![]()
![]()
![]()
Demographics, a Historical Perspective, and Dutch Sexology
1. Basic Sexological Premises
2. Religious and Ethnic Factors Affecting Sexuality
3. Sexual Knowledge and Education
4. Autoerotic Behaviors and Patterns
5. Interpersonal Heterosexual Behaviors
6. Homoerotic, Homosexual, and Ambisexual Behaviors
7. Gender Conflicted Persons
8. Significant Unconventional Behaviors
9. Contraception, Abortion, and Population Planning
10. Sexually Transmitted Diseases
11. HIV/AIDS
12. Sexual Dysfunctions, Counseling, and Therapies
13. Research and Advanced Education
References and Suggested Readings
(Koninkrijk der Nederlanden)
Jelto J. Drenth, Ph.D., and A. Koos Slob, Ph.D.*
* This chapter draws extensively from the 1991 Special English Issue of the Tijdschrift voor Seksuologie, published on the occasion of the Tenth World Congress for Sexology, Amsterdam, June 18-22, 1991. We gratefully acknowledge the authors of this volume and the editors for their kind permission.
A. Demographics
Located in northwest Europe on the North Sea, the Netherlands’ 15,770 square miles are roughly the size of the states of Massachusetts, Connecticut, and Rhode Island combined. Belgium borders the Netherlands on the south, Germany on the east, and the English Channel and the United Kingdom on the west. The Kingdom of the Netherlands includes the Dutch Antilles, the autonomous Caribbean islands of the West Indies. Curacao, Aruba, and Bonaire are near the South American coast; St. Eustatius, Saba, and the southern part of St. Maarten are southeast of Puerto Rico. (The northern two thirds of St. Maarten island belongs to French Guadaloupe). Combined, the six islands have an area of 385 square miles.
Over 88 percent of the 15.4 million Dutch live in cities. Life expectancy at birth in 1995 was 75 for males and 81 for females. The 1995 birthrate was 12 per 1,000 and the death rate 8 per 1,000, with an annual natural increase of 0.4 percent. The infant mortality rate was 6 per 1,000 live births. Age distribution is 18 percent for those under the age of 14; 15 to 64, 69 percent; and 65 and over, 13 percent. The Netherlands has one hospital bed per 172 persons and one physician for 400 persons. The per capital domestic product in 1995 was $17,200.
B. A Brief Historical Perspective
In 55 B.C.E., Julius Caesar conquered the Celtic and Germanic tribes that inhabited the region that is now the Netherlands. After Charlamagne’s empire fell apart in the mid-800s, the Netherlands, then what is today Holland, Belgium, and Flanders, was divided among dukes, counts, and bishops. Holland soon passed through the Duke of Burgundy to King Charles V of Spain. In the later 1500s, as the area drifted toward political freedom and Protestantism, William the Silent, prince of Orange, led a confederation of the northern provinces that declared independence from Spain in 1581. The United Dutch Republic’s rise to naval, economic, and artistic eminence came in the 17th century, only to end in 1795 when Napoleon made his brother Louis king of Holland. Napoleon annexed the country in 1810, but the French were expelled in 1813 and the kingdom of the Netherlands, including Belgium, established. The Belgians seceded and formed a separate kingdom in 1830.
The Netherlands remained neutral in World War I, but was invaded and brutally occupied by the Germans between 1940 and 1945. After several years of fighting, Indonesia gained its independence in 1949; West New Guinea was turned over to Indonesia in 1963. The independence of former Dutch colonies was followed by mass emigrations to the Netherlands.
C. Dutch Sexology
To understand Dutch sexology, one needs to keep in mind five general characteristics of our society that crystallized in the latter half of the nineteenth and first half of the twentieth centuries:
1. The role of the family and the position of men and women is central in Dutch society. Excluded from the labor process, women were supposed to derive their task, fulfillment, and satisfaction from marriage and family. Together with Ireland and Sicily, the Netherlands has the lowest rate of working wives and economically independent women. Even today, many politicians support this inequality of social roles. In recent decades, however, the position of the housewife has gradually declined, a factor that may impact on sexual problems for women and men.Research on sexual behavior, attitudes and related subjects began in 1968, when the largest women’s weekly, Margriet, commissioned a national Seks in Nederland (SIN) survey using a representative sample of 1,284 men and women, ages 21 to 65, and 809 youngsters ages 16 to 20 (Noordhoff et al. 1969). This study was repeated in a modified and extended way in 1974 (with teenagers only) and in 1981 and 1989. These surveys present a fairly accurate description of major social and demographic correlates of sexual attitudes and behavior, and the changes in these variables over time.2. Since the origin of the Netherlands in the seventeenth century, there has been a strong segregation between Catholicism and Protestantism, with many subdivisions among the latter. In the nineteenth century, humanism, socialism, and liberalism were influential. As a result, the Netherlands now has a very strong compartmentalization or “denominational segregation.” Some forty different organizations and over twenty-five political parties have access to television broadcasting and the elections. Due to different, sometimes very powerful religious influences, extreme contrasts in social and sexual behavior exist between various groups. For instance, one fundamentalist Protestant political party still discriminates against women in membership and office eligibility, although over half of those voting for this party are women. On the positive side, this compartmentalization has resulted in a willingness to cope with differences in opinion and a rather liberal attitude towards varying social groups and lifestyles. The pedophile movement, for example, openly expresses its views on child-adult sexual relations. Our homosexual movement is widely respected, and our national organization for homosexuals even received royal assent. The Protestant University of Amsterdam houses the world’s only chair of transsexology.
3. Holland, in the west, was rich and industrialized with extensive colonial ventures; the east was less prosperous and mainly agrarian. The west is the focus of political, economic, cultural, and social development, including a large group of sexologists. This geographic separation also influences differences between groups in Dutch society.
4. When the Dutch East Indies became independent Indonesia in 1949, several hundred thousand people came from this culture to the Netherlands. A similar immigration occurred in 1975 when Dutch Guiana became independent Suriname. The Netherlands has also received its share of labor from the Mediterranean. A second and third generation of Turkish and Moroccan origins, most born in the Netherlands, still struggle with the problem of being rooted in two cultures. Political refugees are the latest contribution to our multi-ethnic society. Some 7 percent of our population was born in other countries. The result is a profoundly multiracial society in which sexual rules and values sometimes differ greatly, presenting a major challenge for sexological research and treatment.
5. Sociosexological research in the Netherlands has been quite extensive since the 1960s. Initial research focused on problems resulting from a restrictive sexual morality. During the 1970s, attention shifted to the rapid process of sexual liberalization and its practical consequences, such as the need for family planning education and services. The past decade has been dominated by research on sexual abuse and the spread of STDs and AIDS. Published mostly in the Dutch language, this research has not had a significant impact outside Holland, despite the fact that open and permissive sexual attitudes give Dutch sexology a unique position, not just in terms of attitudes and behavior, but also in terms of research possibilities. More international comparative and collaborative research would benefit all.
While strongly inspired by the 1948/1953 Kinsey studies, the 1968 Dutch study reflected the main interests and concerns of Dutch society at that time, namely self-pleasuring, premarital and extramarital sexual contacts, sexual desires, prostitution, homosexuality, contraception, and (illegal) induced abortion.
Kooy (1975) analyzed the 1968 SIN-survey, putting the data in a theoretical perspective of changing family relationships, declining moral influence of religion, and growing social equality between the sexes. The second SIN-survey (in 1981) had the character of a trend report (Kooy et al., 1983). The main trends observed were growing tolerance towards different kinds of sexual behavior and more equality between partners in heterosexual relationships. Secularization seemed to be the most important background factor in these changes. The 1989 survey was strongly influenced by fear of AIDS and a need for knowledge to underpin prevention programs.
In part, the study of adolescent sexuality parallels the adult studies, including sexual development, relationship development, sexual education, prevention of unwanted pregnancy, and induced abortion, and recently STD and AIDS prevention. In 1974, the first SIN-survey was repeated for adolescents only. De Haas (1975) interpreted and reported the data from an educational view point; Kooy (1976) used a sociological perspective. The 1981 adolescent data were not analyzed before they were used in the framework of the much larger 1989 study (Vogels and van der Vliet 1990). The 1974 and 1981 studies included 600 and 800 youngsters, ages 15 to 19, while the 1989 study included 11,500 youngsters and 11- to 14-year-olds. Finally, both the 1989 adolescent and 1989 SIN adult surveys were motivated by the fear of the HIV epidemic.
A. Character of Gender Roles
It is difficult to generalize on gender roles in the Netherlands. Dutch society has become so diverse that, at any given moment, different groups will be influenced differently. Yet, in all but the most isolated groups, an awareness of the variation in social and sexual role responsibilities must have led to a rise in tolerance for less-conventional behaviors.
The classic Western role separation, men being providers and women housekeepers and care givers has been criticized intensively. Some feminist principles have found almost universal support. Holland is subject to Europe’s legislation against sex discrimination, and today it is hard to find examples of sex discrimination in the workplace. Government policy includes a “positive action” plan: in some segments of paid labor, women will be favored in the job-application process to bring down the underrepresentation of women in these professions. The government has funded a mass-media campaign intended to raise girls’ awareness of preparing for financial independence.
Countering these conscious efforts, mass-media influences, such as soap operas and commercials, are often extremely conservative in their depiction of role ideals. The impact of this on the general public’s role awareness is hard to estimate.
B. Sociolegal Status of Males and Females
In recent years, legislation reforms have tended to equalize legal rights for men and women, homosexuals and heterosexuals. For instance, a 1991 reform of rape laws encompassed male and female rape. Children under age 12 are protected against all sexual contacts; for 12- to 16-year-olds, sexual contacts are legal offenses only if the adolescent, his/her parents(s) or guardian, or the Child Welfare Court files a complaint. Existence of a dependency relation between the adult partner and the adolescent is an exception to this. The law’s intention is that the child’s own judgment outweighs the parent’s.
In the Netherlands, bypasses are available for teenagers to obtain oral contraceptives and abortions without parental permission.
C. General Concepts of Sexuality and Love
As oral contraception has uncoupled sexuality and procreation, so the possibility of uncoupling sexuality and love has also been recognized. Large groups of Dutch men and women sympathize with the need for sexual gratification of people who are not in steady relationships. Self-pleasuring and “recreational” sex are no longer taboo. Virginity is disappearing as an ideal. Self-pleasuring as a variation within a steady relationship is also no longer universally scorned.
Yet love is still probably the most-valued principle in Holland. Almost all Dutch men and women believe that steady relations must be built on love, and that sexuality with love is more satisfying that without it.
A. Source and Character of Religious Values
Denominational segregation, 34 percent Roman Catholic and 25 percent Dutch Reformed, has not played an important role in Dutch sexuality. The Dutch Society for Sexual Reform (NVSH) found its Protestant counterpart in the Protestant Society for Responsible Family Planning (PSVG) and a Catholic Bureau for Sexuality and Relations. But these religiously inspired organizations are small and limited to providing written information and educational materials. NVSH has separated into a lay persons’ organization for political action and education, and a professional organization, the Rutgers Foundation, for medical and psychological help. The Dutch government funds the foundation’s counseling centers and participation of foundation administrators and staff in international organizations, such as the International Planned Parenthood Federation.
Religious motivations have played an important role in our legal reform. The Dutch abortion law adopted in 1985 permits abortion on request with the sole restriction of a five-day waiting period. Opposition from fundamentalist Catholics has little support. Moreover, the Pope’s regulations on contraception is almost universally ignored by Dutch Catholics, as are restrictions on homosexual behavior and the sexuality of the handicapped. Catholic and Protestant groups have played important roles in the acceptance of gays and lesbians, with some churches celebrating ceremonies of gay and lesbian unions. (Legal marriage is not available for homosexual couples in Holland.)
B. Source and Character of Ethnic Values
Most Muslims in the Netherlands came from Turkey or Morocco as “guest laborers” in the booming economy, women and children following the men after they settled in. The Netherlands now has a second generation and a third on its way. Tension between Muslim traditions and the Western way of life is common. Islamic traditions emphasize family honor, with specific restrictions on sexual behavior and distinct social roles for men and women.
Arranged marriages are common and the confrontation of two cultures sometimes leads to conflicts between parents and children who, raised in the Western world, want to choose their own spouse. Muslim tradition includes the ultimate measure of kidnapping to force a marriage. Incidents of this, and of Muslim girls running away from home to avoid an arranged marriage, are common, leading to the establishment of a shelter home for Muslim girls only. Muslim honor sometimes conflicts with the Dutch legal system, leading to tragic misunderstandings in the law courts. Helping professionals are only slowly learning how to handle such problems without trespassing on Muslim taboos. Relevant for sexological practice are the following:
· A male doctor will not be allowed to perform a physical examination of a Muslima in the absence of her husband;Comparative research data on the influence of religious background on sexual topics include:· A male patient will often be embarrassed if asked about his sexual problems by a female doctor;
· Self-pleasuring is an almost-absolute taboo and should not be advised as a therapeutic modality;
· Prostitution is much less forbidden for Muslim men; and
· Direct communications are uncommon - a metaphorical presentation of the most distressing problems, infertility and erectile failure, is the rule.
· Muslim adolescent boys commonly initiate all types of sexual activity earlier than their Christian and nonreligious male and female peers; Muslim girls are considerably less experienced;While incidence figures for induced abortion are generally low in the Netherlands, some ethnic groups have a higher risk of unwanted pregnancy and abortion (see Section 9). Among autochtonous* women, unwanted pregnancy is mostly due to contraceptive method failure; among Caribbean, Mediterranean, and refugee women, nonuse or inconsistent use of contraceptives is the more likely cause. A 1990 study of unwanted pregnancy among Caribbean women (Lamur et al.) identifies three groups with distinguishing attitudes towards contraception:· Christian and nonreligious adolescents tend to prefer sex in steady relationships, Muslim adolescents tend to have more casual sexual experiences and less steady relationships;
· Attitudes toward premarital sex in steady relationships are more accepting in Christian and nonreligious adolescents (80 percent) and less so in Muslim adolescents (40 percent). Muslima are very restricted.
· Muslim adolescents tend to advocate abstinence as the best way to avoid HIV infection, and are less willing to use condoms for this purpose (Sandfort and van Zessen 1991).
The problems of political refugees have not yet been researched. Dutch Amnesty International workers have some experience with the atrocious problems of sexual torture and humiliation some refugees have experienced.*Note: In Dutch sociology, “autochtonous” means “of Dutch descent,” including Dutch nationality, Caucasian, and raised in Western traditions. “Allochtonous” includes immigrants and their next generations from former Dutch colonies, immigrants from Mediterranean countries who came to Holland seeking work in the 1960s and 1970s, and political refugees from all over the world.· Among women born in the six Caribbean islands, the strongest influence on sexual attitudes and practices is the Roman Catholic Church. Information on sexuality is extremely scarce. Strong negative moral and practical feelings toward contraception are common. The pill and IUD are often seen as severe health hazards; when used, physical complaints are common.· Creole women from Suriname (formerly Dutch Guiana) also have little access to sexual information, but this is changing for Creole women born after 1960. In this younger group, middle-class women from stable families are mostly highly career-oriented and very concerned about unwanted pregnancy. Lower-class women are often familiar with a pattern of single women having children with fathers who are more or less distant. Among middle-class Creole families in the Netherlands, sexual information is more adequate and attitudes towards sex and protection less taboo-burdened. Yet these women are less constant in their choice of contraceptive methods and tend to have more physical complaints when using the pill. For all Creole women, abortion is not an easy solution for unwanted pregnancy. Despite a high abortion rate in this group, moral restraints are strong and abortion is definitely not seen as a normal contraceptive method.
· Hindustani women of Suriname descent have very strict family rules, and honor (Izzat) is a leading principle. Premarital sex is an absolute taboo. Education is highly valued and often considered part of a girl’s dowry. In recent years, information on sexuality and contraception is provided to Hindustani girls, but effective premarital contraceptive use is rare. A sex taboo seems to prevent information from being absorbed adequately for practical use.
A particular problem causing some public discussion is clitorectomy. A modified form of clitorectomy, incision of clitoral prepuce, has been under consideration as a result of requests mainly from Somalian women. The Dutch government recently prohibited all forms of clitoral mutilation. Incidentally, Islamic and Hindustani women commonly consult Dutch gynecologists for hymen reconstruction, as part of preparation for marriage.
A. Government Policies and Programs for Sex Education
The Netherlands has the lowest rate of unwanted teenage pregnancies of all the industrialized nations. Some attribute this to a relatively effective use of contraceptives, especially the pill, among teenagers. This effective use is explained, at least in part, by a pragmatic and liberal attitude towards sex education, the high quality of information and education on sex and contraception in secondary schools and the mass media, and the wide availability of confidential and low-cost contraceptive services.
These results, however, are no reason for self-satisfaction or complacency. For one thing, contraceptive behavior among ethnic minorities and young adolescents is still ineffective, and the abortion rate among adolescents is still about 45 per 100 pregnancies. In terms of AIDS, about half of the sexually active teenagers appear to engage in risky behavior.
The Dutch government finances a number of sexuality organizations, including the Netherlands Institute for Social Sexological Research (NISSO), the Rutgers Foundation for contraceptive information, sexological education, and STD prevention, and the Foundation for the Study of STD. Recently, the government policy has tried to integrate these special service organizations into the general health institutions. The Rutgers Foundation, which has for decades provided the easiest access for teenagers to contraceptive information, has been forced to concentrate its services in seven offices in large cities and start a training program to share the foundation’s specific knowledge and skills with physicians, mental-health workers, and educators.
In recent years, the government has strongly encouraged and promoted prevention programs. Health promotion is now obligatory in secondary schools, even though traditionally Dutch schools have formed their own curricula. Numerous educational courses and an amalgam of materials on sex and AIDS have been developed by several local and national organizations. Special materials have been developed for Catholic, Protestant, and nonreligious schools. Despite underlying philosophical differences, most of these programs are very similar in terms of goals, methods, and materials.
On a national level, knowledge of the proportion of schools providing sex and AIDS education, what teachers teach, and what methods and materials they use is limited. A late 1980s survey suggests that some sex and AIDS education was provided by about 85 percent of the Dutch secondary schools, generally by hygiene or biology teachers. The major topics covered were biological-physiological aspects of puberty and unwanted pregnancy. Topics such as intercourse and sexual desire received lowest attention. As for AIDS education, practical guidelines for reducing risk were the main topics covered, along with attitudes towards homosexuality. The way teachers covered these topics, however, varied widely, depending on the teacher’s area of expertise and teaching methods. Biology-hygiene teachers seemed to focus on transmission of knowledge of biological and physiological aspects. Sociology teachers and counselors seemed to emphasize relational aspects, such as gender-role patterns, cohabitation patterns, friendship, sexual orientations, and being in love.
Eighty percent of Dutch secondary schools offer a mean of four to five hours of AIDS education. Forty percent use one of four AIDS courses developed for national use on AIDS, though often not according to the specific methodological guidelines. More time is devoted to knowledge transfer than to training in social skills. Teachers were not sufficiently trained or supported to implement these courses, and the materials are not tailored to normal school practices.
Criticism of teachers’ training in providing sex and AIDS education is widespread. Yet there was for some years in the mid-1980s, a three-day in-service postgraduate course for secondary school teachers, during which about 500 participants were trained (Schraag 1989). A unique feature of this course was that teachers and pupils worked together to express their underlying convictions and wishes about sex education in school and to develop a program for sexual education. The course program and contribution of the trainers have been evaluated on many occasions, leading to continuous adjustments and corrections.
Although it is frequently argued that health education should be a systematic process, most sex-education courses and materials have not been developed in a systematic way. Very few consider behavioral determinants, and little is known about the effectiveness of the various courses and materials. Besides, only two of the evaluative surveys on sex and AIDS-education classes have used an adequate experimental design. Both surveys concluded that the courses under scrutiny produced only an increase in knowledge and minor changes in some attitudes, results similar to evaluations of United States sex education programs and the more general results of health education. Besides knowledge transfer, health education should offer students the opportunity to involve their social environment and develop skills necessary for an adequate performance of the desired behavior. In the 1990s, organizations responsible for implementing educational innovations in health and sex education were encouraged to cooperate with groups responsible for development of educational programs (Kok and Green 1990). Future research should clarify how interventions based on behavioral-science theories can improve diffusion and adoption of health education programs.
Government-financed mass media campaigns are an important means of educating the public. In 1987, the first campaign to alter social norms of condom use focused on a number of Dutch celebrities who use condoms themselves. In 1988, a second campaign focused on “Safe Sex for Holidays,” followed in 1989 by ironically confronting 18- to 24-year-olds with irrational beliefs and popular excuses for risky behavior. “Sleep well” was the final comment on each poster and the campaign’s title. A pretest/posttest evaluation proved that the majority of respondents had noticed the poster campaign and understood its irony. Those who had noticed the campaign differed from the pretest group by better acknowledgment of the personal risks they took and a lower endorsement of three popular excuses. Condom use in this group rose slightly. Yet, only half of the group ever used condoms, and a quarter were inconsistent in their use.
A 1992 addition to government involvement in sex education and prevention is a mass-media campaign directed at child sexual abuse. This campaign, “There Are Secrets You Should Talk About,” is designed to reach children in abusive situations and make the public aware of the reality of child sexual abuse. A second mass-media campaign, “Sex Is Natural, But Never Self-Evident,” addresses boys and men on the topic of coercion in sex. Evaluative data on these campaigns are not yet available.
B. Informal Sources of Sexual Knowledge
Veronica, a Dutch broadcasting company, has had a Sunday-afternoon, three-hour phone-in radio program on sex and related subjects since 1985. Themes discussed on program “Radio Romantica” range from light-hearted to serious, including sexual fantasies, falling in love, rape, incest, sexual abuse, safe-sex techniques, coping with AIDS, unwanted pregnancies, homosexuality, bisexuality, and pedophilia. A professional sexologist hosts the program with a liaison officer and a team of students and graduates trained in psychology and social work. The program draws about 250,000 listeners.
In a less systematic way, almost all Dutch broadcasting companies have programs dealing with sex and AIDS. Since the sexual revolution of the 1960s and 1970s, sexuality has provided prime topics for radio, television, and magazines. Books on sex education, for adults and adolescents, are numerous, and vary widely in quality. Pornography is easily available, although the information and messages propagated in these magazines is a matter of concern for many educators. The impact of pornography as an educational source has not been evaluated. (Section 11 deals with numerous mass-media campaigns on AIDS and safe sex.)
A. Children and Adolescents
Research on child sexuality is relatively underdeveloped. In 1990, readers of the magazine Ouders va Nu (Parents Today) responded to a questionnaire about their children’s sexual behavior and their own attitudes concerning sexual education (Cohen-Kettenis and Sanford 1991). The children’s ages ranged from 0 to 7. The results of this survey on child autoeroticism are shown in Table 1.
Table 1
Childhood Self-Pleasuring Behavior (in
Percentages)
|
Behavior |
Boys |
Girls |
|
Touches genitals with the hand |
96 |
94 |
|
Self-pleasures by hand |
58 |
39 |
|
Self-pleasures using an object |
13 |
21 |
Figure 1 - Percentages of Boys and Girls Engaging in Self-Pleasuring
Source: Vogels and van Vliet (1990), Figure 3.2, p. 37.B. Adults
In the 1989 research (Sandfort and Van Zessen 1991), questions on personal habits disclosed a distinct sex difference of several issues.
· 55 percent of the women and 23 percent of the men had never read sexually explicit books or magazines;Figure 2 - Percentage Frequencies of Self-Pleasuring According to Sex· 71 percent of the women and 47 percent of men had never watched sexually explicit videos or movies;
· 30 percent of the women and 5 percent of the men never looked at an attractive man with sexual intent, 26 percent of the men reported this behavior “often”;
· 77 percent of the women and 90 percent of the men were familiar with sexual fantasies. Men tend to fantasize more often and have a more positive view of fantasies. Fantasies featuring power balance and violence were uncommon.
· 92 percent of respondents reported a positive attitude toward self-pleasuring; only 16 percent opposed self-pleasuring in a steady relationship. Autoerotic behavior was related to sex, age, and current relationship status. (See Figures 2, 3, and 4.)
Source: Sandfort and van Zessen (1991), Table 4.10, p. 129.Figure 3 - Percentage Frequencies of Self-Pleasuring According to Age
Figure 4 - Percentage Frequencies of Self-Pleasuring According to Relationship Status
(n = 982; steady relationships, 75%; casual relationships, 13%; no sexual contact in past year, 12%). Source: Sandfort and van Zessen (1991), Table 4.6, p. 129.
A. Children
In the Parents Today study (Section 4A), many questions referred to childhood sexual behavior. Table 2 gives a selection of the data. In this study, Dutch parents reported considerably more sexual behavior than United States parents in similar studies, so U.S. data are not useful as criteria in diagnosing child sexual abuse in Dutch children.
Table 2
Childhood Heterosexual Behavior (in
Percentages)
|
Behavior |
Girls |
Boys |
|
Interested in the opposite sex |
63 |
63 |
|
Plays doctor-and-nurses games |
44 |
43 |
|
Tries to see nude people |
44 |
43 |
|
Touches genitals of others |
39 |
32 |
|
Tries to undress other people |
30 |
22 |
|
Shows genitals to adults |
15 |
25 |
|
Shows genitals to children |
16 |
24 |
|
Kisses with tongue out of mouth |
13 |
16 |
Puberty Rituals
There are no common puberty rituals among autochtonous Dutch groups, although as a result of the more open attitude towards sexual development in some progressive families, young girls will have their menarche greeted by some festive, yet intimate, parental or family attention.
It has been argued that in modern Western society, parallel to individualization tendencies, rituals have disappeared, leading to loss of emotional anchors. In psychotherapy, the use of individually tailored rituals is quite often recommended.
Premarital Sexual Activities and Relationships
The 1989 survey of children ages 11 to 19 involved more aspects than previous studies, and the presentation of many subjects that were put into longitudinal perspective. Data suggested an expanding “sexual moratorium,” a period in which the adolescent is sexually active, but not in a steady relationship open to procreation. In recent years, it has been increasingly common for young adults to go through a period in which they have a number of sexual partners, in more or less steady relationships (Figure 5).
Survey responses revealed a common pattern of four years between the first French kiss and sexual intercourse. The sequence of steps in this personal development is remarkably uniform, and showed no sex difference (Figure 6).
Figure 5 - Age at First Menstruation, First Sexual Intercourse, and Marriage or Cohabitation by Year of Birth

Source: van der Vliet (1990), p. 54.Figure 6 - Sexual Development: Age at Which Half of the Respondents Had Experienced Some Behaviors (n = 11,500)
Source: Vogels and van Vliet (1990), Figure 3.3, p. 39.In earlier studies, the concept of a “stepwise interaction career” was developed by Straver and coworkers (1986), based on Glaser and Straus’s (1980) elaboration of symbolic interactionist theory and Simon and Gagnon’s (1980) approach to psychosexual development. This approach emphasizes the active role of youngsters in shaping their own sexual identity and their sexual relationships. Rademakers (1992) later used this theoretical framework in her study of the causes of ineffective contraceptive behavior at initial sexual contact among adolescents (see Section 9).
Going out to bars or discotheques is a major factor affecting sexual experiences, increasing sexual experiences at all ages and in all aspects. Young people with lower educational levels showed less permissiveness and less experience in communication, but experienced sexual intercourse at an earlier age than adolescents with more education.
Responses to the question “Do you ask your partner what he/she likes in love making?” suggest that boys take responsibility for their partners’ satisfaction more often, especially at an earlier age (Figure 7). Assessing personal limits is another competence aspect; girls more than boys seem to consider this to be their task at all ages (Figure 8).
Sexual contacts between children and adults have been examined in several Dutch studies. Unlike most such research data, these contacts were not considered abusive by definition. Sandfort (1982) studied the experience of twenty-five boys, ages 10 to 16, involved in sexual relationships with adult men. Almost all the respondents indicated the sexual contact was predominantly positive and did not have a negative influence on their general sense of well-being. The friendships also fulfilled several of the boys’ personal needs. Although these results do not have general applicability, they counterbalance the predominant notion that all adult-child sexual involvement is abusive. In a later study, Sandfort (1991) used a much broader design to study the possible influences of voluntary, as well as nonconsensual, sexual experiences before age 16 in a random sample of 283 male and female subjects, aged 18 to 23 years, who had had sexual experiences with adults. Controlling for other factors, these sexual experiences seemed to have positively influenced sexual desire, arousal, and anxiety irrespective of the partner’s age. Nonconsensual experiences seemed to have caused sexual problems in later life, as well as more general psychosomatic complaints. The more severe these experiences, the stronger were the negative effects. Nonconsensual contacts with peers seemed, on average, to be less severe than nonconsensual experiences with adults. Using the same data, Goddijn and Sandfort (1988) showed the importance of the opportunity to express one’s feelings about traumatic experiences in order to diminish the psychosocial complaints in later life. Studies on involuntary sexual contacts are dealt with in Section 9A.
Source: Vogels and van Vliet (1990), Figure 3.9, p. 45.Figure 8 - Percentages of Respondents Who See to It That Lovemaking Does Not Get Out of Hand Always or Most of the Tune, According to Age and Sex
Source: Vogels and van Vliet (1990), Figure 3.9, p. 45.C. Adults
Some Demographic Outlines
Remarkable changes in the popularity of marriage have occurred in the Netherlands in recent decades (Beets et al. 1991). Before the end of World War II, the Dutch tended to marry at a relatively late age. In the years of rapidly expanding economic possibilities in the 1970s, more men and women married at a younger age. In 1945, only 18.5 percent of 20- to 24-year-olds was or had ever been married; in 1974, the figure was 41.8 percent. Since 1974, marriage has again declined in popularity, especially for the young, as cohabitation became more popular. The mean age of first marriage was 22.8 in 1970; in 1990, it was 28.2 for men and 25.9 for women. Data on cohabitation are scarce, but what data are available provide some insights:
· Around 1985, almost half of all 20- to 24-year-olds who were living together were not (yet) married, in the 25 to 34 age group, 20 percent were not married;Combining cohabiting and married couples, there is a recent slight decrease in the number of Dutch men and women living in two-person households. Divorce rates have gone up fast since 1968, from 11 percent of marriages in 1970 to 28 percent in 1988. One out of six children in the 1970s marriage cohort will experience their parents’ divorce before age 21. One-parent families are also increasing. Ten years ago, 19 percent of Dutch mothers were raising their child(ren) alone. Divorcees outnumbered widows and never-wed mothers in this group, with most single mothers holding full-time employment outside the home.· 70 percent of the unmarried said their living together would be long term; 40 percent of a cohort were still in the same relationship at a three-year follow-up;
· Cohabiting couples have fewer children than married couples; the wish for children is often the motive for marriage.
· Until 1975, only 2 percent of the children born annually were born out of wedlock. Since then, the figure has risen to 10.6 percent. “Extramarital birth” today can have several meanings: a child of cohabiting parents (about two thirds of all extramarital births); a child in a Living Apart Together (LAT) arrangement, a lesbian couple’s child, or a homosexual or heterosexual unwed mother who intends to raise the child alone. By 1989,10 percent of unwed mothers were single women and lesbian couples who were artificially inseminated with donor semen (AID). In the past decade, self-insemination has gained in popularity, probably equaling physician-managed AID today.
· The classic unwed mother who had an unwanted pregnancy is almost extinct in Holland, forcing the Dutch organization for the support of unwed mothers to reorganize with new goals to support one-parent households and the victims of sexual violence (and their mothers).
Divorced persons are increasingly postponing a second marriage. In 1990, the mean age for males entering a second marriage was 42.7; for women, 38.8 years. In 1990, 77 percent of all marriages were first marriages for both partners. In 23 percent, one or both partners were divorced; in 10 percent, one or both were widowers.
Fertility rates have been decreasing, from 3.2 in 1964 to stabilize at just over 1.5 since 1976. In 1988, 4 percent of all 20-year-olds had one or more children, 32 percent of the 25-year-olds, 67 percent by age 30, and 87 percent by age 40. Government policy aims at zero population growth, a goal that seems feasible even though it will bring a considerable increase in the proportion of senior citizens. In 1990, 13 percent of the total population was over 65, compared with only 8 percent in 1950.
Single Adults
Prompted by a need for data and insights useful in AIDS prevention, the 1989 SIN adult study was the first to pay specific attention to sexual behavior of singles.
In this survey, 13 percent of male respondents (n = 421) and 11 percent of females (n = 580) reported no sexual contacts in the year before the interview. Some 40 percent were sexually inexperienced. Part of this group could be adequately characterized as “late starters,” but at age 30, 8 percent of males and 4 percent of females were inexperienced in heterosexual intercourse. The higher percentage of male homosexuals in the sample may only partly explain the high figure of inexperienced males, because half of the male respondents who labeled themselves as homosexuals had in fact had sexual intercourse. Men tended to be more dissatisfied than women with being single, 70 percent versus 57 percent preferring to have a relationship. In the larger cities, the proportion of respondents with no sexual relationships is slightly lower. In their solo-sex experiences, this group differs only slightly from couples: 18 percent never fantasize sexually, and only 19 percent more than once a week; 28 percent never engage in self-pleasuring and 26 percent do so more than once a week.
In the 1989 study, “singles with sexual contacts” were defined as: no steady relationships of at least one year at the time of interview; one or more casual or short sexual contacts. By definition, this group must include a certain number of persons with new relationships that will eventually turn out to be long term: 10 percent of women and 18 percent of the men fell into this category. Respondents under 25 contributed most to this group, with respondents 33 to 50 rarely in this group. Singles with sexual partnerships tended to live in larger cities. Like the group with no sexual experiences in the last year, they, too, tended not to be politically involved. One-night stands were uncommon: only 13 percent had casual sex (defined as once or twice); 50 percent of men and 25 percent of women had casual sex besides one or more longer partnerships (the latter with a mean of twenty-five sexual encounters). Males reported a higher number of partners in the past year (mean 2.4 versus 1.8 for women; maximum of ten for men and five for women). Vaginal intercourse was the most popular technique for men (96 percent), but women preferred manual stimulation to vaginal intercourse, 95 percent to 86 percent. Anal intercourse was quite unpopular. Men used condoms in only 31 percent of their coital acts; women scored even lower with 21 percent.
Adults in Dyadic Relations
In 1989, mean coital frequency for men and women in stable relations was seven times a month, higher than in 1968 and 1981, but respondents in the earlier surveys were aged 20 to 65, while the 1989 sample was 18 to 50 years old (Table 3, Figure 9). Length of the relationship is more important than age for coital frequency (Tables 4 and 5, Figure 10). In all groups, women tended to be content with their current frequency and men more likely to want more. Men were more affirmative in thinking their sex could be better. Women were more likely to admit to making love without the desire to do so and engaging in sexual acts they did not really like. Other satisfaction-related statements on which men and women gave similar responses included: general satisfaction with sex, conflicts about sex, admitting gender differences in sexual desire, admitting being pressured to engage in sexual contact, and communications on sexual preferences. On a one-to-ten scale, the mean rating of men for their satisfaction with their own sex life was 7.3; for women 7.5.
Abstinence in these stable relations is nonexistent, when defined as refraining from all sensual body contact (hugging, kissing, and cuddling). When sexual contact is defined as genital contact, 0.5 percent of these relationships were abstinent; when defined as vaginal intercourse, 4 percent were abstinent during the past year (Figure 11).
Table 3
Duration of Living Arrangement in 751 Stable
Relationships
|
Age Group |
Mean Duration of Relationship |
Married |
Cohabiting |
Living Apart |
|
18-25 |
4.0 |
24 |
33 |
43 |
|
26-33 |
8.8 |
73 |
20 |
7 |
|
34-41 |
14.1 |
86 |
5 |
9 |
|
42-50 |
22.4 |
97 |
1 |
2 |
Men: 71 = 276; Women: n = 452Figure 9 - Percentage Frequencies of Making Love in 751 Stable Relationships
Source: Sandfort and van Zessen (1991), Table 3.3, p. 65
“Extramarital” Sex
Marriage was the only form of stable relationship studied in 1968 and 1981. In the 1989 study, questions regarding sex with more than one partner were edited differently to include cohabitation and stable Living-Apart-Together (LAT) relations. Moreover, the 1968 and 1981 studies focused on 21- to 65-year-olds, whereas the 1989 study dealt with 18- to 50-year-olds. Longitudinal comparisons must therefore be done with some caution.
Table 4
Mean Frequency of Sexual Contact in Steady Relationships,
by Age
|
Age Group |
Mean Frequency of Sexual Contact, per Month |
|
18-25 |
7.4 |
|
26-33 |
7.0 |
|
34-41 |
6.9 |
|
42-50 |
6.8 |
|
Duration of Steady Relationship (in Years) |
Mean Frequency of Sexual Contact, per Month |
|
1-2 |
8.5 |
|
2-5 |
7.5 |
|
Over 5 |
6.8 |
Source: Sandfort and van Zessen (1991), Table 3.4, p. 66Figure 10 - Satisfaction with Frequency of Making Love, by Sex and by Three Groups of Frequency
Source: Sandfort and van Zessen (1991), Figure 4.2, p. 107.
In 1968 and 1981, men were more tolerant than women on extramarital sex, with a shift for both genders toward more tolerance. In 1981,13 percent of the men and 6 percent of the women had no objections at all, with 48 percent of the men and 39 percent of the women accepting extramarital sex in certain situations. In 1989, more questions were included on this topic. Seven percent of the men and 5 percent of the women agreed that partners in a stable relationship should allow each other to have sex with a third party; 82 percent of men and 88 percent of women firmly opposed this (Table 6).
Figure 11 - Sexual Behaviors in Stable Heterosexual Relationships, According to Sex
Men n = 276; Women: n = 452. An * indicates a significant sex difference.Since extramarital sex is taboo more than other behaviors, underreporting cannot be ignored. In 1989, the fear of AIDS seemed to be a more potent motive for denying extramarital sex than moral restraints in general. Marriage is the type of stable relationship that contributes most to monogamy: In the total group of respondents in a stable relationship for over one year, 14.6 percent of the men and 9.2 the percent of women reported sexual contact with more than one partner. In the year preceding the interview, 6.4 percent of the men and 2.8 percent of the women had engaged in sex with a second partner; 2.1 percent of the men and 3.7 percent of the women were aware of their partner’s extramarital relations. Three quarters of the men keep their extramarital sex a secret; three quarters of the women informed their partners of their affair. “Extramarital sex” was casual in 50 percent of the cases; long-standing affairs were limited to one out of six. Prostitution and sexual contacts abroad were only a small proportion of the reported extramarital-sex contacts.
Source: Sandfort and van Zessen (1991), Figure 3.2, p. 67.
Table 6
Extramarital Sexual Contacts in 1968, 1981, and 1989, in
Percentages
|
Frequency
|
1968 |
1981 |
1989 |
|||
|
Male |
Female |
Male |
Female |
Male |
Female |
|
|
Occurred often |
1 |
0 |
3 |
2 |
- |
- |
|
Occasionally |
10 |
2 |
11 |
7 |
12 |
7 |
|
Never |
78 |
86 |
80 |
86 |
88 |
93 |
|
Not Answered |
11 |
12 |
7 |
5 |
0 |
0 |
Source: Sandfort and van Zessen (1991), Table 3.10, p. 751Sexuality and the Disabled and Chronically Ill
In the early 1970s, when Heslinga gained national and international notoriety with his plea for better information and sex education for the handicapped with his book Not Made of Stone: Sexuality of the Handicapped People, these services are not routinely provided by doctors, and empirical research was also scarce. Today, close to a hundred organizations provide support and written information on the sexual consequences of such conditions as adrenogenital syndrome, anorexia nervosa, breast cancer and mastopathy, depression, diabetes, gynecological cancer, incontinence, ostomy, multiple sclerosis, premenstrual syndrome, postmenopause, posthysterectomy, and schizophrenia patients and their families.
Direct sexual services for the handicapped are available through the National Foundation for Alternative Partnership Mediation. In one ongoing research project, the Rotterdam sexology department and the department for industrial design at Delft Technical University developed a water-driven self-pleasuring aid for manually disabled men and women to be used in the bath or under the shower.
Mental-health institutions have also gained some awareness of their residents’ sexual problems and the tension between controlling and understanding patients’ sexual needs. Professionals in homes for the mentally handicapped seem more eager to take additional courses in sexual education. Awareness of the high figures for past sexual abuse among patients is growing rapidly, and competence in addressing these problems is probably also expanding.
In the past decade, Dutch sexologists have carried out longitudinal research on sexual rehabilitation of (1) women with ovarian, cervical, endometrial, and vulvar cancers, (2) men with testicular cancer and Peyronie’s disease, and (3) men and women with diabetes, various ostomies, chronic kidney disease, and skin diseases. Because of the uniqueness of these studies, a summary of their Findings follows.
(1) Cancer of the Female Genitals (Main sources: Leiden and Groningen University Gynecology Departments). The Dutch Cancer Foundation has funded a steady series of research programs on treatment for female genital cancers. Bos-Branolte used a semistructured interview and questionnaire to evaluate psychosexual functioning of sixty-nine women treated for ovarian (twenty-nine), cervical (twenty-four), endometrial (twelve), and vulvar (four) cancers. Posttreatment follow-up ranged from six months to seven years. Results showed a decrease in sexual activity (59 percent) and intimacy (22 percent) with an increase in need for intimacy (19 percent), emotional support (30 percent), and open communication (23 percent). In addition, 33 percent reported a negative change in their partner’s sexual activity. Many women had the impression that, although their partners needed emotional support during their illness, they did not receive this help. Intimacy, emotional support, and open communications seemed to contribute more to a positive relationship than sexual expressions.
In 1984, Weijmar Schultz and Van de Wiel started a series of research projects with a pilot study of ten women treated for vulvar cancer. A self-report questionnaire evaluated sexual functioning some two years after treatment. Despite many problems, eight of the ten couples resumed sexual contacts, with or without restrictions. Sufficient information, coping, and communications did not guarantee complete sexual rehabilitation. Motivation for sexual expression and mutual affection might be more important than any physical restriction imposed by surgery. A small-scale prospective longitudinal study of the sexual functioning of women treated for vulvar cancer tested this observation. Ten couples and an age-matched control group were interviewed and filled out questionnaires at admission and at six, twelve, and twenty-four months posttreatment. Only at six months could an increase in sexual dissatisfaction be detected. Over the remaining period, in spite of persisting poor perception of genital symptoms of sexual arousal, the women’s satisfaction did not differ from pretreatment satisfaction and control group ratings. Satisfaction with sexual interaction under these circumstances appears to be more dependent on intimate aspects than on physiological arousal, suggesting information and counseling as the most promising focus for intervention.
A more detailed assessment of seven of these women at twelve months posttreatment confirmed that, although in the patients’ own opinion cancer and its treatment had caused rather dramatic changes in their sexual life, comparison with the age-matched group revealed only minor differences in sexual satisfaction, behavior, and motivation. The only significant differences were in experienced sexual arousal and orgasm. The authors hypothesized that sexual rehabilitation itself is guided on a higher level by a more general striving for balance in the relationship. Interventions to prevent or reduce sexual problems after treatment for cancer of the female genitalia should be directed toward both the patient and partner.
A similar design was used for thirteen couples with wives treated by simple hysterectomy for benign gynecological disease and thirteen age-matched control couples. At a one-year follow-up, all patients reported some disruption in the sexual response cycle, whereas current behavior and motivation for sexual interaction were within the normal range. The women clearly expressed general satisfaction with their sexual functioning and little relational dissatisfaction. Here too, arousal experience is found not to be the sole reason for sexual motivation and satisfaction. The authors stress that post-treatment counseling should not be limited to hysterectomy patients with a cancer diagnosis. A more-detailed examination of eleven cervical cancer patients at six months posttreatment revealed that sexual interaction was valued significantly less than control subjects, while no changes in overt behavior occurred. The most important psychosexual variables underlying this reduced sexual valuation were found to be a considerable decrease in the self-image of oneself as a sexual partner. Apparently women try to cope by conforming to the sexual demands of their partner and to prevailing norms. Cervical carcinoma treatment appears to have a strong negative effect on the sexuality of the patients, and often amplifies an already existing ambivalence toward sexual interaction common in many women.
Sixteen partners of patients treated for female genital cancer were interviewed one year posttreatment on two general themes: involvement and support, and sexuality and relationship. Many men reported experiencing the process of providing support as stressful, and had serious doubts about the efficacy of their efforts. Furthermore, these men appeared to have extensive sexual problems, which could not be adequately solved. It was hypothesized that the disease and its treatment also poses a crisis for the partner, which leads to a regression towards a more rigid, male-stereotypical way of coping. Consequently, while treating the patient, the partner and their communication patterns should be the focus of attention too.
Finally, data on seven vulvar cancer patients and twenty-five cervical cancer patients were analyzed for prognostic variables for future sexual adjustment. The small sample size allowed only a few cautious conclusions. Overt sexual behavior after treatment can be predicted quite accurately by past sexual experience. Satisfaction, motivation, and sexual response are less predictable. This outcome supports the conclusion from the comparative study on cervical cancer treatment and simple hysterectomy, that psychological variables are more decisive than physical ones in predicting future sexual rehabilitation.
(2) Testicular Cancer Treatment (Source: Groningen University Urology Department). Nijman et al. studied sexual functioning of 101 patients following bilateral retroperitoneal lymph node dissection for stages I and II nonseminomatous testicular cancer. All patients were without evidence of disease after at least four years’ follow-up. Twelve men experienced ante-grade ejaculation, while eighty-nine experienced retrograde ejaculation (“dry” orgasm). In seventy-five of the 101 men, urine analysis after intercourse or self-pleasuring showed retrograde ejaculation in fifty-five men, and lack of ejaculatory emission into the urethra in twenty patients.
Seventeen patients had diminished sexual desire (especially after radiotherapy), twelve experienced difficulty reaching orgasm, and six complained of erectile dysfunction. A second study of fifty-six men with nonseminomatous testicular cancer stages II and III, before and after treatment (surgery and chemotherapy). Two years after completing therapy, 54 percent experienced sexual dysfunctions. Greatly reduced or absent antegrade ejaculation was reported by twenty-six patients; eighteen of them had undergone retroperitoneal lymph-node dissection in varying degrees of extensiveness, whereas eight had not. Chemotherapy may have caused ejaculatory disorders in 30 percent of the patients. Only two reported a change in quality of erections; seven experienced a markedly reduced libido, and five reported their orgasms had changed in a negative way. The remaining testis showed signs of atrophy in twenty-one patients.
(3) Diabetes Mellitus (Source: Rotterdam University Sexology Department). Slob et al. recorded subjective and objective psychophysiological responses to erotic visual stimulation for twenty-four women with diabetes mellitus type I and ten control women. No significant differences in subjective response (general sexual arousal and genital arousal) was reported. The objective response (thermistor readings from one minor labium) varied with the height of the initial temperature. Since the initial temperature was significantly higher in the patient group, the subsequent rise during erotic visual stimulation was less in diabetic women than in controls. When samples of the two groups were matched for initial temperature, the difference in increase of labial temperature was no longer significant. When women with high initial temperatures (37° C) were excluded, there was in both groups a significant correlation between the degree of subjective arousal and the rise in labial temperature. Patients with serious neuropathy and/or angiopathy did not participate in this study.
(4) Peyronie’s Disease (Source: Groningen University Urology Department). Van Driel studied surgical treatment, compared with the natural course, in thirty-two patients with Peyronie’s disease and twelve with a congenital penile curvature. Subjective symptoms were recorded by check list, objective symptoms by means of Polaroid photography during erection at home. Patients were seen at three-month intervals until a steady state was reached. In twenty-three patients, spontaneous recovery was sufficient. When pain persisted longer than one year, a Nesbitt operation (surgical shortening of the contralateral side) was performed; twenty-one patients were treated this way. All were satisfied with the functional and cosmetic outcome, although a completely straight penis was not accomplished in four. No complications were met. Conservative management in cases of bent penis seems preferable; however surgery is a good and safe alternative when complaints and dysfunctions persist.
(5) Ostomy (Source: Groningen University Sexology Department). The first step in Dutch research on sexological sequelae of ostomy operations was a study in which readers of a stoma patients’ monthly were asked to complete a questionnaire: 995 men and 512 women gave a retrospective account of changes in their sexual life following ostomy. Results confirmed that men are more hampered in their sexual functioning by ostomy than women, and that colostomy had a stronger negative effect than ileostomy. Results suggest the most serious impact on sexual functioning is found with urostomy, especially in men. Prospective confirmation is needed.
(6) Chronic Kidney Disease (Source: NISSO). Van Son-Schoones used a semistructured interview and psychometric questionaires to evaluate psychosexual functioning in seventy men and forty-seven women with chronic kidney disease; thirty-four male partners and forty-seven female partners were included. Evaluation included the effect of treatment method (hemodialysis, continued ambulatory peritoneal dialysis, or transplantation) on sexual functioning, personal well-being, and coping with the disease, as well as the quality of information and counseling. Few differences were found between the three treatment modalities. Organic sexual dysfunctions, psychosocial problems, and acceptance problems were most frequently found in the hemodialysis group. Partners, irrespective of treatment, did have more sexual problems and were less satisfied with the sexual relationship. The quality of information and counseling appeared to be insufficient.
(7) Skin Disease (Source: Leiden University Dermatology Department). In 1990, a research study was initiated to quantify the well-known sexual problems of patients with psoriasis and constitutional eczematous rash: fifty-two psoriasis patients (twenty-eight men, twenty-four women, mean age 37) and twenty-five eczema patients (nine men and sixteen women, mean age 28) completed extensive anonymous questionnaires: 10 percent had no partner, 3 percent only incidental partners. Men felt most ashamed in social situations of partial nudity, women were more ashamed in sexual situations. Sexual motivation was lower than average, and women scored lower than men. On sexual satisfaction, only women scored below average. Facial skin symptoms were most embarrassing. One third had difficulties initiating contacts and entering a sexual relationship, and felt shame in an intimate relation. Psoriasis patients felt more inhibited than eczema patients. Many expressed the conviction that a good sexual relationship is beneficial for the skin disease.
The authors advocate more discussion of sexuality in the care for skin-disease patients, especially when young and inexperienced in sexual relations. Women, psoriasis patients, and patients with facial symptoms are most in need of counseling.
Incidence of Oral and Anal Sex
Growing concern about HIV transmission and recognition that anal intercourse is high-risk behavior have attracted researchers’ attention to anal sex. In 1989, 12 percent of women and 6 percent of men in steady heterosexual relationships reported being more or less experienced in anal intercourse. Anal sex seemed to be nonexistent in casual and extramarital heterosexual relations.
In the Amsterdam large-scale longitudinal cohort research project on homosexual behavior and seroconversion, the proportion of men who engaged in anal intercourse slowly declined from 88.6 percent in 1984-85 to 62.4 percent in 1987-88.
There are no legal restrictions on anal sex in Holland; social attitudes towards this form of eroticism probably shows wide variation. The idea that anal sex is not an exclusively homosexual variation, but can be part of heterosexual lovemaking as well, is gradually being acknowledged in the general public.
In 1989, experience with fellatio and cunnilingus was the rule for both men and women (see Figure 11).
In the United States, the Kinsey-scale differentiation between exclusive homosexuality and exclusive heterosexuality based on combined sexual behavior and erotic experiences dominates most orientations theory and research. Historical, sociological, and psychological studies of homosexuality in the Netherlands leans toward a different paradigm in which homosexuality is seen as a design for living in which erotic and sexual attraction is embedded in a wider context. Dutch study of homosexuality thus focuses on gender and gender development, family studies, and lifestyle and lifestyle management. Changing social attitudes to homosexuality made this paradigmatic change possible.
A. Children and Adolescents
The large-scale 1968 and 1974 studies of adolescent sexuality paid only limited attention to homosexual behavior and feelings. Tolerance towards homosexuals had grown considerably: In 1968, 55.3 percent believed that homosexuals should be free to lead their own lives; in 1974, 84.9 percent held this position. In 1968, 18.6 percent of male respondents said they had at least one self-pleasuring experience with peers; in 1974, this was 16.1 percent. In 1968, 5.5 percent reported being mostly or exclusively attracted to the same sex; in 1974, 1.8 percent. Some attraction was indicated by 10 percent in both surveys.
Information useful in AIDS prevention was a major objective of the 1989 study of 11,431 12- to 19-year-old boys and girls. On self-definition, 47 percent of the 12- to 13-year-olds reported not knowing the meaning of “homosexuality” and “bisexuality”; 6 percent of 18- to 19-year-olds were ignorant on this subject. Slightly less than 1 percent of boys and girls defined themselves as exclusively or predominantly homosexual; 1.3 percent of boys and 0.8 percent of girls defined themselves as bisexual; 8 percent of boys and 15 percent of girls reported fantasies of a homosexual nature. Such fantasies produced uncertainty on self-definition in only a minority; the youngest age group is most often uncertain on the subject of self-definition (60 percent of 12- to 13-year-olds did not know how to self-label).
Percentages of respondents experienced in homosexual behavior were low: boys 1.5 percent, girls 1 percent. Anal intercourse was practiced by half of these boys - among heterosexual 14- to 19-year-olds, 7 percent had at least one experience with anal intercourse. Bisexual experience was reported by 64 percent of the boys and 70 percent of the girls.
In the 1980s, several studies of homosexualities examined the process that homosexuals go through in self-definition. A large difference was found between males and females. More than 50 percent of men called themselves homosexual by age 17, 50 percent of women self-identified around age 23. Half of the boys experienced their first same-gender attraction by age 8; girls by age 14. In the process of sexual-identity formation, behavioral, psychic, erotic, and sexual responses appear more important for self-definition for boys. For girls, relational factors are characteristic, with identity formation and identity management centered on social, instead of sociosexual aspects. Defining oneself as a homosexual for boys means the coding of erotic and sexual responses, and for girls the coding of feelings of intimacy, bonding, and togetherness. These are relative differences and one could predict that, as soon as gender differences in development become less important, the gap between a gay and lesbian development of the self will disappear. This accounts for intergenerational differences and the positive influence of a warm and permissive climate at home on identity development. In a theoretical perspective, in families without polarized sex roles, not only do male-female differences become less important, but also the distinction between homosexual and heterosexual differences. What counts is the capacity for management of social interactions.
Of special interest are Dutch studies on the construction of intergenerational male intimacy. Sandfort (1987) described how this developed in the gay movement and how concepts of male homosexuality and male homosexual pedophilia changed between 1946 and 1981. In a monumental two-volume work, Loving Boys (1988, 1990), Brongersma maintained that intergenerational male intimacy has a biological as well as a sociological foundation. At the beginning of puberty, boys tend not to interact sexually with girls. In this period the sexual drive is high, so boys enter into sexual contact with peers and with older men. This view of man-boy relationships uses a theoretical framework that relies heavily on historical and anthropological material. These relations are seen as a rite de passage, emotionally loaded by images of becoming male, not homosexual. Another sociohistorical illustration was presented by Maassen, who described the work and life of Gustav Wyneken, an influential pedagogue of pre-Nazi Germany, accused of having had sexual relations with some of his pupils.
In a 1992 special women’s issue of Paidika, the journal of pedophilia, some Dutch authors described woman-child intimate relations, of which the majority was homosexual and in some way pedagogic. While woman-girl relationships appear rare in Holland, Wekker describes a special kind of woman-girl relationship in Suriname Creole working-class women (mati) who are self-supporting and have children by men with whom they are in more or less steady relationships. They become familiar with homosexual contact in their teens, are mostly initiated by older women, and large age differences are common at all ages in this cultural group. One wonders whether the subject of adult-child sexuality is changing under the influence of coeducation, the development of youth cultures, and the acceptance of sexual relationships in early adolescence. Nowadays, adolescents can have sexual contacts with peers of both sexes, so the motivation for erotic commitments with adults may decline or disappear.
B. Adults
Gender Roles and Relationship Patterns
Tielman’s Homosexuality in the Netherlands (1982) describes the Dutch Gay Emancipation Movement between 1911 and 1982. Warmerdam and Koenders (1987) described the homosexual organization COG between 1946 and 1966. Detailed oral histories of the discrimination against homosexuals and their emancipation are available. There are numerous impressions, accounts, and photographs available, and a lot is analyzed in Homologie, a scientific and cultural bimonthly. Still missing, however, is a broad and thorough study of the homosexual and lesbian subcultures in these periods from a nonpolitical perspective.
Hekma (1987) analyzed how during the nineteenth century, Dutch physicians and psychiatrists, influenced mainly by German and French ideas, constructed a homosexual identity with specific bodily and mental characteristics. This widely accepted image of gay and lesbian identity was disputed by Muller (1990), who showed that most German physicians relied heavily on personal statements of their clients, who in their self-confessions constructed homosexuality themselves. The theoretical issue is, as in other psychiatric cases of alcoholism and anorexia, who has the power in the discourse, who “invents” the images, the categories, the definitions of the self? It seems that in the nineteenth century, the “making of the homosexual” was mainly an interaction of physicians and their patients. In the twentieth century, homosexuals discovered themselves as a community.
Dutch research on gay and lesbian relationships took root in our tradition of research on alternative relationships. Instead of focusing on differences between marriage and alternatives, Dutch researchers try to understand the dynamics of different forms of relationships. Straver (1981) found that among unmarried couples - heterosexual, homosexual, and lesbian - some couples structure their relationship in a traditional, strong role differentiation, while others accentuate complete togetherness with a tendency towards independence. Still others emphasize self-development. Living together is no longer an essential condition in forming a relationship. Straver does not present a correlation between these models and sexual orientation.
Schreurs (1990) compared lesbian, cohabiting women (above average in education, income, and professional activity, and mainly in their 20s and 40s) with a similar group of heterosexual couples. Analysis produced Stravers types of relationships, except for the strong role-differentiation type. Relations characterized by togetherness led to the highest scores for relationship satisfaction; couples in autonomy relations expressed satisfaction with autonomy as well as with togetherness. A group characterized by distance scored identical on autonomy, but lower on togetherness. In comparison with heterosexual couples, only emotional and recreational bonding scored lower in heterosexual couples, and men scored lower on satisfaction with emotional bonding.
Schreurs criticizes current theories in which lesbian relations are considered a risk for symbiosis (i.e., high bonding with loss of autonomy). In lesbian relationships, a high degree of emotional bonding obviously is possible without loss of autonomy, an important consideration for therapists working with lesbian couples.
In a similar study, Deenen (1991) analyzed 320 men in steady homosexual relationships: 69 percent lived together; mean relationship duration 8.2 years (10-39 months: n = 88 with mean age 30; 40-199 months: n = 138 with mean age 36; 120-446 months: n = 93 with mean age 45. He found no support for the phasic developmental model of McWhirter and Mattison (1984), who hold that sexual and emotional satisfaction depend on the time of a relationship between two men. Deenen found differences between short- and long-lasting relationships, and a difference between men younger than thirty years and older men. Both variables, relationship duration and partner’s age, predicted relationship satisfaction and sexual satisfaction better than the phasic developmental model.
For women and men in homosexual relationships, emotional intimacy is the best predictor for relationship satisfaction. Sexual contact seems more important for men, but this difference may disappear if one relies on a less-strict definition of sexual contact and replaces it by affectionate bodily contact. One can go even further, seeing the whole erotic and sexual attraction embedded in the more general context of living, a line of reasoning also found in Dutch studies of sexual identity and identity development.
Social Status; Legal and Religious Restrictions
In the late 1960s, Dutch research on homosexuality was characterized by a social-scientific perspective in which the changing of social attitudes towards homosexuality was a primary objective. In 1968, 36 percent of Dutch adults believed that homosexuals should be restricted in leading their own way of life. In 1980-87, this figure stabilized around 6 to 7 percent.
Until 1971, the legal age of consent for homosexual acts was 21 years of age; for heterosexual acts, 16. This statute was abolished in 1971, mainly on the argument that scientific research showed that people did not become homosexual by seduction at puberty or in adolescence. The new law and general tolerance had a great impact on the counseling of people with problems of homosexuality. Gradually, the image of homosexuality as a psychiatric symptom disappeared completely. In the 1980s, newly established departments of gay and lesbian studies at the Universities of Utrecht and Amsterdam triggered a diversity of studies on homosexuality. Studies of genetic, hormonal, and neural factors are insignificant, the emphasis being placed instead on history, sociology, and social psychology.
While tolerance certainly has increased, this does not exclude all sorts of gross and subtle discrimination, including violence. For decades, youth gangs have beat up gay men in cruising areas. It took the homosexual movement a long time to persuade the gay victims (often men seeking anonymous sexual contacts while they were still “in the closet”) to accuse their assaulters in court and to convince police officials that this form of violence should be taken seriously.
Two legal topics are currently under discussion, legislation against discrimination and legal recognition of gay unions. Legislation against discrimination on grounds of race, sex, sexual lifestyle, etc., has taken more than a decade. During these years, religiously inspired parties have tried successfully to introduce exceptions based on conflicting interests. The central issue is always whether Christian schools will dismiss or refuse to hire homosexual teachers.
Although Dutch civil laws do not specify the heterosexual essence of marriage, no gay or lesbian couple has been able to enter a legally recognized marriage. Two recent efforts to gain this recognition have been turned down by the high court with the suggestion that the matter should be studied by the government and a law reform prepared. All political parties support this opinion.
Discrimination and homophobia are expected in macho cultures such as the military. Since 1971 and the abolition of the penalty for homosexual acts after age 16, homosexuality has been tolerated in the military. A 1992 NISSO study of homosexuality in the military concluded that:
· Drafted men did not differ from the general population in homosexual feelings and experience;This 1992 NISSO research marked a milestone in the development of attitudes towards homosexuality in the military. COC, the national organization of homosexuals, gave the Dutch Minister of Defense and the Foundation Homosexuality and the Armed Forces its annual reward. In 1993, a national confidential counselor on homosexuality in the military was instituted.· Male professionals less often reported homosexual feelings and experience;
· Female professionals more often reported homosexual feelings and experiences - women are not drafted for military service in Holland.
· In all branches and at all levels, respondents were aware that discrimination was not tolerated; female soldiers were more tolerant than their male colleagues. Yet, distancing and isolation in some form was a common reaction, and unconditional support was often withheld from homosexuals. When open about their sexual orientation, homosexuals were excluded from the comrade culture. Homosexuals tend to be isolated much more than allochtonous soldiers.
· Excesses, from abusive language to physical attacks, are not uncommon in the army.
· Homosexuals tend to mask their orientation while in service. In their immediate environment, homosexuals have little support - the Foundation Homosexuality and the Armed Forces functions only on a national level.
There is not much information on homosexuality in other organizations, e.g., prisons. Coercive homosexual contact in institutions, as is known from reports in the United States, are reported incidentally, but these acts are definitely not prison routine. Homosexual rape is seldom reported to the Dutch police. A few cases of male pedophilic or incestuous offenses are brought to trial each year, but cases involving adult victims are rare.
Prevailing Patterns in Sexual Behaviors
The 1989 survey showed that homosexual and bisexual people tend to be the most permissive on the subject of sex in general (Table 7 gives results for 421 male and 580 female respondents).
Table 7
Homosexual Experiences
|
Experience |
Male |
Female |
||
|
Number |
Percent |
Number |
Percent |
|
|
Ever felt physical attraction |
54 |
13 |
59 |
10 |
|
Ever been in love |
25 |
5 |
18 |
3 |
|
Ever has thought to be homosexual |
33 |
8 |
19 |
3 |
|
Ever had sex with a person of the same sex |
50 |
12 |
25 |
4 |
|
More than incidentally had sex with a person of the same sex |
24 |
6 |
13 |
2 |
|
Same-sex attraction is currently present |
24 |
6 |
19 |
3 |
|
Feels to be (primarily) homosexual |
17 |
4 |
2 |
0.4 |
Source: Sandfort and van Zessen (1991), Table 2.3, p. 4Physical attraction for same-sex partners was felt at a mean age of 14 for male and 19 for female respondents. This difference was smaller in the younger age groups. Respondents reporting attraction to same-sex partners generally were confused and worried by these feelings. After a mean duration of three years, these feelings subsided in about half of the men and two thirds of the women. Men who are attracted to men tend to have had some form of sexual contact at least once; in women, attraction led to sexual behavior in only a minority. The time from first sexual attraction to sexual contact was shorter for men than women (Table 8).
Homosexual and bisexual men had a much larger number of sex partners; for women, total numbers were too small to form conclusions. For homosexual men, the mean number of partners in the past year was 9.1; in the past five years, 48.6, and in their whole life, 270.3. In comparison, heterosexual men reported means of 1.1,1.4, and 3.9 for the same periods. Bisexuals reported numbers between these two extremes.
Long-term relationships (mean duration six years) were reported by two thirds of the homosexual respondents. Of the men, half of this group had an open relationship with incidental contacts tolerated. The mean for such incidental contacts was twelve, which is not different from the mean of homosexual men not engaged in a steady relationship. In steady relations, anal intercourse was common (82 percent) and condom use was extremely rare. In incidental homosexual encounters, anal intercourse is practiced by a quarter of the men with condom use uncommon. Gay bars and cafes, saunas and Turkish baths, some well-known highway parking places, and parks were the main sites for incidental contacts. All sorts of subculture variations are available, especially in Amsterdam, including leather and S-M, piercing, and tattooing.
Table 8
Current Sexual Orientation, by Self-Labeling and Behaviors,
in Percentages
|
Criteria |
Males |
Females |
|
Self-labeling |
||
|
Exclusively heterosexual |
89.5 |
92.9 |
|
Almost exclusively heterosexual |
4.5 |
4.1 |
|
Mainly heterosexual |
1.9 |
2.1 |
|
Equally homosexual and heterosexual |
0.0 |
0.5 |
|
Mainly homosexual |
0.7 |
0.9 |
|
Almost exclusively homosexual |
1.9 |
0.2 |
|
Exclusively homosexual |
1.4 |
0.2 |
|
Behavioral |
||
|
Exclusively heterosexual |
81.7 |
88.4 |
|
Bisexual |
1.9 |
0.5 |
|
Exclusively homosexual |
3.6 |
0.3 |
|
Never had sexual relations |
12.8 |
10.7 |
Bisexual respondents in the 1989 study are relatively young. They tend to self-label as heterosexual and their behavior pattern is similar to heterosexuals with short-term relations. Anal intercourse is rare and, when practiced, condoms will be used, contrary to vaginal intercourse in which condom use is rare.
It is remarkable that there has never been a research study on homo (bi) sexuality in marriage in Holland. The 1968 and 1981 studies showed that 2.3 percent and 3.3 percent respectively of male respondents with predominant or exclusive homosexual attraction were, or had been married. Married homosexuals sometimes will seek help from professionals, but the only organization for marriage and homosexuality is the self-help group Orpheus.
Table 9
Frequency of Sexual Contact in Steady
Relationships
|
Frequency |
Percentage |
|
None |
4.1 |
|
Once in a while |
6.9 |
|
1-3 times a month |
17.3 |
|
1-2 times a week |
43.1 |
|
2-5 times a week |
25.2 |
|
6 or more times a week |
2.2 |
Source: Deenen, 1991
The first and most important clinic specializing in gender dysphoria is the Academic Hospital of the Free University of Amsterdam. The Dutch Gender Foundation was established in 1972. After several years of informal contact with the Free University Hospital, the ethics committee gave its approval to the medical treatment of transsexuals. The clinic started in 1976, mainly with hormonal treatment and a small number of surgical corrections. In 1982, a multidisciplinary team was formed, following the guidelines of the Harry Benjamin International Gender Dysphoria Association. Medical treatment is covered by health insurance. Support and peer-group contact are provided in some large cities by the Dutch Society for Sexual Reform (NVSH) and the Organization for Humanistic Help. Self-help groups often include transvestites. Special groups for parents and other family members have been organized recently. The most recent, and tragic, expansion of self-help for transsexuals is a group of persons treated with sex-reassignment surgery who regret the operation.
There are few legal barriers to the sex change after a legal reform that took place in 1985. A transsexual’s sex may be corrected on the birth certificate if a medical declaration states that the person is irreversibly bodily corrected to the other sex and is permanently infertile. Married transsexuals must divorce before the birth certificate can be changed. At the same time (or sometimes earlier), a person’s given name may be changed.
Thus far, some 1,500 transsexuals have been assessed by the Amsterdam gender team; approximately 150 sex-reversal surgeries (SRS) have been performed. In 1988, the Free University founded a chair for transsexology, which was awarded to Louis Gooren. Utrecht professor Peggy Cohen-Kettenis, whose chair (installed in 1992) is dedicated to gender development and psychopathology, works in close collaboration with the Amsterdam team. In some adolescent cases, treatment began before the patient’s pubertal maturation process was fully completed; some twenty patients completed their SRS before or shortly after age 18. These teams also carry out training and research activities. Two smaller gender teams are active in Groningen and Arnhem, unfortunately not active in research.
The incidence of male-female transsexuality has been estimated at 1:12,900; and for female-male 1:30,400. Scientific attention to further diagnostic specification is expanding, especially for the concept of primary (aware since early childhood) versus secondary (awareness developing later in life) transsexuality.
Kuiper (1991) has provided the most extensive evaluation of the Amsterdam SRS treatment approach, reporting on 105 male-to-female and 36 female-to-male transsexuals, all at least in the phase of hormonal treatment. In a long-term follow-up, 50 percent of male-to-female and 75 percent of female-to-male transsexuals participated, with mean duration since the start of hormonal treatment being over ten years. The main conclusion is that there is no reason to doubt that SRS is effective in ameliorating the patient’s gender-related distress. Other personal and social problems were much less influenced by SRS, and female-to-male transsexuals were found to be better adjusted socially (criteria: relations, work, sexual satisfaction, and loneliness). Psychic functioning was characterized by high scores on negativism, shyness, and psychopathology (delusional, paranoid, and bizarre thoughts), and this did not change after SRS. For male-to-female transsexuals, SRS proved to be a major health risk: in a group (mean age 37), 11 out of 105 had died at eight-year follow-up, with myocardial infarction as the most common cause. There is a great need for psychological help on nongender issues such as loneliness and shyness.
Verschoor (1990), a founder of the Amsterdam gender team, reported on a comparison of biographic questionnaires from SRS clients, transvestite members of the NVSH self-help groups, members of the homosexual organization COC, and controls. The youth of the transvestites appeared less conflicted than those of the transsexuals and homosexuals. Two thirds of the transvestites are married, often with resulting major problems in the relationship. Cross-dressing is sexually arousing for most transvestites. Progression towards transsexual wishes is uncommon - the transvestites in this group are certainly a selected group. For some transvestites, there is a link With S-M.
In 1984, Slijper studied female Congenital Adrenal Hyperplasia (CAH) patients (aged 6 to 16), comparing them with type I diabetes patients and controls. Diminished sex dimorphism in behavior correlated with severity of health problems (e.g., more pronounced in the salt-losing variant of CAH) and with the degree of their parents concern with the illness, especially the gender-confusion aspect. Genital virilization itself does not correlate with degree of tomboyism. In 1992, ten patients aged 16 to 33, were reevaluated on sexual and relationship experience and sexual anatomy. Self-pleasuring was frequent in seven. While gender-role behavior had been masculine throughout primary and secondary school, self-expressed sexual orientation was heterosexual in all. Yet, falling in love and sexual experience with partners was very rare. Only three women menstruated regularly. In contrast with the patients’ conviction that their genitalia were normal, adequate functional anatomy was found in only four.
A. Coercive Sex
Child Abuse, Incest, and Pedophilia
Years of feminist activities directed at sexual violence resulted in 1982 in a large-scale government-organized conference to develop policies for future years. Since then, sexual violence has been high on the political agenda. Research flourished, volunteer movements were supported financially, the concept of expertise through personal experience was widely acknowledged, public attention was raised by mass-media campaigns, a network of confidential doctors for the anonymous reporting of child abuse was set up, and education for helping professionals was made available all over the country. In psychiatric hospitals, a more profound interest in the patient’s sexual-abuse history is growing. Knowledge of the more complicated reaction patterns of childhood abuse, such as dissociative disorders, is expanding. More incest cases were brought to court, and perpetrators were sentenced to heavier penalties - the legal maximum being six years. A modest attempt with outpatient psychological help for perpetrators of sexual abuse was started, as an adjunct to the already existing residential compulsory programs for mentally disturbed violent sex offenders. A systems approach was introduced, in which all family members are supported by their own therapist, who work together to integrate the therapeutic process.
In the mid-1980s, Draijer (1990) carried out a nationwide representative study of female child sexual victimization by family members with in-depth interviews of 1,054 women, ages 20 to 40. This was 50 percent of all women approached. Intrafamily sexual abuse before age 16 was reported by 15.6 percent. For 25 percent, this study was their first discussion of these events. On a severity scale, 55.6 percent were found to be mild or not severe; 44.4 percent were classified as severe or very severe. (Step) fathers were the most inclined to commit more-intrusive forms of abuse. The level of education, level of professional occupation, religion, and geographical isolation were insignificant predictors. Family backgrounds that correlated significantly with incest included: conservatism in male-female roles, restricted sexual norms, child emotional neglect, lack of physical warmth in child rearing, discontinuity in family life, physical aggression, illness, depression, emotional instability of the parents, and the father’s possessiveness and controlling tendency. Sexual victimization correlates with problems in later life in a much higher degree than all other negative family dynamics. Only 13 percent had no negative effects whatsoever.
Child sexual abuse outside the family has gained less attention (see Section 5B). In the 1970s, because of society’s greater tolerance for all sexual expressions, pedophilia was for some years less tabooed. A public discussion about adult-child sexual contact on a nonexploitative base was then possible. Since the legal reform of 1991, adult sexual contacts with boys aged 12 to 16 are felonies only if the boy or his legal representative wants prosecution: maximum penalty is six years. Gender equalization of pubertal sexual rights was also part of this reform.
Following a low in child sexual-abuse cases reported in 1983, there has been a steady increase in both reported cases and the percentage of cases prosecuted. In 1989, cases of child sexual abuse by nonfamily members or authority figures was 1.9 per 100,000 inhabitants.
Male victims of childhood sexual abuse come out of the closet much later than females. The double taboo on homosexuality and powerlessness results in massive shame and repression. Volunteer and professional help for male victims is more difficult to find. Some child-abuse cases attract a lot of the general public’s attention, especially the difficulties in truth finding, e.g., the use of interviews with the so-called anatomically correct dolls.
B. Sexual Harassment
Since the 1982 government conference on sexual abuse, sexual harassment has been recognized as a major problem in all sorts of organizations, including schools and business organizations. It has certainly become easier for workers to lodge complaints. Confidential counselors have been introduced in schools, and training of personnel managers and administrators on this issue is available all over the country. Verbal and physical misconduct on gender-related issues is extinct, but the general public’s recognition of the intolerability of such behavior is widely acknowledged.
One special type of sexual abuse requires mention: the sexual contacts between (para) medical professionals and their patients or clients. It has been found that women abused in childhood were often revictimized during therapy. Recently, extra attention has also be given to the mentally and physically handicapped. In the 1980s, ethical codes on this particular type of misconduct were formulated. In the 1991 law reform, medical and social work professionals were included with civil servants, teachers, youth leaders, and prison wardens in those faced with a maximum penalty of six years for abuse of authority.
C. Rape
Rape was an early target for the feminist movement in the 1970s. It took some years to convince police and the courts that rape cases deserved much more attention, and rape victims much more sensitivity during interrogation. Some rape characteristics shocked the general public, for instance, the almost universally denied fact that date/acquaintance rape is more common than stranger rape. A government-financed mass-media campaign in 1992 addressed young men on sexual coercion: “Sex is natural, but never self-evident.” Until 1991, Dutch law did not allow prosecution for marital rape. Sexual assault, meaning all other forced sexual acts except vaginal intercourse, is a criminal offense between husband and wife. This law reform has been a major target for emancipation action. Rape victims have also profited from the victim movement’s help initiatives and its achievements in training professional social and psychotherapeutic workers.
Maximum penalty in rape cases is eight years. The number of rape cases brought to the police is steadily rising. In 1991, 1,333 accusations (9 per 100,000 inhabitants) resulted in 858 rape cases (65 percent), 746 suspects, being cleared, a rather stable percentage over the years. For sexual assault, 2,427 accusations (16 per 100,000) resulted in 1,060 cases (43.7 percent) and 632 suspects being brought to court by the police.
D. Prostitution
Studies on prostitution are numerous, but almost all data are nonrepresentative. In Holland, prostituting oneself is not illegal, but creating the opportunity for prostitution, e.g., profiting from a brothel, is. In 1993, a legal reform lowered the sanctions and allowed local governments to formulate their own policies. Prostitute activists are dissatisfied with this reform, arguing that the new situation will not improve the prostitute’s legal position. In the last decade, a movement to abolish exploitation and improve working conditions (safety, hygiene, and privacy) was initiated. Prostitutes fear that the new legal situation will lead to registration and taxing (including a Value Added Tax [VAT]), which will again force the weaker group members into evading the law. Today’s urgent problems include the trade in women from Third World nations, exploitation, illegal immigration, and fraudulent parental claims by Antilles men for South and Central American girls intended to legalize their working for Dutch brothels, and violence.
The total number of prostitutes in the Netherlands has been estimated at 15,000 to 20,000, the vast majority being women. Some 10 percent are supposed to be streetwalkers, 30 percent in window prostitution, 30 percent working in a sex club, 15 percent in an escort service, and 15 percent work in their private residence. Drug addicts, including drug tourists, are numerous in the streetwalker group. Window and club prostitution are dominated by Caribbean, South-American, African, and Asian women. In recent years, condom use among these groups has been promoted by means of audiotaped messages. It is generally believed that today most prostitution intercourse is protected, with drug-addicted streetwalkers as the most likely exception.
In 1968, more than half of all single men and 12 percent of husbands refused to answer questions about paid sexual encounters. In both groups, 12 percent admitted to having visited a prostitute at least once. In 1981, refusal was almost nil and 11 percent admitted to having visited a prostitute at least once. Moreover, 19 percent of the married group, especially the younger-age group, had visited a sex club at least once. In 1989,13.5 percent of the male respondents reported having paid for sex at least once; 2.6 percent had had at least one paid sex experience in the past year.
In the 1989 study, visiting prostitutes seemed to be motivated more by the desire to maintain independence than by social inadequacy. For men in steady relationships, common motives are variation or a strong desire for special forms of sex their partner refuses them. Condom use seems almost to have doubled as a result of the safe-sex campaigns.
Male heterosexual prostitution is extremely rare in Holland, but one study of escort boys was published in 1989. In recent years, male strippers (“Chippendales”) have made a remarkable appearance in the entertainment world.
Male homosexual prostitution is estimated to count some 1,300 men, of which a large group must be relatively young. Some consider themselves true professionals, with a professional pride in working according to their own standards. Others are motivated largely by drug addiction and homelessness. Sexual orientation is problematic: most boys consider themselves to be heterosexual, which suggests limits on the behaviors they consider acceptable or not. Fortunately, these restrictions result in a rather low prevalence of unsafe sex; homosexual prostitution seems to be a minor risk factor in the AIDS epidemic. Unfortunately, this discrepancy between self-perceived sexual orientation and behavior can lead to resentment and violent outbursts. A boy who feels trapped, especially when a man wants to perform anal penetration, will sometimes commit violent acts against his customer, as this behavior is most threatening to his masculinity. In ten years, eighteen murder cases with this dynamic were reported in Amsterdam. Moroccan boys were overrepresented, and this may reflect high vulnerability for threats to their masculinity as a result of their Islamic culture.
E. Pornography
Pornography as a subject of public decency laws has almost completely disappeared from the legislative discourse since the 1960s sexual revolution movement. Feminist criticism of the misogyny obvious in a lot of pornography has been heard throughout the nation, but this did not influence legislation to any substantial degree. In the latest reform, the protection of children and women in the pornography-producing business has gained more impetus than the decency aspect. Penalties up to three months can still be given for public exposure of indecent materials, exposure to children under 16, and selling child pornography. Child-abuse laws are often applied in cases of the production of child pornography; maximum penalty: six years.
Child pornography has been under scrutiny as a result of allegations from the U.S.A., implying that enormous amounts of these materials were being imported from the Netherlands. It cannot be denied that in the mid-1980s, Holland produced and exported child pornography, some of which, especially heterosexual material, clearly qualified as hard-core. Yet, the American interest in Dutch pornography has all the characteristics of a witch hunt, exaggerating the numbers of victims. In 1989, six child pornography cases led to convictions.
The use of pornography is quite common. In the 1989 study, only 23 percent of the men and 55 percent of the women had no experience at all with erotic magazines or books, while 54 percent of the men and 12 percent of the women had watched pornographic movies or videos. The “new kids on the block” are erotic pay-phone lines (06-numbers); 12 percent of the men and 4 percent of the women reported having phoned a sex line. This erotic option has become an addiction for some Dutchmen. Recently alcohol-and-drug services have begun treating some of their patients for 06-phoning problems.
F. Other Unconventional Behaviors
Some paraphilic behaviors are well embedded in society. Transvestites, for instance, have formed groups, often with transsexuals, for mutual support and opportunities to cross-dress without the risk of ridicule or violent reactions. People interested in sadomasochistic sexual contacts have formed two national organizations, and numerous sex clubs offer opportunities for expression. Gay and lesbian S-M groups are also active, and one occasionally sees some very aesthetic expressions of the S-M preference, especially in photography.
Indecent exposure is the most common sex crime; in 1990, 1.8 percent of all women were confronted with an act of exhibitionism. The number of reported cases shows a slow decline: 3,840 in 1991 (26 per 10,000). Only 30.5 percent were brought to court by the police. Exhibitionism complaints often result in a warning, and when brought to court, suggestions for some sort of therapy will often be the judge’s sentence. Unfortunately, no studies of results of court-ordered out-patient treatment of exhibitionists are published.
A. History
Contraceptive advice in Holland started in the 1880s. The inspiration for a Neo-Malthusian League was imported from the United Kingdom by Alette Jacobs (1854-1929). This remarkable woman, the first Dutch woman ever to enter secondary school, the university, and become a medical doctor, was strongly influenced by feminist ideals and a heartfelt concern for the poor. The League, founded by Jacobs and two other doctors, found little support and more often violent opposition in medical circles.
After Mensinga invented the diaphragm in 1881, this became the main weapon in the struggle against large, poor families. Free clinics started in Amsterdam in 1882, and soon afterwards in Rotterdam and Groningen. The Neo-Malthusian League produced leaflets and books in enormous numbers. Some midwives joined the clinics, and from the 1890s on, lay women were trained in instructing and prescribing the diaphragm. The clinic network expanded rapidly, as condom quality improved and more precise information on the Ogino-Knaus method of periodic abstinence became available.
In 1939, the Neo-Malthusian League performed Holland’s first socio-sexological research, distributing 26,010 questionnaires to its members; 7,788 were returned and analyzed (Nabrink 1978); see Table 10 for some results of this survey.
Table 10
Contraceptive Use and Failures in 1939 (n =
7,788)
|
Method |
Females |
Males |
||||
|
|
n |
Failures |
% |
n |
Failures |
% |
|
Coitus interruptus |
155 |
29 |
18.7 |
165 |
46 |
27.9 |
|
Diaphragm |
1,484 |
75 |
5 |
1,409 |
44 |
3.2 |
|
Condom |
1,105 |
67 |
6 |
1,036 |
79 |
6.7 |
|
Cervical cap |
95 |
19 |
20 |
91 |
12 |
13.2 |
|
Patentex jelly |
56 |
20 |
35.7 |
61 |
20 |
32.7 |
|
Periodic abstinence |
56 |
12 |
21.4 |
53 |
17 |
32 |
Following the introduction of the oral contraceptive in 1962, general practitioners and gynecologists were initially reluctant to prescribe the pill, sometimes for reasons blatantly moralistic. The NVSH consultation bureaus soon became a well-known alternative for teenagers, unmarried couples, married couples who wanted to postpone procreation, widows, and divorcees. Professional expertise in the NVSH bureaus was also on a higher level in those pioneering years. In 1969, the society separated into a professional organization for the management of the consultation bureaus, the Rutgers Foundation, and a layman’s organization for political action, education, and discussion and self-help.
Since the mid-1970s, contraceptive advice has become part of the regular physician’s routine; gynecologists play a minor part in contraception in Holland. The Rutgers Foundation still was a useful alternative for girls and women who sought extreme discretion (e.g., young girls and women in extramarital relations whose spouses had vasectomies) and for more specialized questions on contraception and “second opinions.” Since 1992, the Rutgers Foundation has concentrated its services in seven large cities, and guides its efforts more to educating the regular providers of contraceptive and sexological services.
From the mid-1960s on, contraceptive use and attitudes have been major research issues. Unwanted pregnancy and induced abortion caused major social, medical, and political concern. Accordingly, in the past two decades, questions about contraceptive use and the prevalence of unwanted pregnancy were almost always included in surveys, particularly those for adolescents.
Several studies directly addressed the issue of family planning. Initially, research was mainly done by general practitioners and family-planning doctors. Social scientists entered the field a few years later. A 1974-75 representative study, involving 1,200 men and women, revealed that modern methods of family planning had been rapidly accepted, irrespective of social status or religion. NISSO did several studies in close collaboration with Stimezo-Nederland, the national abortion federation, which began its own research program in 1974. The role of induced abortion in society was studied as it related to changing patterns of family formation, sexual behavior after the “sexual revolution,” and emerging modern contraceptive behavior. An international comparative investigation of the consequences of legal changes regarding abortion in Western Europe and the U.S.A. was followed by a study of contraceptive behavior throughout Western Europe (Ketting 1990).
In 1986, NISSO started a new research program on family planning, concentrating on specific groups. Studies published prior to 1993 include:
· Anthropologically inspired in-depth interviews on sexual and contraceptive behavior of Turkish immigrants;B. Some Data· A similar study on Caribbean immigrants;
· An in-depth study of the social and psychological mechanisms underlying the effectiveness of contraceptive behavior of young girls at the start of their sexual careers;
· A study on the rather new phenomenon of women’s ambivalence towards child bearing; and
· A representative study of the experiences of 1,200 women with, and attitudes towards, oral contraception.
Vogel and van der Vliet’s 1990 study on adolescent sexuality gave a lot of information on contraceptive use and the various motives for the use of condoms. They concentrated on contraceptive motives, although this distinction is not always possible.
Mean age for first coitus in this survey was 17.5. In this first coital experience, 57 percent used a condom. The earlier first coitus occurred, the higher the proportion of condom users. Allochtonous youngsters scored lower especially when not born in the Netherlands. In the older age groups, as relations become steady, oral-contraceptive use is the rule, and condom use for STD/AIDS prevention loses most of its impetus.
Many girls are using oral contraceptives before their first coitus. One in five girls are taking the pill by the time they start petting naked. (A prescription for medical reasons, e.g., menstrual discomfort, may account for a proportion of this number.) Two thirds of all girls with some coital experience have at some time used the pill; 60 percent were using oral contraception when interviewed. When first intercourse was experienced at an early age (11 to 13), the percentage was lower (just over 10 percent); in the oldest group, almost three quarters were current users.
In keeping with the Dutch slogan, “If you take care of the condoms, I’ll take care of the pill,” combined use of the pill and condom was practiced by 13 percent of respondents (boys: 18 percent, girls: 9 percent) in their last intercourse experience. The 14 to 15 age group is most conscientious in this regard, 22 percent. The use of no contraception at all is rare; only 11 percent of 16- to 19-year-olds used no contraception in their last sexual intercourse (see Table 11).
Adults
Van Delft and Ketting (1992) have reported the most recent number data from 1988: Of the 18- to 37-year-old women, 43 percent used an oral or injectable contraceptive, 22 percent no contraceptive, 7 percent each for the condom or vasectomy, 5 percent each for vasectomy and IUD, and 3 percent tubal ligation. Only 13 percent of the married women, 5 percent of the cohabiting women, and 14 percent of the women in steady relationships used no contraceptive (Tables 12 and 13).
Table 11
Pregnancies per 1,000 Unmarried Women, Grouped According to
Consequences, 1980-1988
|
Year |
“Forced” Marriage |
Birth Out of Wedlock |
Abortion |
Total |
|
1980 |
2.8 |
2.4 |
5.3 |
10.5 |
|
1981 |
2.9 |
1.9 |
5.3 |
10.1 |
|
1982 |
2.5 |
2.1 |
5.1 |
9.7 |
|
1983 |
2.3 |
2.2 |
5.3 |
10.0 |
|
1984 |
2.1 |
2.0 |
4.4 |
8.5 |
|
1985 |
1.9 |
2.0 |
4.4 |
8.4 |
|
1986 |
1.9 |
2.1 |
4.1 |
8.1 |
|
1987 |
1.6 |
2.3 |
3.8 |
7.7 |
|
1988 |
1.6 |
2.3 |
3.8 |
7.7 |
Source: Van Delft and Ketting (1992), Table 22, p. 61Table 12
| Contraceptive Method |
Age of Women (in Years) |
Total 18-37
|
||||
|
18-19 |
20-24 |
25-29 |
30-34 |
35-37 |
||
|
Oral-injectable |
45 |
59 |
48 |
31 |
22 |
43 |
|
IUD |
1 |
2 |
5 |
9 |
6 |
5 |
|
Tubal ligation |
0 |
0 |
1 |
6 |
11 |
3 |
|
Vasectomy |
0 |
0 |
3 |
12 |
23 |
7 |
|
Condom |
5 |
5 |
9 |
9 |
8 |
7 |
|
Other methods |
4 |
6 |
4 |
5 |
3 |
5 |
|
No contraceptive |
45 |
24 |
19 |
16 |
15 |
22 |
|
Pregnant |
0 |
3 |
9 |
6 |
2 |
5 |
|
Infertile |
0 |
1 |
2 |
6 |
9 |
3 |
Source: van Delft and Ketting (1992), Table 1, p. 10Table 13
|
Contraceptive Method |
Married |
Cohabiting |
Steady Relationship |
No Male Partner |
|
Oral-injectable |
35 |
68 |
67 |
28 |
|
IUD |
7 |
7 |
3 |
1 |
|
Tubal ligation |
5 |
2 |
2 |
1 |
|
Vasectomy |
13 |
3 |
1 |
- |
|
Condom |
9 |
6 |
6 |
4 |
|
Other methods |
4 |
5 |
6 |
4 |
|
No contraception |
13 |
5 |
14 |
58 |
|
Pregnant |
9 |
4 |
1 |
0 |
|
Infertile |
5 |
1 |
1 |
3 |
· American data often report method failure in the first year of use. Most methods gain in reliability in time;It is generally acknowledged that U.S.A. data on method failure cannot be used for Dutch educational materials (Table 14).· The “morning after pill” is easily available in Holland and is used by women who are aware something has gone wrong with their usual method;
· Some American data may be distorted by including users who deliberately stopped using the method.
Estrogen dose-dependent side effects, especially cardiovascular ones, led to the introduction of the so-called sub-50s in 1975. In five years, they became the leading oral contraceptive. Today, most physicians prescribe sub-50s. This seems to work reasonably well: abortion data show that women on 50s and sub-50s have comparable risks of unwanted pregnancy.
Concern over the pill’s side effects around 1980 led to a short but sharp decline in pill use. Introduction of sub-50s largely removed this concern. Today, most women are aware of positive side effects. Nevertheless, total oral-contraceptive use once again showed a slight decrease in 1990. Condom use for STD and AIDS prevention may have led some women to stop or postpone oral contraception. The decline in popularity of hormonal contraception led to a short increase in IUD use (Table 15).
Gynecologists and the Rutgers Foundation were the early providers for IUDs. From 1983 to 1987, the Dutch industry producing the most popular IUD ran educational workshops for physicians, increasing the use of IUDs. Early on, there was an awareness of negative side effects, menstrual discomfort, and a rising number of extrauterine pregnancies.
Table 14
Distribution of Hormonal Contraceptive Use by Type of
Method, 1980-1989, in Percentages
|
Year |
Sub-50 Combination |
Tri-phasic |
50 (-plus) |
Injectable |
Others |
|
1980 |
41.9 |
0.1 |
46.7 |
4.3 |
7.0 |
|
1981 |
47.5 |
5.6 |
36.5 |
4.8 |
5.6 |
|
1982 |
55.6 |
10.1 |
25.3 |
4.7 |
4.3 |
|
1983 |
57.2 |
14.8 |
20.4 |
3.9 |
3.7 |
|
1984 |
58.7 |
18.8 |
16.6 |
2.8 |
3.1 |
|
1985 |
69.7 |
20.8 |
14.5 |
2.4 |
2.6 |
|
1986 |
61.0 |
22.1 |
12.5 |
2.2 |
2.2 |
|
1987 |
61.4 |
23.8 |
11.2 |
1.8 |
1.8 |
|
1988 |
61.7 |
25.2 |
8.2 |
1.6 |
2.0 |
|
1989 |
62.8 |
25.2 |
8.2 |
1.6 |
2.2 |
Source: van Delft and Ketting (1992), Table 11, p. 26Table 15
|
Year |
Number Sold |
Mean Years in Situ |
|
1980 |
100,000 |
2.00 |
|
1981 |
97,000 |
2.25 |
|
1982 |
79,000 |
2.50 |
|
1983 |
78,000 |
2.75 |
|
1984 |
77,000 |
3.00 |
|
1985 |
67,000 |
3.25 |
|
1986 |
48,000 |
3.50 |
|
1987 |
45,000 |
3.75 |
|
1988 |
40,000 |
3.75 |
|
1989 |
39,000 |
3.75 |
|
1990 |
38,000 |
3.75 |
The diaphragm was never very popular after World War II, being used predominantly by women in steady relationships and dissatisfied with alternatives. It has its place in a lifestyle characterized by conscious living with health risks. In small circles, modified and perfected forms of periodic abstinence are also used. We have no reason to suppose that Roman Catholics are a large proportion of abstinence users. In 1992, the woman’s condom (Femidom) was introduced. Among 300 women, ages 21 to 40, who were regular users of oral contraception, IUD, or sterilization during the trial period, 155 women reporting using Femidom on at least three occasions. Both men and women appear reasonably satisfied with the Femidom.
Surgical sterilization peaked in 1979, when 132,000 men and women had vasectomies or tubal ligations. The proportion of men is growing steadily, because it is well known that sterilization is much easier in men. The operation is most often performed between ages 35 and 44. Since 1985, the percentages of sterilized men and women in each age group has been rather constant. In the 35 to 39 age group, 18 percent of women and 20 percent of men are sterilized; in the 40 to 45 age group, about 25 percent of women and men are sterilized; about 30 percent of men and women 45 to 49 have been sterilized. Forty percent of all couples aged 30 to 49 have one spouse sterilized.
In recent years, sterilization has decreased in the younger age group, most probably due to an ongoing tendency to postpone having a first child. Also, some couples are debating for a number of years whether or not they want to have children at all. This has led to an expanding group of last-chance mothers with considerable fertility problems caused by a more advanced age. This group of doubters, combined with a growing conviction that oral contraception is not a major health risk, will likely lead to a further decline in sterilizations.
Interception with the “morning after pill” (MAP) and the “morning after-IUD” (MA-IUD) along with abortion, is one of the adjuncts of planned contraception. The MAP is easily available for use after unprotected intercourse, as well as for backup for incidental failures with the regular method. The largest group using MAP is the 16- to 18-year-olds. Around 1980, when the negative attitude toward the pill peaked, use of MAP also peaked. The original MAP (5x5 mg ethinyl estradiol) has been replaced with the Yuzpe regime (100 mg EE plus 500 mg norgestrel repeated after 12 hours) introduced in 1982. By 1986, the Yuzpe MAP accounted for 85 percent of MAP prescriptions. In 1986 and again in 1992, some doubt was cast on the effectiveness of the Yuzpe regime, leaving the future of this method open to question.
C. Abortion
Just over 30,000 abortions are performed yearly in Holland, a quite stable number in recent years. More than 90 percent are done in abortion clinics, almost all under local anesthesia; the rest are done in gynecology departments, 80 percent under total anesthesia. Among women living in Holland, 69 percent have their abortions within six weeks after conception; 2.2 percent were pregnant longer than fifteen weeks in 1989-90. Large numbers of abortion patients (35 to 40 percent) visit our clinics from western Germany, Belgium, Spain (showing a sharp decline since 1988), and numerous other countries.
Separate data are available from women in Holland, Suriname, the Dutch Antilles, Turkey, and Morocco. Abortion rates in these groups show significant, but rather stable differences, with a slight increase for the Moroccan and a slight decrease for Suriname, Antilles, and Turkish women (Table 16). Moroccan women tend to be relatively young, primigravidae, and unmarried; it is supposed that the rising number for Moroccan women indicates some alienation from their traditional culture. For Turkish women, data suggest that abortion is used mostly to put an end to the expansion of the family. Allochtonous women have used abortion more often than autochtonous women, and it must be assumed that this implies more user failures. Moreover, one third of these women had used no contraception at all compared with 20 percent for Dutch women. For allochtonous women, some 25 percent, the abortion in 1989-90 was not their first. For Suriname and Antilles women, it is recognized that they show more fear for unhealthy side effects of oral contraceptives. This leads to an eagerness to stop taking the pill, for instance, when a relationship falls apart.
Table 16
Abortion Rates, per Ethnic Groups, Ages 15-44, per
1,000
|
Ethnic Group |
Rate |
|
Autochtonous |
3.4 |
|
Surinam |
28.8 |
|
Antillies |
31.1 |
|
Turkey |
17.8 |
|
Morocco |
12.4 |
Source: Rademakers, 1992, Table 2.11, p. 20Teenagers as a group are constant in their risk of abortion in recent years, around 4 per 1,000 girls aged 15 to 19. Teenagers have shown a slight increase in live birthrates in recent years.
As Dutch couples conceive later in life, the number of prenatal diagnostic tests for fetal malformation and disease will rise, and so will the decision for an abortion to resolve an unfavorable outcome. Precise numbers of such abortions are not available.
D. Government Policies on Contraception and Population
In 1970, the Dutch Parliament decided that medical contraception and the cost of medical contraceptive advice should be included under general health services. Condoms are the only contraceptives that are not covered. Even in AIDS-prevention campaigns, a recommendation to include condoms has been ignored. In the recent economic recession, with a growing need to reduce health expenses, hormonal contraception is quite often mentioned as one possibility to cut costs. Thus far, these suggestions have led to strong reactions, especially because risk groups, such as minors and allochtonous women, will be the first to suffer the consequences of unwanted pregnancy and abortion.
In 1979, the Dutch government endorsed its State Committee on Population Questions recommendation that all Dutch couples were free to decide their number of children and the time they wanted to have them. Since then, the government has supported effective contraceptive behavior by stimulating and financing research, general education, and low-level professional help. The effectiveness of Dutch contraceptive practice is based on the opportunity for almost all young people to get the pill. Today, most general practitioners are able to handle the delicacy of prescribing the pill to young girls, even if their parents are not informed. In coming years, it will be learned whether or not unwanted pregnancy will increase as a consequence of the Rutgers Foundation’s concentration in seven cities.
Abortion was a criminal offense in the Netherlands until a long-awaited legal reform took place in 1982 - 1953 was the last time a physician was prosecuted for performing an abortion. In 1969, Stimezo, a national organization for medically qualified induced abortion, was formed. Stimezo standards of good advice and care have found their way into today’s practice. On the insistence of the religious parties, the 1982 law includes one aspect contrary to the practice of that time, e.g., a waiting and reconsideration time of five days after the initial consultation with a doctor. Since that law passed, abortion has been free for all Dutch citizens. Minors living with their parents need their parents’ consent, but a legal alternative is available.
Population planning is not an active concern of the Dutch government. Zero growth is accepted, and a changing population stratification (young groups shrinking, elderly groups growing) causes only moderate concern. Will the future active group be able to support a large retired population? In gynecological circles, some concern is growing about the tendency of couples to postpone having children until an age when fertility definitely is lower. A popular slogan, “A smart girl plans her pregnancy in time,” is a variation of an earlier advertisement by the Institute for Idealistic Propaganda: “A smart girl is prepared for a future for herself.”
A. Incidence, Patterns, and Trends
According to Mooij’s (1990) history of STD, gonorrhea and syphilis were rare in the Netherlands in comparison with the surrounding countries - until 1942. During World War II, a rapid increase was reported, with a peak in 1947. In 1952, numbers were again as low as they were in the 1930s. A steady decline was observed until 1960, but since then, a second, and longer, epidemic has occurred, with rapid increases in the 1970s. Undoubtedly, these growing numbers were the result of a new enthusiasm for sexuality, the sexual revolution, supported by the general public’s knowledge that STDs were now easily cured. Public education almost forgot primary prevention in these years.
The sexual revolution certainly changed the medical and health professionals’ ideas on specific risk groups. Prostitutes were no longer the main source of concern; homosexuals, teenagers, foreigners, and Dutch tourists who had sex while vacationing abroad became new targets for information campaigns. It is remarkable that these predictions, based on information from abroad, were not confirmed by Dutch experience, except for homosexuals, and recently Turkish and Moroccan men.
The neglect of primary prevention gradually ended when hepatitis B and herpes, which are not curable by penicillin, appeared. Herpes caused considerable panic in heterosexual circles. Alarming data from the U.S.A. were uncritically transposed to Holland and connections with cervical cancer and neonatal disease exaggerated. The number of diagnoses peaked in 1985, perhaps biased by a more widespread availability of diagnostic services and an antiviral medication that might have prompted people in fear of herpes to be finally tested. In this peak year, the number of herpes cases at the Amsterdam free clinic was 25 percent of the number of gonorrhea cases. Today, herpes is infrequently diagnosed and the attention paid it by the general public and media is insignificant. However, it is reasonable that herpes promoted a growing concern for primary prevention in the 1980s, as the sharp decrease in STD diagnosis started some years before AIDS appeared.
Two STDs are among the infectious diseases for compulsory notification to the National Health Inspection: gonorrhea and syphilis. Unfortunately, only about 35 percent of all cases are reported. Free clinics have a more complete reporting, including data on location of the disease (urethral, rectal, and/or pharyngeal), ethnic background, sexual preference, prostitution, and earlier infections. Unfortunately, they have no information on the characteristics of groups using their services, and whether or not this group’s composition is stable or changing.
National registration numbers for gonorrhea steadily decreased from 13,199 in 1983 to 3,024 in 1989. The peak year for men was 1981 (140 per 100,000 inhabitants); for women, 1984 (65 per 100,000). An increase in 1990 was followed by the lowest number ever in 1992. In free clinics, similar trends were observed. The fastest decreases were among male homosexual and bisexual men, since 1984. Female prostitutes showed a little slower decrease, and later - since 1985. For homosexual and bisexual men, 1989 already showed some increase, including more anorectal infections, and unfortunately this trend has continued into 1990 and 1991. Moreover, these patients tend to be slightly younger in recent years.
For the Amsterdam free clinics, repeaters are a growing population in the total numbers. Percentagewise, homosexuals are declining and prostitutes are increasing. In all years, the peak age for male infections is 25; for women, age 20.
The percentage of Penicillinase-Producing Neisseria Gonorrhoeae (PPNG) in Dutch patients is steadily increasing. The first cases of PPNG were reported in the Netherlands in 1976; in 1990, 29 percent of all gonococcal infections was caused by PPNG. Since 1985, a rapid increase in Tetracycline-Resistant Gonorrhea (TRG) has been observed. In 1989, 40 percent of PPNG cases also involved TRG.
Syphilis was still decreasing in 1992, with only 190 new infections reported. In Amsterdam free clinics, in 1987, an increase in syphilis incidence was reported in heterosexual men, and some increase in female prostitutes. In that year, heterosexuals for the first time outnumbered homosexuals. In 1989, homosexual men in Amsterdam also showed an increase in new cases of syphilis, similar to tendencies in gonorrhea and seroconversions, perhaps due to a decrease in safer-sex practices.
In Holland, since the early 1950s, all pregnant women are screened for syphilis in the first trimester. In the Amsterdam area, 1985-89, only 55 out of 3,520 blood samples were positive for both TPHA- and VDRL-tests. Only four cases of congenital syphilis were reported in 1990. However, screening is still cost-efficient in Amsterdam, and a second screening later in pregnancy should not be introduced as a routine restricted to women having many partners during pregnancy.
Chlamydia trachomatis probably is the most widespread STD today, but information is scanty on this subject since reporting it is not mandatory. The most thorough research took place in 1986-88. In a 1986-88 Amsterdam free clinic survey of 1,000 clients (65 percent male) at the free clinic, chlamydia was found more often than gonorrhea: 14.3 percent versus 11.5 percent in men, 19.2 percent versus 6.3 percent in women. Combined infections were found in 2 percent of men and 2.6 percent of women. Combination infections were low in homosexual men. In men, signs for urethritis were found in all but 1, with negative tests for gonorrhea and chlamydia in 41 percent of the cases. In the department of gynecology of a large Amsterdam hospital, 1985-89, the incidence of gonorrhea dropped from 1.1 percent to 0.4 percent, and chlamydia from 8.6 percent to 4.1 percent.
While chlamydia definitely is the most common STD in Holland, there are good grounds for concluding that the epidemic has peaked. However, the serious consequences for fertility justify further efforts to control the disease. In 1986, in the Tilburg Infertility Clinic, of seventy-seven women receiving their first treatment, tubal abnormality was thought to be the cause of infertility for sixty-nine; 54 percent had significant titers for chlamydia.
Data on condylomata acuminata are rarer, with indications that incidence is in the same range as herpes, increasing slightly up to 1985 and decreasing in recent years. Tropical STDs are rarely diagnosed in Holland, with occasional small epidemics of haemophilus ducrei.
Allochtonous men are a growing proportion of free clinic customers. Data suggest that Turkish and Moroccan men are six to ten times more at risk for contracting STDs. Turkish men have gonorrhea in a high proportion and a high proportion of PPNG. They also report prostitution as the source of their infection in a higher percentage. Suriname and Antillian men show a higher proportion of syphilis.
B. Government Policies Concerning STD
The Dutch government has recognized STDs as a special group of diseases, with associated shame and stigma calling for special forms of illness management. Alternatives for discreet and anonymous help have been financed. Local health services provide free clinics in all large cities; the Rutgers Foundation is another alternative for STD diagnosis and treatment. For syphilis and gonorrhea, a service is offered to assist patients anonymously in contacting the sexual partners they think they have infected or been infected by.
A national organization for STD control, the SOA Foundation, produces a scientific bimonthly and contributes to the discussions in medical and political circles, and to prevention programs. In the last decade, physicians’ organizations have produced consensuses for standard medical care. More intensive health and STD education programs have been incorporated in a framework of sexuality and relationship management in schools. STDs other than AIDS have never been the target for specific primary prevention programs until recently. The SOA Foundation has applied for funding for a Chlamydia Public Information campaign, but this has not been forthcoming. Target groups other than teenagers in schools also have never been defined for prevention programs on STDs other than AIDS. Special attention to allochtonous groups can be justified by these groups’ higher infection rates, and their higher proportion of PPNG.
A. Incidence, Patterns, and Trends
Unlike syphilis and gonorrhea, notification of AIDS cases to the National Health Inspection is voluntary. While syphilis and gonorrhea cases are underreported, AIDS reporting tends to be almost complete because of the serious nature of the epidemic. Many intravenous drug users die of health risks inherent in their lifestyles before their HIV-positive status is detected. Starting with 5 new cases of AIDS in 1982,437 cases were reported in 1991 and 419 in 1992. Only 10 cases of HIV-2 infection were reported. Homosexual men, followed by IV drug users (male and female), and heterosexual men and women, account for most AIDS cases, with the incidence remarkably stable through the years. Men ages 30 to 45 and women 25 to 35 are most at risk. Survival time has increased from nine months in 1982-85 to twenty-two months in 1989, because of earlier diagnosis and better treatment (Tables 17 and 18).
Table 17
Number of Newly Diagnosed AIDS Patients per
Year
|
Year |
New Patients |
|
1982 |
5 |
|
1983 |
19 |
|
1984 |
31 |
|
1985 |
66 |
|
1986 |
136 |
|
1987 |
242 |
|
1988 |
321 |
|
1989 |
389 |
|
1990 |
413 |
|
1991 |
437 |
|
1992 |
419 |
|
TOTAL |
2,478 |
Source: National Health Inspection, 1993The number of HIV-positive persons in Holland is unknown. Individuals may be tested anonymously, in which case their status is not reported. Some data is available on segments of the population from research groups studying pregnant women, drug users (30 percent of whom are IV users), clients at the Amsterdam free STD clinic, Amsterdam prostitutes and their customers, and voluntary applicants for blood donation.
Table 18
Number of AIDS Patients, According to Risk Group and
Sex
|
Risk Group |
Male |
Female |
|
Homosexual-Bisexual |
1,930 |
- |
|
Intravenous Drug User |
145 |
67 |
|
Homosexual-Bisexual + IVDU |
26 |
- |
|
Hemophilia |
40 |
1 |
|
Blood Transfusion |
20 |
15 |
|
Heterosexual |
108 |
74 |
|
Mother-to-child |
2 |
9 |
|
Rest/unknown |
33 |
8 |
|
TOTAL |
2,304 |
174 |
Source: National Health Inspection, 1993In a national prospective research project on HIV-infection in pregnancy, testing is voluntary and the percentage of women choosing to be tested varies widely for different hospitals. Between September 1, 1985, and January 1,1991, fifty-five women were found to be positive: 60 percent were not born in Holland. In 58 percent, intravenous drug abuse was the risk factor; in two of the twenty-two women supposed to be heterosexually infected, blood transfusion was also reported. Ten were born in an area where AIDS is endemic; seven had at-risk male partners. Of thirty-six women for whom test results were known before twenty weeks of gestation, two had spontaneous and ten induced abortions.
Among the estimated 2,500-plus hard-drug users in Holland, only 30 percent are IV users. IV use varies from practically zero among allochtonous groups to 70 percent for “heroin tourists.” Combining results of a cohort survey amongst injectors in Amsterdam started in 1985 with reported AIDS numbers resulted in an estimation of 750 to 800 HIV-positive IV drug users in Amsterdam as of July 1, 1991. Even more rough is an estimate of HIV-positive IV drug users outside Amsterdam, ca. 500. Local differences are large and unexplained: Participants in a detox clinic in the Hague were all seronegative, while their injection behavior was no more risky than an Amsterdam group. Prevalence of seropositivity among all IVDUs is estimated at 25 to 27 percent. Specific preventive measures include a syringe-exchange program and condom promotion, especially for those active in prostitution (some 80 percent of all female IV drug addicts).
In an Amsterdam free STD clinic, during ten weeks in 1991,90.5 percent of all the patients accepted testing: 22 percent of the homosexual men were positive, as were 12 percent of the male and 41 percent of the female IV drug users. Prevalence in heterosexuals without other risk factors was 0.5 percent (5 of 997) for men and 0.1 percent (1 of 771) for women.
When prostitutes and their customers were tested in Amsterdam in 1991, three (from Ghana, Nigeria, and the Dominican Republic) of 199 prostitutes were HIV-positive. One customer who admitted to homosexual contacts was HIV-positive.
Blood-donor volunteers in any HIV risk group are asked not to donate. In 1985, fifteen donors were found to be HIV-positive; in 1990, the new discouragement policy resulted in only five infected donors. This procedure does not totally exclude HIV transmission by blood transfusion, because of latency between infection and seropositivity. Blood products for hemophiliacs have been heat-treated since 1985, so this is no longer a risk group. Early in the epidemic, about 13 percent of hemophiliacs were infected.
B. Effectiveness of Prevention Education Programs
In a sample of 1,013 homosexual men in Amsterdam followed since 1984, an extensive change in behavior has been documented in two directions: a decrease in the number of sex partners and a lower prevalence of anogenital contact. These behavior changes resulted in a decline in sero-conversions to almost zero in 1987. However, since the end of 1989, there is an increase in the incidence of HIV infection in the same cohort. Interviews with this group revealed that higher percentages of both sero-positives and seronegatives had had anogenital sex without protection, especially in casual sexual relations.
In recent years, AIDS health promotion has changed its message from “avoid anal sex” to “avoid unprotected anal sex.” The availability of special condoms for anal intercourse has been a major factor in this development. Recently, condom efficacy was studied among cohort members. Condom failures (torn, slipped) were seen more often when vaginal condoms were used or when no lubricants, or oil-based lubricants, were used. Personal efficacy prevents failure by slipping, but not by tearing the condom. In-depth interviews with men who seroconverted indicate the significant role of the use of alcohol and other drugs, as well as the divergent individual background of each seroconverter. Personality factors, like coping styles and health locus of control, seemed to be almost completely unrelated to behavioral change. Preceding sexual behavior seems to be the best predictor of actual behavior.
In a quasi-longitudinal telephone survey, changes in beliefs, attitudes, and behaviors related to AIDS were followed from early 1987 onwards. Knowledge regarding the use of condoms to prevent HIV transmission increased to a level that can be considered sufficient by the end of the 1980s. The general population seems to opt for monogamy and condom use as preventive measures. The use of condoms rose, especially among teenagers and persons in nonsteady relationships. These observations were confirmed by condom sales figures and STD incidence. However, there seems to remain a discrepancy between the inclination to use condoms and the actual use.
In the 1989 study, sexual behavior of 1,000 respondents is described in the context of HIV transmission as it relates to: potential risk, awareness, knowledge, and endorsement of misconceptions on transmission. Based on sexual behavior, 12 percent should be considered to have taken at least some risk in the year preceding the interview. Of these 124 subjects, 58 percent completely ruled out the chance that they might have been infected. In general, the level of knowledge is rather high. The knowledge of the subjects who have been at risk ironically is slightly greater than average. This might imply that more intensive prevention strategies should be directed at subgroups who are relatively more at risk.
In the 1989 teen study, sexual mores are found not to be changed by AIDS. To avoid HIV infection, teens prefer postponing sex till one has found the right partner or using condoms during intercourse. In general, however, in fact youngsters do not postpone their first sexual contact. Only a few of those who advise the postponing of sex have had unsafe sexual contacts. Half of those recommending the use of condoms do not stick to their own advice. Condoms are used especially in the beginning of affairs; but later on, many couples switch to oral contraceptives to avoid pregnancy. Moreover, a questionnaire survey among school children revealed that intentions of consistent condom use for HIV prevention decreases with the amount of actual intercourse experience. They seem to ignore the fact that their relationship career will most likely be characterized by serial monogamy. This research suggests more attention to efficacy aspects of condom use: buying them, raising the topic with a new partner, etc.
Based on a theory of sexual networks, 60 percent of the 18- to 19-year-olds seems to run no risk whatsoever of getting infected with HIV. This network analysis research is a promising new branch of sociosexual study. Other new approaches are studies on negotiations between male and female prostitutes and their customers to find out to what extent they could take health-promoting measures.
C. Treatment, Prevention Programs, and Government Policies
Since the onset of the AIDS epidemic, an elaborate system of care and prevention for homosexual men has been developed in the Netherlands. The gay community took the initiative for the first nationwide AIDS education campaign (1983) aimed mainly at homosexual and bisexual men. Also in 1983, an ambulatory venereal disease and AIDS clinic for homosexual men was started in Amsterdam, the Supplementary Services Foundation (StAD), supplementing regular services.
In 1984, as the AIDS epidemic spread among gay men, the StAD started a small-scale primary prevention course for gay men, aimed at altering sexual habits. This was modeled after an American example and was successful throughout the country. The foundation still organizes numerous prevention activities aimed at gay men, such as safe-sex workshops, video workshops, shows in gay bars, and activities in gay cruising areas (parks, public toilets). Postgraduate education programs and material on AIDS have been produced by StAD and a number of Amsterdam physicians who have many AIDS patients. Doctors employed by the StAD support some of the doctors in Amsterdam with the heaviest burden of AIDS patients by taking over office hours and home visits.
Another important gay health-care institute is the Schorer Foundation. In the AIDS field, the foundation has offered psychosocial care for gay men and their friends and families since 1984. It also initiated, and now coordinates, the “buddy” home-care projects all over the country. This project offers AIDS patients free volunteer support at home. The foundation also produces education programs and training courses for workers in psychosocial health care.
Although these gay organizations are important care providers, most gay men with AIDS make use of general health institutions such as general practitioners, district nurses, hospitals, psychiatrists, and social workers. Therefore gay (and other) lifestyle elements need to be included in postgraduate education for all caregivers, to prevent communication problems. After all, HIV has no precedent as an extremely serious health and culture problem in the gay community.
The total number of women infected is smaller, but the progression is faster in women. Attention to women and AIDS seems to be restricted to their role as infectors (prostitutes, IV users, and pregnant women). In December 1990, on World AIDS Day, which was dedicated to women, it was observed that women should be the target for more and better campaigns for the prevention of AIDS, and that care for women should be improved. For some years, the Rutgers Foundation has provided short-term support and education groups for HIV-infected women.
Care for HIV-positive IV drug users is often complicated by aggravated addiction behavior, which often makes these patients difficult to deal and make appointments with. Municipal health centers and general practitioners in the big cities, and local clinics for the addicted, monitor a substantial percentage of IV drug users. This includes health education, education on HIV prevention, assessment of physical condition, and often also the prescription of methadone, a heroin substitute. A needle/syringe exchange program is an important part of prevention. Education for hemophiliacs and support for those infected has been helped by the very active national haemophilia patient association.
Treatment for HIV is evaluated nationally. Recently a national consensus on early Zidovudine (AZT) treatment was published. In the early years, testing was thought to be of limited value because no health gain was to be expected, and for preventive measures, the individual’s serostatus was supposed to be of no importance: safe sex should be practiced by seronegatives as well as seropositives. Today, early detection is expected to be effective, even if it does not change the patient’s sexual habits. Testing is always on a voluntary basis, and if the patient wants to be tested anonymously, this is always possible.
A policy decision currently under discussion is the desirability of contact tracing and notification in heterosexually infected cases of HIV, as is common practice for gonorrhea and syphilis. Because of low heterosexual prevalence, this approach might be highly cost effective.
A. General Views
Dutch clinical sexological practice follows the international framework of diagnosis and the DSM-III-R with some hesitance about the normative aspects of such procedures. Feminism and emancipatory trends have had an enormous impact on Dutch sexology. Health Care for Women projects have been substantially Financed by the government with sexuality a major area of concern. In recent years, most of these projects have been integrated, sometimes unwillingly, into the general mental health-care institutions. Health Care for Women is situated methodologically between self-help and professionalism. Group approaches are highly valued and the group-therapy approach used more often than for men.
Another concern inherited from Health Care for Women is the power issue in heterosexuality. Since the early 1970s, there has been a passionate plea for better help for sexual-violence victims, stimulated by independent nonprofessional self-help organizations. Dutch sexologists have responded by initiating discussion on professional standards and ethical codes on therapist-client sexual contact. Current interests include: sexual abuse of the mentally and physically handicapped, and introduction of sexological diagnostic and treatment approaches as an adjunct to personality-oriented diagnosis.
Desire problems: There is a modest amount of literature on desire discrepancies. The interactional aspect, the incapacity for intimacy, has gained most attention, along with unrealistic expectations and the balance of power. There is no literature available comparing male higher-libido with female higher-libido.
Arousal problems: The medical-sexological approach used with many cases of male erectile dysfunction has resulted in numerous articles but no relevant quantitative data. While clinical criteria are set by the Dutch Society for Impotence Research, concern is growing about over-use of methods prompted by cost and patient acceptance. Psychophysiological methods and pharmacoDuplex scanning are the most widely used methods; neuro-urophysiological, hormonal, and invasive methods are restricted to specific indications. It is widely recognized today that psychological inhibition can prevent the reaction on intracavernous vasoactive drugs, and that an erotic atmosphere enhances the reaction. Regarding treatment, a preliminary, cautious conclusion might be: Dutch men seem to be rather reluctant to accept prosthesis as a solution for erectile failure; intracavernous injections are acceptable for a larger group with a high discontinuation rate; vacuum devices are used, but here, too, discontinuation is high.
There is no specific literature on arousal dysfunction in women, except for a study on diabetes.
Orgasm problems: In 1977, the Utrecht psychology group enriched sexological theory by contrasting the “interaction phase” with the “solo phase” and emphasizing surrendering to one’s own feelings as essential during orgastic release. Lonnie Barbach’s group treatment is widely used for primary female anorgasmia, but there are no outcome studies. For female secondary and/or situational orgasm difficulties, sex therapists tend to prefer couple therapy. After analyzing 1,112 respondent questionnaires, De Bruijn (1982) tried to describe backgrounds of female anorgasmia. Among her conclusions: to some women, orgasm is simply not important in lovemaking; those regularly having orgasms during partner interaction tend to use techniques similar to their self-pleasuring techniques; in interaction, some women simply do not get stimulation long enough to attain orgasm; and orgasm by following the male’s movements in intercourse is the only stimulation technique in which orgasm is linked to feelings of love and intimacy. Her findings, published in a best-seller, have been widely acknowledged by both professionals and the general public. Ironically, the 1939 survey of NVSH members reported female respondents attributing differences in satisfaction found in men and women to the short duration of intercourse. Plus ça change, plus c’est la même chose.
Inhibited and premature male orgasm have received less attention. Premature ejaculation is common and treated by standard modalities, but no treatment results are published.
Coitus problems and genital phobias: Vaginismus, dyspareunia, unconsummated marriage, and phobic avoidance of vaginal penetration are subjects of intense interest, characterized by an increasing tolerance of the symptom’s hidden meaning. As early as 1917, Treub concluded that fear is the main cause and refrained from incision of the perivaginal muscles; in the 1960s, Musaph stressed the usefulness of psychoanalytical interpretations. During the 1979 World Congress of Sexology in Mexico City, Dutch women sexologists vented their annoyance with sexology’s neglect of sex-role bias. Cohen-Kettenis criticized medical and behavioral sexologists for having only one goal in the treatment for vaginismus: consummation. Bezemer was the first to report on group treatment for women suffering for vaginismus, together with other primary dysfunctions in one group. Moch (1987) broke the taboo on reporting relapse after successful treatment for vaginismus. Drenth (1988) pointed out that for some couples, vaginismus is a fertility problem and can be treated as such by artificial insemination. In 1989, Drenth also identified genital fears, phobias, and obsessions as the male counterpart of vaginismus, pointing out that phobic avoidance of genital play can result in pseudo-phymosis. In 1989, the Dutch Society for Sexology organized a symposium on Vaginismus and Dyspareunia: The Dutch View.
B. Availability of Diagnosis and Treatment
Historically, treatment for sexual problems in the Netherlands began in the Neo-Malthusian League. In the League’s counseling centers, psychoanalytic treatment of sexual problems was strongly influenced by Van Emde Boas and Musaph, pioneers in the Sexual Reform movement, until the 1970s. In 1969, when the Rutgers Foundation separated from the Dutch Society for Sexual Reform (the League’s postwar successor), treatment of sexual problems was very much still part of its activities. As demand increased, the foundation reorganized its staff in multidisciplinary teams.
Dutch gynecologists also played a major role, led by the internationally renowned Theodor van der Velde. His book, The Perfect Marriage (1925), was the first such work to find a large general public. Fertility studies led to the formation of the Society for Psychosomatic Obstetrics and Gynecology in 1979. All academic hospitals now have a sexological outpatient department. Unfortunately, these clinics are much too small, except for Amsterdam and Leiden. Since psychiatry departments pay little attention to sexual problems, a Society for Impotence Research (NVIO) was founded in 1986.
The work of Masters and Johnson opened the sexological territory for social scientists. Between 1975 and 1986, Utrecht trained psychology students in the practical applications of group and couple sex therapy. Since then, some psychologists and social workers in private practice provide treatment for couples with sexual problems. The sexological knowledge of helping professionals has certainly expanded in recent years. However, specialized sexological help is sometimes hard to find for many patients. The total number of sexologists is small and concentrated in certain areas. Health insurance will pay for sexological help if a physician refers. Clients almost always have to pay their own sliding-scale bills for treatment by psychologists and social workers in private practice and by Rutgers Foundation sexologists.
C. Therapist Training and Certification
Sexology is not a regulated profession in Holland, so full-time sexologists are rare and reliable sexologists and therapists will always have other basic training in medicine, psychology, psychiatry, or social work, perhaps with some postdoctoral education in sexology. Sexological education in Holland lacks cohesion and formal recognition. A very small number of professionals has been educated in the Flemish University of Leuven Sexology Department, where one can earn a doctorate in sexology.
Recently, the Dutch Society for Sexology (NVVS) started to regulate sexological training. Since 1992, an introductory course in sexology is provided by the NVVS and Erasmus University Rotterdam. Specialized curricula for medical-sexological workers, educators, prevention workers, and researchers will follow. An applications course for psychopathic rapists will be the next step in regulating sexological training. Recently, the Amsterdam Psychotherapy Training Institute included sexology in behavioral psychotherapy training. A register of trained members and establishment of set standards for the education of professional sexologists are short-term goals for NVVS.
A. Sexological Research
The Dutch Institute for Socio-Sexual Research (NISSO) has been the center of surveys on sexual behavior, sometimes in collaboration with other organizations. Considerable research has been done on contraception, abortion, sex and disabilities/illness, homosexuality in the armed forces, and prostitution. Other areas being explored are: the (in) adequacy of sexual help by different groups of helping professionals; an interview study on respondents of earlier surveys who reported exceptionally positive sex lives; child sexual development; forensic sexology; and construction of sexologically relevant psychometric scales.
The multidisciplinary nature of Dutch sexology is illustrated by the diverse backgrounds of the professors holding the six chairs dedicated to sexology in Dutch universities: endocrinology (Gooren, Amsterdam), psychiatry (Hengeveld, Utrecht), medicine (Van Dijk, Amsterdam), psychology (Frenken, Leiden), psychology (Cohen-Kettenis, Utrecht) and physiology/biology (Slob, Rotterdam).
The Psychology Department at Utrecht University has examined the therapeutic effect of different behavioristic treatment methods for sexual dysfunctions in individuals with different sexual orientations. The Utrecht University Gay and Lesbian Studies group has ongoing studies in: historical research on lesbian lives; various subjects on discrimination and homosexuality-related violence; homosexuality and education; and homosexuality in health care. The Amsterdam Psychology Department initiated Dutch psychophysiological research including the effects of sexual imagery on sexual arousal, women’s reactions to male- and female-made pornography, the effect of mood induction on subsequent visual stimulation, and the effect of subliminal visual stimuli. In Rotterdam, psychophysiological research includes study of the effects and interaction of visual and vibrotactile penile stimulation; the effect of papaverin-induced tumescence on perceptual threshold of penile stimulation in sexually functional and dysfunctional men, and the effect of menstrual phase on sexual arousability in women. In Groningen, research has included vaginal sensitivity in nonerotic conditions. Almost all academic urology departments are in some way active in research on erectile failure.
Animal sexology, centered in the Utrecht Department of Comparative Physiology, is an important aspect of Dutch sexology. Research at Utrecht and Rotterdam has focused on mating strategies in natural and semi-natural conditions: wolves, plains zebras, chimpanzees, orangutans and long-tailed macaques, savanna baboons, and stump-tailed macaques. The Rotterdam and Amsterdam groups have studied female initiative and hormonal influences on proceptivity and receptivity in rats, reward and aversive components in female sexual experience (including homosexual versus heterosexual preference conditions), hormone-dependency of self-stimulation behavior in the medial preoptic area; brain and behavior gender differentiation, and the determination of the different influences of various steroids. The sexually dimorphic nucleus of the preoptic area is also being researched.
B. Postgraduate and Advanced Programs
Treatment of human sexuality in medical, psychological, and social work curricula is subject to considerable variation, with the personal interest of faculty determining the impetus sexuality will have in the programs. Precise requirements and interdisciplinary training are defined in psychiatry and gynecology. There are no university sexology programs in other areas such as education, prevention, or research. In 1992, the Dutch Society for Sexology (NVVS) started a post-graduate training program (see Section 12C).
Journals
Tijdschrift voor Seksuologie (Journal of Sexology). Faculty of Medicine, Erasmus University, P. O. Box 1738, 3000 DR Rotterdam, The Netherlands
SOA Bulletin (Journal of STD). P. O. Box 19061, 3501 DB Utrecht, The Netherlands
Sekstant (Journal of the Dutch Society for Sexual Reform [NVSH]). P. O. Box 64, 2501 CB Den Haag, The Netherlands
Sexuality in Society. International newsletter of the NISSO. NISSO, da Costakade 45, 3521 VS Utrecht, The Netherlands
Organizations
A. de Graaf Foundation. (Prostitution), Westermarkt 4, 1016 DK Amsterdam
Interfacultaire Werkgroep Homostudies (Department of Gay and Lesbian Studies), Utrecht University, Heidelberglaan 1, 3584 CS Utrecht, The Netherlands
Dutch Centre for Health Promotion & Health Education, P. O. Box 5104, 3502 JC Utrecht, The Netherlands. Phone: 31-70/35-56847; Fax: 31-70/35-59901
Jhr A. Schorer Foundation. (Consultation bureau for homosexuality), Nieuwendijk 17, 1017 LZ Amsterdam, The Netherlands
NISSO (Netherlands Institute for Social Sexological Research), da Costakade 45, 3521 VS Utrecht, The Netherlands
NVIO (Dutch Society for Impotence Research), Department of Psychology, University of Amsterdam, Weesperplein 8, 1018 XA Amsterdam, The Netherlands
NVVS (Dutch Society for Sexology), Zijdeweg 17,2811 PC Reeuwijk, The Netherlands
Rutgers Foundation (Contraception information and sexuality education), Groothertoginnelaan 201, 2517 ES Den Haag, The Netherlands
Rutgers Stitching, Postbus 17430, Croot Hertoginnelaan 201, 2502 CKs Gravenhage, The Netherlands. Phone: 31-70/363-1750; Fax: 31-70/356-1049
Stimezo (National organization for induced abortion), Pieterstraat 11, 3512 JT Utrecht, The Netherlands
Note: The Special Issue of Tijdschrift voor Seksuologie issued for the Tenth World Congress for Sexology contains an exhaustive list of literature.
Beets, G., et al. 1991. Population and Family in the Low Countries 1991. Amsterdam/Lisse.
Brongersma, E. 1988, 1990. Loving Boys, 1 & 2. Elmhurst, New York, U.S.A.: Global Academic Publishers.
Cohen-Kettenis, P. T., & Th. G. M. Sandfort. 1991. “Sexual Behavior of Young Children: Observations of 665 Parents.” Paper presented at the Tenth World Congress for Sexology, 1991, Amsterdam.
Deenen, A. A. V. M. 1991. Intimacy and Sexuality in Gay Male Relationships. Dissertation,
Utrecht. Draijer, P.J. 1990. Seksuele Traumatisering in de Jeugd. Lange Termijn Gevolgen van Seksueel Misbruik van Meisjes Door Verwanten. Amsterdam: SUA.
Gianotten, W. L. 1988. “Sexology in the Netherlands: The Past and the Present.” Nordisk Sexologi, 6:202-09.
Glaser & Straus. 1980. Cited in C. Straver, Jong Zijn en Contact Zoeken (Being Young and Seeking Contacts). Zeist: Nisso.
Heslinga, K., A. Verkuil, & A. M. C. M. Schellen. 1973. Wij Zijn Niet van Stem, (Not Made of Stone: Sexuality of the Handicapped People). Leiden: Noordhoff stafleu.
Ketting, E. 1990. Contraception in Western Europe. Carnforth: Parthenon.
Ketting, E., & K. Soesbeek, eds. 1992. Homoseksualiteit en Krijgsmacht. Delft: Eburon.
Kooy, G. A. 1975. Seksualiteit, Huwelijk en Gezin in Nederland. Deventer: Van Loghum Slaterus.
Kooy, G. A. 1976. Jongeren en Seksualiteit. Deventer: Van Loghum Slaterus.
Kooy, G. A. 1983. Sex in Nederland. Utrecht/Antwerpen: Spectrum.
Kuiper, A. J. 1991. Transseksualiteit. Evaluatie van de Geslachtsaanpassende Behandeling. Utrecht: Elinkwijk.
Lamur, H., et al. 1990. Caraibische Vrouwen en Anticonceptie. Delft: Eburon.
Mooij, A. 1991. “De Ziektes van de Revolutie.” In G. Hekma, et al., eds. Het Verlies van de Onschuld. Groningen: Wolters-Noordhoff.
Nabrink, G. 1978. Seksuele Hervorming in Nederland. Nijmegen: SUN.
Noordhoff, J. D. et al. 1969. Sex in Nederland. Utrecht/Antwerpen: Spectrum.
Rademakers, J. 1992. Abortus in Nederland. 1989-1990. Utrecht: Stimezo.
Sandfort, Th. G. M. 1987. “Pedophilia and the Gay Movement.” Journal of Homosexuality, 13:89-111.
Sandfort, Th. G. M. 1991. “The Argument for Adult-Child Contact. A Critical Appraisal and New Data.” In O’Donohue & Geer, eds. The Sexual Abuse of Children: Theory, Research and Therapy. Hillsdale, New Jersey, U.S.A.: Lawrence Eribaum Associates.
Sandfort, Th. G. M., & G. van Zessen 1991. Seks en AIDS in Nederland, Den Haag: SDU.
Schraag, J. A. 1989. “Sexual Education in Schools: Concepts and Possibilities.” International Journal of Adolescent Medicine and Health, 3&4:239-250.
Schreurs, K. 1990. Vrouwen in Lesbische Relaties. Verbondenheid, Autonomie, en Seksualiteit. Utrecht: Publikatiereeks Homostudies.
Simon & Gagnon. 1980. Cited in C. Straver, Jong Zijn en Contact Zoeken (Being Young and Seeking Contacts). Zeist: Nisso.
Slijper. F. M. E. 1992. “Evaluation of Psychosexual Development of Young Women with Congenital Adrenal Hyperplasia: A Pilot Study.” Journal of Sex Education and Therapy, 18:200-07.
Straver et al. 1986. Stepwise Interaction Career: First elaborated in J. Rademakers and C. Straver, Van Fascinatie naar Relatie (From Fascination to Relation). Zeist: Nisso.
van Delft, M., & E. Ketting 1992. Anticonceptiege-Bruik in Nederland. Houten: Bohn Stafleu van Loghum.
van der Vliet, R. 1990. De Opkomst van het Seksuele Moratorium (The Rise of the Sexual Moratorium). In G. Hekma & B. van Stolk, eds., Het Verlies van de Onschuld (The Loss of Innocence). Groningen: Wolters-Noordhoff.
Verschoor, A. M. 1990. Een Dubbel Bestaan: Travestieten en Hun Omgeving. Amsterdam/Lisse: Swets en Zeitlinger.
Vogels, T, & R. van der Vliet. 1990. Jeugd en Seks. Den Haag: SDU.
![]()
![]()
![]()
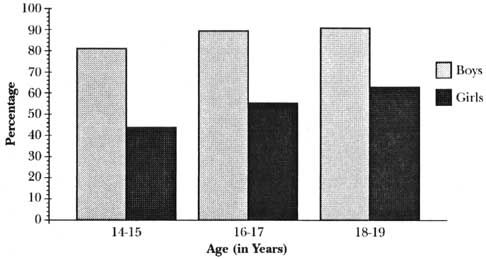{kind=link}
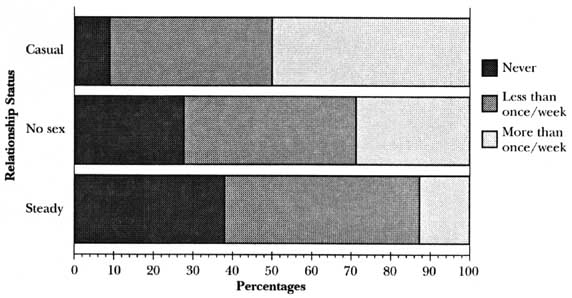{kind=link}
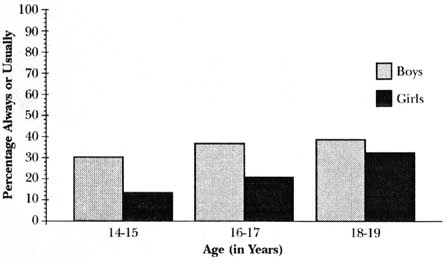{kind=link}
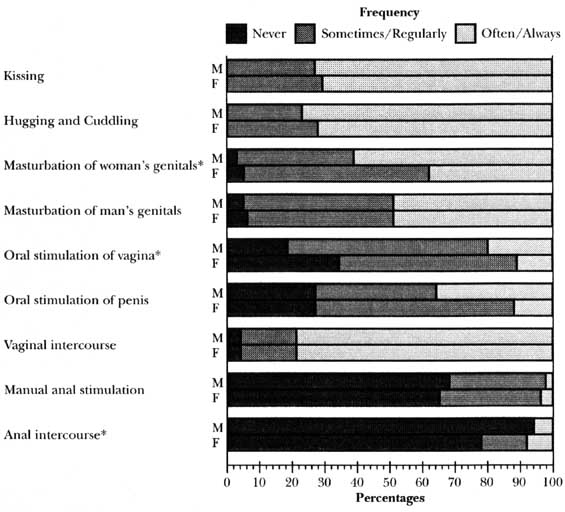{kind=link}