or with another person or other animate body. Some authorities say it simply means sexual responses emanating from one's own organism.
The most discussed form of autoeroticism is masturbation. As such, some people tend to consider autoeroticism and masturbation one and the same. Yet, there are many autoerotic manifestations that are not properly described as masturbation.
The human body is capable of experiencing erotic arousal from birth to death. Indeed, some authorities say they have observed fetuses in utero engaging in activities they conclude produce erotic responses in the fetuses. In addition to there being no age for erotic responses to occur in humans, it also appears that the stimuli that elicit an erotic response in one or another person may come from a variety of sources. Many of those stimuli may be self-induced or may occur spontaneously—thus the importance of conceptualizing this category of erotic responses.
When such a self-induced or spontaneous stimulus event occurs to a person who is physically, and perhaps, though not necessarily, psychologically, susceptible to its erotic potential, an auto erotic response is likely to occur. Besides masturbation, one of the most common of autoerotic responses is that which occurs during sleep. That phenomenon has been the subject of much study, contemplation, and consternation throughout history.
Biblical pronouncements indicate that the ancient Jews considered the expulsion of semen during sleep an impurity, and the impure one was commanded to wash his clothes and body and consider himself unclean until the evening. But even earlier, the ancient Egyptians and Babylonians had also wrestled with the occurrence. The Egyptians felt that semen was a life force that when wasted (i.e., used for any purpose but procreation), was not only a drain on the offender's system, but also a pollution of the universe.
The Babylonians explained orgasms during sleep as being the work of a "maid of the night" who visited men during sleep and of a corresponding "little night man" who visited women during their sleep. The Egyptian/Jewish notion of "pollution" carried over to Christians who treated it only slightly less alarmingly than they did voluntary masturbation; in the Middle Ages, they blamed it on the devil, who sent a succubus to lie under men and an incubus to lie upon women.
It is now known that orgasms during sleep are normal, harmless occurrences (as is the perhaps more common phenomenon of erotic dreams that do not necessarily lead to orgasm). In females, the result of such an event is often vulval vasocongestion and vaginal lubrication, and at times orgasm. In the male, the result is often erection of the penis, and at times ejaculation. This is known to most often occur during periods of the sleep cycle known as the rapid eye movement (REM) phase, which normally occurs about every 90 minutes during sleep.
Another form of auto erotic activity similar to erotic dreams during sleep is erotic daydreams (i.e., conscious erotic thoughts and fantasies occurring while awake). These may or may not lead to orgasm, which may occur in some people without any direct physical stimulation of their body.
A variation of erotic daydream is the occurrence of erotic responses in some people that result from visual, psychic, tactile, or auditory stimuli of a nature that is not perceived by the person (nor perhaps by others) as erotic. Examples of this type of autoeroticism are the experiencing of a heightened state of erotic arousal, and perhaps but not necessarily an orgasm, while listening to certain music, while contemplating a pleasing landscape or artwork, while involved in a dangerous or even life-threatening situation, or while engaged in religious reverie. There are many other possible experiences that may precipitate or accompany such a response in a person so inclined.
In contrast to the other forms of autoerotic activities, masturbation is by definition the erotic stimulation of one's own body (usually of the genital organs), commonly resulting in orgasm, achieved by manual or other bodily contact (exclusive of sexual intercourse) and/or by instrumental manipulation.
The word "masturbate" entered the English language around 1785. It was borrowed from the Latin masturbari, meaning to rub or to agitate by hand; the negative connotation ascribed is "defiling by hand." It joined and gradually superseded, at least in most of the developed world, other terms for the activity; most meaning some form of self-abuse or self-gratification, and all having quite negative implications.
Ancient Egyptian, Greek, and Roman civilizations were either mildly negative or almost indifferent about male masturbation. In each of those ancient cultures, there appears to have been little or no concern about female masturbation. In fact, masturbatory aids for females in the form of what are today called dildoes (i.e., objects resembling the male penis) were in quite common use.
Knowledgeable sexologists today have given clear and unambiguous evidence that masturbation, whether or not resulting in orgasm, when performed in a way that is not intentionally or inadvertently designed to injure the body is not harmful to the body in any way and that the act, by itself, causes no mental pathology. However, there remains in Western cultures a strong and pervasive residual of fear and ignorance concerning the supposed harmful effects to the individual who masturbates. The traditional Judaeo-Christian abhorrence of masturbation springs from the biblical prohibition against men "wasting" their seed. Strong strains of that negativity are still pervasive in modern Western society.
Prior to the 18th century, Western cultures saw masturbation as primarily a matter to be handled by religious dogma. However, the Christian, and particularly the Protestant, churches of those times were not inclined to give it much notice. As a result, in areas of the world controlled by the Christian churches, the practice of masturbation was practically a nonissue.
Then, in 1760, a Swiss physician named Tissot published the book Onanism, or a Treatise Upon the Disorders Produced by Masturbation. In one fell swoop it convinced much of the world that not only was masturbation a sin and a crime, it caused an enormous number of diseases and illnesses in those who practiced it.
Quickly, the medical profession became the loudest champions of the anti-masturbation crusade. Physicians in increasing numbers began attesting in books, journals, and monographs as to the myriad mental and physical disorders that were, without question, caused by masturbating. The list of maladies grew until there was hardly a serious affliction of mind or body, including insanity and death, that some medical authority had not ascribed absolutely to the "solitary vice." Remedies prescribed for offending children and adults ranged from special diets, loose clothes, and various forms of bondage, to surgery on the genitals and commitment to insane asylums.
The sound and fury reached its zenith during the Victorian years. In the latter part of the 19th century, medical authorities began to apply reason and to understand that masturbation, per se, is a benign, even at times beneficial, normal, and natural activity. That opinion is also now shared by many Christian religious denominations.
The percentage of people in a given culture or subculture who masturbate varies. However, researchers believe that in many Western societies only a small percentage of males and females have never masturbated and in general agree that more females than males have never done so.
Although masturbation, per se, in no way harms the person who engages in it, there is the possibility that the way in which it is performed may cause adverse physical consequences.
The almost infinite variety of methods that can be used in attempts at erotic self-stimulation inevitably include some that may harm the body of the person using them. These may involve injuries to the tissue of the genital area by excessive or too forceful rubbing or thrusting; injuries caused by inserting objects into the urethra or anus; the misuse of electrostimulation; and the ingestion, injection, or inhalation of harmful compounds thought to enhance one's response to self-stimulation. Autoerotic fatalities have resulted from accidental autoasphyxia while intentionally constricting the carotid vessels in one's own neck, from suffocation while wrapped in plastic or blankets, from the inhalation of various gases, from electrocution, from exposure, and from poisoning. It is estimated that in the United States and Canada, there are between 500 to 1,000 accidental autoerotic deaths a year.
REFERENCES
Ellis, H. Studies in the Psychology of Sex. New York: Random House, 1936.
Haeberle, E. J. The Sex Atlas. New York: Seabury, 1978.
Masters, R. E. L., ed. Sexual Self-Stimulation. Los Angeles: Sherbourne, 1967.
Dwight Dixon
Joan K. Dixon
![]()
![]()
![]()
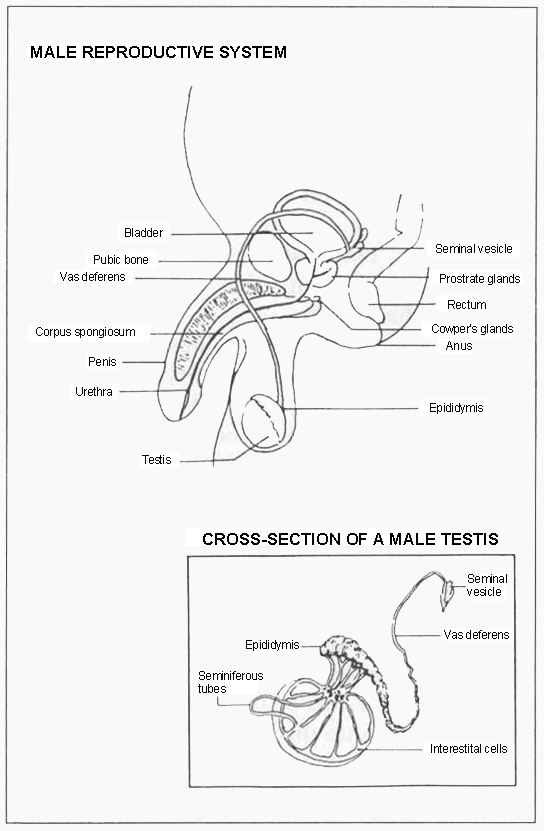{kind=link}
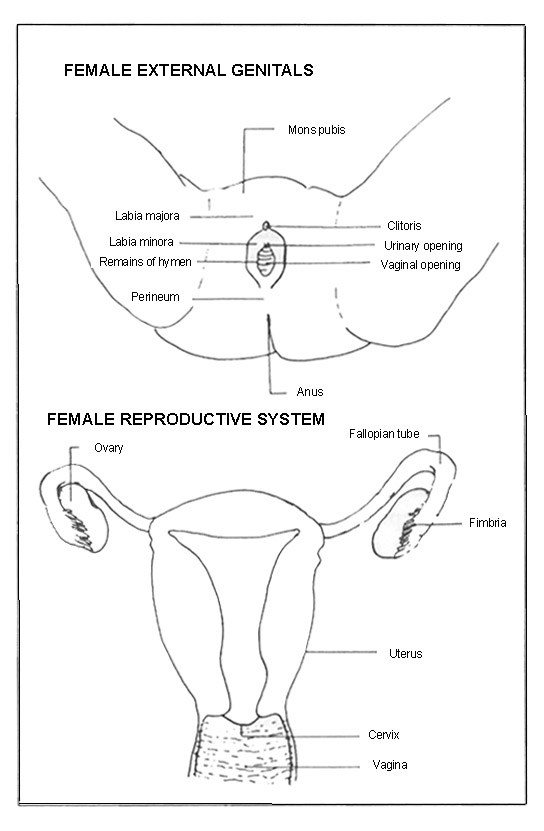{kind=link}