Transgender adults often report traumatic life experiences having been subjected to marginalization, discrimination and/or abuse over the course of their lives (Grant et al., 2010; Whittle, Turner, & Al-Alami, 2007). It is precisely these issues that have caused transgender adults great distress and have impacted their self-esteem and quality of life (Grant et al., 2010; Whittle et al., 2007). The impact of bullying, violence and shame on transgender individuals lives is well documented (Grant et al., 2010; Matos & Pinto-Gouveia, 2010; Nuttbrock et al., 2009; Whittle et al., 2007; Wyss, 2004) and has been shown to be a significant contributor to suicidal ideation (DiStefano, 2008; Roeger, Allison, Korossy-Horwood, Eckert, & Goldney, 2010). Moreover, a transgender adult identification has been shown to be correlated with cross-gender behaviour in childhood (Singh et al., 2010) and childhood gender role nonconformity as an indicator of adult suicidal ideation (Plöderl & Fartacek, 2009). Therefore understanding the childhood experiences of transgender adults within their families, social networks and environment would help contribute to the knowledge of how to support gender variant children and their parents with the aim of preventing the reported debilitating outcomes for transgender adults.
Gender variance is used to denote expressions of gender non-conforming dress and or behaviour. The term transgender is the umbrella term including the greatest diversity of people with gender variance (Bockting, 1999; Green, 1994; Lev, 2004). Transsexual, is a term used to describe people who seek medical intervention to change their primary and secondary sexual characteristics for the purposes of feeling congruent in mind and body and for social fit (Eyler, 2007, p. 16). Puberty-delaying hormone treatment, is a medical intervention using gonadotropin-releasing hormone (GnRH) analogues to prevent the appearance of the secondary sexual characteristics at puberty (Olsen, Forbes, & Belzer, 2011). This intervention suppresses the production of oestrogen or testosterone and is completely reversible (The Royal College of Psychiatrists Council Report CR63, 1998).
A number of needs analyses have been reported in the literature regarding transgender people's health, psychological, emotional and medical needs, though the focus has been on their needs as adults. The narrative studies by Costa and Matzner (2007) capturing life stories included some issues that were faced by transgender people as children. However, they lack the focus necessary for an analysis of the child's needs or associated needs of their parents.
To date, only one study has provided some insight to the needs of gender variant children and their parents, through a survey where parents of gender variant children were asked about their experiences and the needs of themselves and of their children (Riley, Clemenson, Sitharthan, & Diamond, 2011). The needs were reported in themes relating to: (a) identification of the gender variance, (b) parents responses and reactions, (c) seeking emotional support, (d) dealing with negative responses from others and concerns about safety, (e) seeking medical support and, (f) political, government and legislative support. The findings indicated that parents identified the needs of their gender variant children as the need to be accepted, loved and respected in their gender expression. The parents identified their own needs as the need for access to information, parenting strategies and emotional support. However, no previous studies have examined the needs of gender variant children from the perspective of adults who have lived through a gender variant childhood. These childhood experiences of transgender adults are an untapped source of crucial data in understanding and determining the needs of gender variant children.
The current investigation inquired about the childhood experiences of transgender adults helping to provide a further window into the difficulties and needs, met and unmet, for gender variant children and their parents. This study progressively investigates transgender adults understanding of their childhood with the aim of capturing their views on the needs of gender variant children and their parents as a step towards providing a safe and comfortable passage for them into adulthood.
Method
A qualitative study using an internet survey was designed to document the childhood experiences of transgender adults retrospectively, in order to ascertain their needs as children and what they perceived were their parent's needs. The study was approved by the Human Research Ethics Committee at the University of Sydney and was advertised through targeted magazines, websites, newspapers, radio programmes and through the World Professional Association for Transgender Health's (WPATH) Listserve and conference proceedings. Purposeful sampling (Charmaz, 2006; Patton, 2002) was employed using ten closed questions to gather demographic information and twenty-one open-ended questions to obtain a reflective expanded response, enabling an appreciation of the extent and depth of participants experiences (Huberman & Miles, 2002; Patton, 2002). As a unique and exploratory study, the questions were developed in consultation with professionals working with the transgender community, academics in the field and transgender adults. To reduce recall bias and improve the reliability of the retrospective method, the research design utilised chronological ordering of multiple open-ended questions to elicit memories of a personal nature and to aid memory retrieval (Brewin, Andrews, & Gotlib, 1993). The survey was open to any adult person who considered themselves transgender to confidently capture participants who experienced gender variant childhoods. The Participant Information Statement specified that participants could withdraw at any time and that submission of the survey is an indication of your consent to participate in the study. The survey was also designed to allow participants to skip questions they did not wish to answer further ensuring all responses were voluntary.
The open-ended questions covered transgender adults experiences of their gender variance as children and the reactions of their families. The survey specifically explored the impact that being gender variant had on their friendships, their experiences at school, and on them throughout their life. The questionnaire also examined services, resources or input that may have been helpful to them or their parents at the time and, in particular, their perspectives on what might help gender variant children and their parents today. Finally the survey considered the impact a gender variant childhood had and is having on each participant, with the last question inviting any further comments.
The qualitative data was analysed using a grounded theory (Charmaz, 2006) and reflective approaches (Grbich, 2009; Spradley, 1980) enabling content and thematic coding. The grounded theory approach bids the continuous reflection and comparison with the data to enable codes to emerge from the actions and processes within the participants experiences (Charmaz, 2006). The codes were checked by the research team and rechecked through examination with the original data to ensure consistency within the themes. Establishment of these themes then allowed the identification of patterns and categories of needs into tables. We included frequencies of codes in the tables to provide an understanding of how often comments were made, however, qualitative research is not dependant on the number of responses, which provides one perspective, but on information richness and depth attending to meaning (Patton, 2002; van Manen, 1997).
Results
Characteristics of participants
One hundred and eighty-one adults identifying with the term transgender adult entered the survey. Those participants who only answered the demographic data were excluded, as it was necessary to represent only the participants that provided input on the open-ended questions. This ensured that the determined needs of gender variant children and their parents were representative of those participants presented in the demographic table allowing 110 respondents to be included in these results. Table 1 presents the demographic information of the participants.
| Table 1: Demographics | ||||
| Born female n (%) |
Born male n (%) |
Born other n (%) |
All participants n (%) |
|
| Age Range | ||||
| 1825 | 8 (23) | 1 (<1) | 1 | 10 (9) |
| 2645 | 17 (49) | 21 (30) | 1 | 39 (35) |
| 4665 | 10 (29) | 44 (63) | 3 | 57 (52) |
| 66+ | 0 (0) | 4 (6) | 0 | 4 (4) |
| Total | 35 (101)* | 70 (100) | 5 | 110 (100) |
| Country | ||||
| Australia | 8 (23) | 21 (30) | 1 | 30 (27) |
| Canada | 1 (3) | 6 (9) | 1 | 8 (7) |
| France | 0 (0) | 2 (3) | 0 | 2 (2) |
| United Kingdom | 4 (11) | 3 (4) | 0 | 7 (6) |
| Japan | 0 (0) | 2 (3) | 0 | 2 (2) |
| Mexico | 0 (0) | 1 (1) | 0 | 1 (1) |
| Norway | 1 (3) | 0 (0) | 0 | 1 (1) |
| South Africa | 0 (0) | 2 (3) | 0 | 2 (2) |
| USA | 19 (54) | 28 (40) | 3 | 50 (45) |
| No reply | 2 (6) | 5 (7) | 0 | 7 (6) |
| 35 (100) | 70 (100) | 5 | 110 (99)* | |
| How do you describe yourself? | ||||
| Transgender | 5 (14) | 13 (19) | 0 | 18 (16) |
| Transsexual: female-to-male (FtM)1 | 20 (57) | 0 (0) | 1 | 21 (19) |
| Transsexual: male-to-female (MtF) | 0 (0) | 33 (47) | 1 | 34 (31) |
| Female | 3 (9) | 19 (27) | 3 | 25 (23) |
| Male | 3 (9) | 2 (3) | 0 | 5 (5) |
| Two-spirited | 1 (3) | 0 (0) | 0 | 1 (1) |
| Masculine androgyne/gender queer | 1 (3) | 0 (0) | 0 | 1 (1) |
| Androgyne | 1 (3) | 0 (0) | 0 | 1 (1) |
| Does not identify with a gender label | 1 (3) | 2 (3) | 0 | 3 (3) |
| No reply | 0 (0) | 1 (1) | 0 | 1 (1) |
| 35 (101)* | 70 (100) | 5 | 110 (101)* | |
| Gender Identity | ||||
| Female | 1 (3) | 54 (77) | 4 | 59 (54) |
| Male | 25 (71) | 2 (3) | 0 | 27 (25) |
| Androgynous | 4 (11) | 2 (3) | 1 | 7 (6) |
| Both female and male | 1 (3) | 12 (17) | 0 | 13 (12) |
| Neither female nor male | 4 (11) | 0 (0) | 0 | 4 (4) |
| 35 (99)* | 70 (100) | 5 | 110 (101)* | |
| Education | ||||
| High School or less | 6 (17) | 11 (16) | 1 | 18 (16) |
| Certificate | 0 (0) | 7 (10) | 0 | 7 (6) |
| Diploma | 1 (3) | 3 (4) | 1 | 5 (5) |
| Undergraduate Degree | 10 (29) | 18 (26) | 1 | 29 (26) |
| Postgraduate Degree | 18 (51) | 31 (44) | 2 | 51 (46) |
| 35 (100) | 70 (100) | 5 | 110 (99)* | |
| Gender variance identification: Age | ||||
| 05 | 18 (51) | 30 (43) | 5 | 53 (48) |
| 612 | 12 (34) | 37 (53) | 0 | 49 (44) |
| 1318 | 1 (3) | 1 (1) | 0 | 2 (2) |
| 18+ | 2 (6) | 0 (0) | 0 | 2 (2) |
| No reply | 2 (6) | 2 (3) | 0 | 4 (4) |
| 35 (100) | 70 (100) | 5 | 110 (100) | |
| Living as preferred gender | ||||
| Full-time | 27 (77) | 45 (64) | 5 | 78 (71) |
| Part-time | 6 (17) | 12 (17) | 0 | 18 (16) |
| Occasionally | 2 (6) | 8 (11) | 0 | 8 (7) |
| Never | 0 (0) | 4 (6) | 0 | 4 (4) |
| No reply | 0 (0) | 1 (1) | 0 | 1 (1) |
| 35 (100) | 70 (99)* | 5 | 110 (100) | |
| Are you taking hormones? | ||||
| Yes | 24 (69) | 54 (77) | 5 | 83 (75) |
| No | 11 (31) | 16 (23) | 0 | 27 (25) |
| 35 (100) | 70 (100) | 5 | 110 (100) | |
| If not, are you planning to take hormones in the future? | ||||
| Yes | 6 (55) | 8 (50) | 0 | 14 (52) |
| No | 5 (45) | 8 (50) | 0 | 13 (48) |
| 11 (100) | 16 (100) | 0 | 27 (100) | |
| Have you had gender reassignment surgery? | ||||
| Yes | 20 (57) | 33 (47) | 3 | 55 (50) |
| No | 15 (43) | 37 (53) | 0 | 53 (48) |
| No reply | 0 (0) | 0 (0) | 2 | 2 (2) |
| 35 (100) | 70 (100) | 5 | 110 (100) | |
| 1 One person in this category also identified as intersex and transgender as well as FtM | ||||
| * Numbers do not add up to 100 due to rounding errors. | ||||
| a Transsexual: Female-to-Males are also sometimes referred to as Transmen | ||||
| b Transsexual: Male-to-Females are also sometimes referred to as Transwomen | ||||
| Note: A proportion of participants, though placing themselves within the parameters offered, made note of their reluctance to be referred to in these terms. | ||||
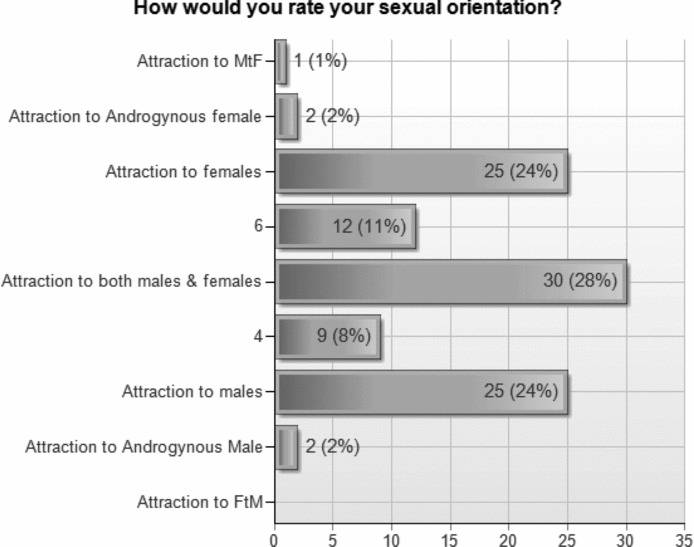
Sexual orientation was recorded (n = 106) covering the spectrum including being attracted to a male-to-female transsexual person (MtF) to being attracted to a female-to-male transsexual person (FtM) in order to give participants the opportunity to identify within a wide range of sexual orientations. The range specifically included: attraction to MtFs, attraction to females (gynephilic), attraction to both males and females (bisexual), attraction to males (androphilic), and attraction to FtMs. The option for participants to identify as being attracted to both males and females, with a tendency towards one or the other was provided to allow participants to identify across the spectrum. Twenty-one participants (19%) identified a sexual attraction in these two areas. Figure 1 illustrates the broad range of responses.
Figure 1. Display graph (n = 106) of sexual orientation (attractions) frequencies for each category. Note. MtF = male to female transsexual; FtM = female to male transsexual
Needs of gender variant children
The following describes the main themes that arose as needs in participant's responses to the open-ended questions What do you think would have helped you as a child then? and What do you think would help gender variant children today? The themes are presented in the order of the frequency (n) with which they were identified from 347 instances of suggested needs for gender variant children. The themes and frequencies are listed in Table 2.
| Table 2: Gender variant children's needs in order of the frequency with which they were reported | ||
| Needs of gender variant children | Frequency | |
| n | (%) | |
| 1. For education programs and information about gender variance to be implemented in schools and in society generally. | 55 | (16) |
| 2. For parents to love and value the child and provide space for them to talk about their feelings. | 52 | (15) |
| 3. To be allowed to express and display their felt gender. | 41 | (12) |
| 4. To know that others also have similar feelings and that gender variance is a natural occurrence. | 28 | (8) |
| 5. To have their gender issues recognised and to be offered help by professionals. | 28 | (8) |
| 6. For parents to transcend their cultural heritage, familial influences and religion to develop acceptance of gender variance in their children. | 26 | (7) |
| 7. To live in a society tolerant of diversity and accepting of gender variance. | 22 | (6) |
| 8. To be supported and understood by the school community. | 21 | (6) |
| 9. For puberty-delaying hormones to be made available where appropriate. | 19 | (5) |
| 10. To be aware of, and have access to, transgender role models. | 15 | (4) |
| 11. For schools to support gender diversity by eliminating gender stereotyping. | 15 | (4) |
| 12. To be protectednot bullied, harassed, blamed, shamed or attacked. | 13 | (4) |
| 13. To meet other similar children. | 5 | (1) |
| 14. Other needs. | 8 | (2) |
| 348 | (100)* | |
| * Numbers do not add up to 100 due to rounding errors. | ||
For education programs and information about gender variance to be implemented in schools and in society generally.
Education and up-to-date information including research was viewed as a bedrock in creating a knowledgeable and skilled environment within which to launch programs across the relevant sectors, including parenting and general education programs. This view was based on the overwhelming belief that the much needed education and information was lacking and would or could have made a difference to their parents responses. Of particular note was the emphasis placed on education in schools, with the need for knowledgeable school counsellors, educated teachers, programs for all children to be aware of, and supportive of, gender diversity. One participant noted that gender variant children need as much information as they can get that is tuned to their age and maturity level so that they can better understand who they are and what might help them to become more comfortable.
A number of participants felt that knowledge was necessary in order to set the foundation for acceptance of gender variance in children. They stated that there is not enough information explaining that, gender is not a sexual thing, and that gender is not sex and is not a binary phenomenon which they felt would help break down some of the walls for many parents. This lack of knowledge was noted as a key barrier to their parents supporting them, particularly as some participants expressed that their parents did not know that transgender people existed.
For parents to love and value the child and provide space for them to talk about their feelings.
The second most common need was the need for parents to provide an unconditional loving environment, with openness and sensitivity where the child could speak to them about their feelings and ask questions.
Participants wrote: I was really terrified of what my parents would think of me; I wanted the world to know, but I didn't have a safe world to tell or show, so I bottled myself up not just my gender either, but my whole self and; [I was] very scared - I had never heard of anyone else having such feelings. I thought if I told anyone they might put me away in some mental institution. I dared not even tell my parents.
Others wrote of situations where the potential for a conversation was thwarted by the parents. One participant wrote:
I found a pic in a catalogue. I felt that it would be really good to be able to dress and look like that. I took the catalogue to my mum, showed it to her, and asked her if I could have it. She said I couldn't because I was a boy and this was for girls. I buried the idea very quickly and did my best to not let anyone else know what my thoughts and feelings were.
While another participant explained:
I learned how to hide this part of me and became very good at it. I was never caught until one day during college, while living at home, I thought my parents had left the house but my dad came back in for something. He saw me with painted toenails and my legs shaved as I ran into the bathroom. He pretended he didn't see it and we never spoke about it.
One participant expressed their need for unconditional acceptance as: [Even though] Id have been killed quite literally, if I transitioned where I grew up, either way, feeling loved and valued, no matter what, by those who cared for me is what would have helped me the most.
Fifty per cent (n = 55) of participants never attempted to share their feelings as children with their parents, while a proportion accepted unspoken limitations. For example, one participant wrote: I never told my parents that I wished to be a boy. They allowed me to be a tomboy, and that was all I thought I could hope for.
Other examples demonstrated unexpected and negative responses received from families when an attempt to communicate was made. For example, I promptly came out to the family [and] received a forceful message that what I was doing was wrong or As a teen I told my mum I was gay and was forced to leave home. Another participant wrote movingly about how she was treated:
I tried to talk with my mother about my problem but it was too difficult for her. I was sent to a private all-boys school. As if that would cure me [It was] the only time I have endured beatings I was definitely not cross-dressing at school. Somehow people just knew I will never get over that.
These expressed fears provide an indication of the depth of suffering children tolerated even in circumstances where there was no deliberate expression or disclosure of their gender variance.
To be allowed to express and display their felt gender.
Many participants indicated that the lives of gender variant children would be much easier if they were supported to express themselves as they naturally felt. One participant stated that children need to be left to be who they are and supported rather than [being] forced into a role that scars them for life. Having to live up to stereotypes and being forced to live within the gender binary were phrases used in describing the causes of distress for gender variant children. Others stated that children ought to be allowed to properly explore their gender identities without fear of reprisals, and express their true self [in order] to avoid a life of suffering. One participant explained how they experienced life day to day:
Basically I felt like my life was pretty much an act in which I walked around in a vehicle that wasn't quite right, whereby no-one could really see me or know me and I couldn't be authentic. I was depressed, anxious, desperate, alienated, but managed to act nearly all the time as if everything was fine.
To know that others also have similar feelings and that gender variance is a natural occurrence.
A recurring theme was the sense of aloneness and isolation that being gender variant created. The need to know that I wasn't alone, that I wasn't crazy, that I was normal was how one respondent put it. Another participant wrote I was very miserable and thought I was going mad while others explained If I had even known trans people existed, that would have given me some language to articulate what I was feeling and made me feel less of a freak and the knowledge that I wasn't insane and that there was a reason for what I was thinking and feeling would have helped as a child. Others mentioned that children need to know [that] everyone is different and understand that it is not a crime to be yourself and that gender variance is a normal part of society. The lack of knowledge for some participants had a significant effect on how they appraised themselves. One participant wrote by the time I was 11, Id come to the conclusion that there was just something innately wrong with me, like I was some kind of cosmic joke, and I already had depression, low self-esteem, and suicidal tendencies while others explained I was always afraid to get close to people, and thought they would hate me or kill if they knew I was a freak and as a child I thought transsexuals were freaks, like a good portion of the population. I didn't know it was a real thing, so to speak.
To have their gender issues recognised and to be offered help by professionals.
There was general agreement that doctors, psychologists, psychiatrists, counsellors and other professionals need to be able recognise gender variance, transsexualism and transgenderism and be capable of diagnosis, recommendations and referrals for treatment or support. Some respondents mentioned that there ought to be early intervention and access to medical professionals who specialize in gender issues while another wrote that medicos and psychiatrists [need to] review the literature, listen to more intersex, transex people and parents to help facilitate what the child truly wants and needs without pressure.
A few respondents were taken to professionals regarding their gender variance. One participant wrote that the medical profession was very intolerant of gender diversity/variance and did not have knowledge or understanding of the gender variant person I was told by a Psych when I was 16yrs that I should GET OVER IT. Other participants wrote of their experience [I was] forced to go to a therapist who was determined to make a man out of me and [I was] ferried from one specialist to another who were examining me for some physical manifestation of this condition.
Respondents reported that they continued to experience this lack of understanding into adulthood. As one participant wrote most medical professionals I have spoken to about the subject have no idea at all, and tend to want to use you as a study subject, rather than offer professional help.
For parents to transcend their cultural heritage, familial influences and religion to develop acceptance of gender variance in their children.
Some participants noted that their parents, they felt, were unable to be open-minded enough to accept a transgender child, due to their culture or beliefs. In particular one participant wrote: my folks were brought up with the closed mentality of gays go to hell, and that boys cannot be girls and vice versa. Nothing can and will ever change their beliefs and another stated: Those were different times. The culture was virulently, monolithically homophobic, not to speak of trans-phobic, and they were a product of it. Others mentioned old-fashioned , bigoted or close-minded with a number stating that their parents would have never understood my gender identity issue or still will not speak to me. Religion was also mentioned as a barrier to parents willingness to accept the gender diversity in their children. Some participants expressed that religion in particular imposed a strict Binary view of life and that kids [ought to be able to] talk to their parents without fear of retribution or religious prosecution and that children have a right to know that gender isn't a religious moral imperative.
To live in a society tolerant of diversity and accepting of gender variance.
Some participants felt that if people were just more tolerant of difference and society would stop denying that transsexualism exists that their childhood would have been significantly easier to manage as everyone else being hung up about my gender made me worse. This lack of societal tolerance, open awareness of transgender issues in communities and general acceptance from society of gender variance was seen as a substantial impediment to their sense of well-being. Other participants wrote:
[I needed] more support and welcoming attitudes from people other than my immediate family. I feel blessed to have them so accepting, but family is not everything that makes a person. I wished I could have had more acceptance in the wider social world.
And,
It [gender variance] was a constant source of frustration [I became] increasingly conflicted I feel my life has been denied me. I never realised my full potential because so much of my energies were channeled into dealing with what was then an impossible situation.
To be supported and understood by the school community.
School in this context was referred to as the school community of other children, parents and staff as well as teachers or school counsellors. Participants felt that, not only was it important to be able to talk about their situation with their parents, but that they also needed recognition and support from school. One participant noted: it would have helped if the school authorities recognized my rebellion for what it wastrying not to conform to the expected gender identity role just because I had a female body.
For puberty-delaying hormones to be made available where appropriate.
None of the participants had access to puberty-delaying hormones as adolescents, but there was a variety of suggestions for puberty-delaying hormones to be available now for children. One participant felt that access to medical transition should be available to youth who are ready it can sure make life much easier!! Another stated that:
Blockers [puberty-delaying hormones] should be made available for our children to grant them the time they need to determine whether this is the right course for them. I felt my chance of another life was slipping away with every month that I was experiencing puberty.
One participant explained the difficulty they had with puberty:
I was late reaching puberty but when I did it was the worst thing ever. I didn't tell anyone Id started menstruating so each month was going through torment trying to cope with bleeding without any sanitary towels (I couldn't bring myself to buy any). I detested my body and became more and more isolated and withdrawn.
To be aware of, and have access to, transgender role models.
Apart from role models being visible in the media or society generally, a couple of participants noted that children ought to be aware of the wider variety of gender expressions and histories and of gender variance in cultures. One participant felt that visible transgender role models would ensure children see a future for themselves. One participant wrote that children might benefit from seeing more publicity of the many successful gender variant people living and working with a fulfilling life with less sensationalism in the media. One participant specified the type of connections they felt would be most useful with transgender adults, stating that:
If parents isolate themselves from decent trans-adults their child will ask themselves if theyll still be loved as an adult Meet with post everything trans-adults, help and be helped, but most importantly, be a REAL community. Don't just talk trans issues together, have them for dinner, play board games, watch movies, go out together in normal friend relationships and let the kids see some of that!
The few participants who wrote about their experiences of, or exposure to, other transgender individuals reported positive reinforcement of their self-identity. They wrote: I remember seeing a trans woman on TV when I was 45 years old, and thinking oh cool just like me and When I was about 18 I met a cross dresser perhaps a transsexual for the first time. It was a wondrous experience. I had a name for what I was and I was not alone.
For schools to support gender diversity by eliminating gender stereotyping.
Participants expressed a general dissatisfaction regarding how children are forced into female or male roles at school. One participant felt that schools produce differences that limit children's activities in expression, clothing, speech, friendships and desires, etc Gender is oppressive for EVERYONE! Another stated that society [needs to] understand that gender is a continuum and not binary and that everyone has some male and some female in them, physically and mentally. One participant felt that the binary sexual identity imposed by force at birth is the CAUSE of a trans-identity and ignores the fact that gender (brain sex) is the key element [of gender identity].
To be protected - not bullied, harassed, blamed, shamed or attacked.
Many participants described being ridiculed, teased, bullied or attacked in some way and the overriding impact that has on their self-esteem and confidence. The fear of not being safe infiltrated their daily life in ways that prevented them from doing activities they would have chosen. One participant explained how paralysing the circumstances were; I found myself with nothing I could do, not allowed to do what I wanted and just petrified of doing what others wanted me to do. This need to express one's self without fear was a major theme and was conveyed by another participant as:
The constant fear of being beaten was difficult to live with, but by high school I discovered how I could make myself feel better: I could become the person everyone expected me to be - and I was soon playing a sport (water polo) and learning how to be a man. This was, of course, when I was around other people. When I was alone, my gender issues would often overwhelm me.
One participant shared how the past still affects her today: The prejudices and fears are still with me and I am afraid to transition because I believe it will destroy my career and I will be ostracized by society.
To meet other similar children.
This was expressed in conjunction with knowing there were others with similar feelings. Participants conveyed that being able to meet other transgender children would have helped reduce the feeling of isolation and that the internet was now a way for trans-children to network with each other.
Other needs identified were: For parents to receive support (n = 4), for parents to become advocates for their gender variant children (n = 3) and for parents to be more involved with their children (n = 1).
Needs of parents of gender variant children
The following describes the needs identified for parents in response to the questions What do you think would have helped your parents/family? and What do you think would help gender variant parents today? The themes are presented in the order of the frequency (n) with which they were mentioned from 203 instances of suggested needs for parents of gender variant children. The themes and frequencies are listed in Table 3.
| Table 3: Needs of parents of gender variant children listed in order of frequency | ||
| Needs of parents of gender variant children | Frequency | |
| n | (%) | |
| 1. To have access to information. | 72 | (35) |
| 2. For schools, other parents and people generally to be educated and have awareness and knowledge about gender variance. | 49 | (24) |
| 3. To have access to other parents of gender variant children. | 22 | (11) |
| 4. For medical professionals and therapists to be educated about gender variance. | 18 | (9) |
| 5. For society to be open-minded and accepting of gender diversity. | 13 | (6) |
| 6. To see portrayals of successful transgender people. | 12 | (6) |
| 7. To have counselling. | 10 | (5) |
| 8. Other needs. | 7 | (3) |
| 203 | (100)* | |
| * Numbers do not add up to 100 due to rounding errors. | ||
To have access to information.
Many respondents mentioned the need for information or knowledge. This was further explained to be not just online but also in doctor's waiting rooms, on television, in schools, in libraries and on radio.
For schools, other parents and people generally to be educated and have awareness and knowledge about gender variance.
Participants emphasised that education was important for communities, parents and in schools, particularly for staff and parent-teacher organizations. Education of the general public was also mentioned as a way of increasing tolerance of gender diversity that would make it easier for parents to support their child and not worry what the neighbours might think.
To have access to other parents of gender variant children.
Having contact with other parents via the internet or through support groups was mentioned as a necessity for parents to feel less isolated. Other benefits of support groups were for parents to have a network and to encounter [others] with the same behaviour in their children.
For medical professionals and therapists to be educated about gender variance.
Some participants felt that knowledgeable professionals may have helped me/us address the underlying issues or that their parents needed the opportunity to discuss it [child's behaviour] with someone that understood [their situation].
One participant wrote:
GPs [need] to have training in the condition so they could inform parents, then my mum wouldn't have just waited for my gender difference to pass. People wouldn't have tried to push me to be a girl if they knew it was a medical condition.
For society to be open-minded and accepting of gender diversity.
Suggested was the need for parents to live in a supportive culture and society. Some participants felt that broader social acceptance including greater tolerant attitudes, without forced stereotypes would have helped their parents ability to support them.
To see portrayals of successful transgender people.
It was noted that, for parents to support their child with confidence, they needed to know about transgender people who were accomplished in employment, relationships and life in general. This was also mentioned with a view to inform parents that this [gender variance] is a part of the normal variety of life and that a child with gender reassignment can achieve virtually anything he/she wants.
To have counselling.
Counselling was mentioned specifically as a support for parents to aid them in collaborating with, and advocating for, their child's self-expression.
Other needs identified for parents.
Other items mentioned as needs for parents were; for them to have active support from religious communities (n = 3), for medical insurance to help with expenses (n = 1), for time to mourn (n = 1), to hear therapists and professionals speak publicly about gender variant children's needs (n = 1), and for legal protection (n = 1).
Discussion
This study was unique in that it explored adult transgender individual's experiences of their childhood with the view to determine the needs of children with gender variance and the needs of their parents.
Overwhelmingly, our participants expressed that they wanted parents, families, schools and communities to have more knowledge and awareness about gender, sex and issues regarding gender variance. This expressed deficit not only appeared to factor into the negativity and hostility the participants faced on an ongoing basis but also appeared to hinder their family's ability for acceptance of gender variance. Participants further expressed their feelings of fear and anxiety as they were unable as children to risk the rejection of those who cared for them. Some participants who felt supported and valued as gender variant children by their parents reported that this acceptance did not compensate for the ongoing fear of bullying and societal pressure to conform. Consequently, living in an environment of rigid stereotypes caused some participants to feel disoriented and at times crazy as they craved acknowledgement and recognition of their reality. The few participants who conveyed that their experience of being able to identify, name or recognise their feelings within a larger context, found that this bestowed on them an externally validated identity that provided a realness. This need for recognition, validation and acceptance supports the development of health literacy (Nutbeam, 2008) regarding gender variance across the identified sectors. Health literacy in this context would include the promotion of gender variance awareness through distribution of knowledge and education to medical providers, allied health practitioners, media, schools, consumers and society at large (Ishikawa & Kiuchi, 2010). Application of health literacy in this way would allow greater autonomy and empowerment (Nutbeam, 2008) for the individuals and families affected by gender variance and would increase their confidence in their needs being met.
The high level of education, 84% (n = 92) being at a tertiary level or higher, was an outstanding aspect of this cohort. If we exclude the age groups 1825 and 66+, we can compare the rate of tertiary levels of education from our study with the Organization for Economic Cooperation and Development (OECD, 2010) figures. The levels of tertiary education in our group of 2665 year olds was 87.5%, still way above the average level of tertiary education for 2564 year olds in OECD countries which is 30% (OECD, 2010) and the levels for Australia, 34% and the United States, 40%. Other studies of transgender communities have also found elevated levels of education (Clements-Nolle, Marx, & Katz, 2006; Shipherd, Green, & Abramovitz, 2010; Whittle et al., 2007). However, Xavier, Bobbin, Singer and Budd (2005) found the tertiary level of education for transgender people of colour to be 36%.
The sexual preference options chosen by the participants shown in Figure 1 are an indication that sexual attractions cover a much wider spectrum than previously thought. We have shown that given the options, transgender adults easily populate the grey areas between bisexuality and either attraction to females or attraction to males. Devor (1993) showed that FtM transsexual's sexual preferences may vary from the time before they transitioned to the time after they transitioned, and that there appeared to be inconsistencies in attractions as individuals tried various sexual partners possibly as a way of coming to their own sexual understanding of themselves. Devor also provided a distinction between being attracted to a straight or gay male or a straight or lesbian female, though this implies that one would need to know the sexual preference of the person they are attracted to before being able to identify their own sexual orientation. Grant et al. (2010) showed that separate categories of queer/pansexual and asexual and other provided 29% of sexual orientations in a survey of over 7,000 transgender and gender non-conforming people. Kenagy and Bostwick (2005) also found 33% of transgender people in their study (n = 111) identified with a sexual orientation other than heterosexual, bisexual or homosexual. What is clear is that options of sexual attraction to female, male or both is limiting and does not provide for variability in attractions allowing for a flexible sexual disposition (Diamond, 1965, p. 167). More research is required for a greater understanding of transgender people's sexual preferences. This study aims to be supportive of all gender variant children irrespective of their psychosocial outcome.
The needs were also analysed with respect to the birth sex of the participants. Although, perhaps remarkably, there was no difference in the resulting needs of the two groups (there were five participants who identified as other, therefore this group was not assessed), there were slightly different emphases placed on some needs. For example, the transgender adults, born female, accentuated their level of confusion as children, especially regarding how they were unable to understand why people did not see them as they saw themselves which transpired as part of the need for information and to be able to discuss their situation with caring adults. The transgender adults, born male, stressed a level of fear about how they would be treated if people knew about their feelings which became part of the need to be accepted, loved and supported. However, both groups mentioned both these factors and the resulting list of needs were the same.
Although other works have identified some similar needs for gender variant children, this research has quantified these needs. For example, Brill and Pepper's (2008) book The Transgender Child focussed on trans-positive approaches to gender variant children and stressed the need for unconditional acceptance and flexibility regarding children's identity and expression. They also warned against punishment of the child and other damaging parenting practices (p. 76) and provided recommendations about information and meeting other families.
The need for safety for gender variant children was also discussed by Blackburn (2004) and Wyss (2004) who showed the impact that harassment, bullying and gender-related abuse in a school environment had on transgender youth and mental health. They promoted strategies that directly responded to the needs outlined in these findings relating to education and information in schools for all children, teachers and staff, and insisted on policies that prohibited discrimination, violence or harassment against any person based on their sexual orientation (Blackburn, 2004) and gender identity or expression (Wyss, 2004).
One parent survey by Riley et al., (2011) showed that parents also identified some of the needs for gender variant children presented here, particularly in the areas of parents attitudes encompassing acceptance, support and advocacy. Riley et al.'s study indicates that both gender variant children and their parents needs changed over time as familiarity and acceptance grew. The children's needs initially focussed around the need to talk about their feelings and being allowed to express their gender. These needs then progressed to the needs for ongoing parental support and acceptance, protection and support from school, support from professionals and the need to have contact with similar others. The parents needs identified in Anonymous study centred around the access to information, parenting strategies and professional and community support. Community support included support from extended family, local community, school community, other families with gender variant children and society at large.
Limitations
The study's target audience were transgender adults enabling responses from those who were most likely to have experienced gender variant childhoods. Although there is evidence that homosexual adults also experience gender variance as children (Zucker & Bradley, 1995), it has been shown that not all homosexual people are gender non-conforming as children and that gender non-conforming behaviour increases with age for this group of people (Reiger et al. 2008). Future investigation of the needs of children who had a homosexual outcome is warranted. Furthermore, transgender adults are not a homogeneous population (Hines, 2010; Nash, 2010), further evidenced by the self-descriptions (and caveats) shown in Table 1 highlighting the diversity within this cohort.
The demographics (Table 1) show that 49% of respondents were in the age bracket 4665 indicating that the information required for memory recall was over 40 years old. Although we aimed to assist this recall in the design of the survey, it is important to remember that the retrospective method may still incur recall bias with participants current beliefs and understandings impacting their responses (Yarrow, Campbell, & Burton, 1970). Furthermore, this bias may affect the results as 53% of participants were older than 46. It is also acknowledged that the different age cohorts may represent different needs in childhood. Our analysis of this breakdown of needs generated a matrix with no remarkable skewing with zero or low numbers in each cell. In particular, the low number (n = 10) of 1825 year olds further reduced the suitability of this analysis.
The participants emphasis on the need for education and although currently relevant, needs to be placed in the context of the times. The ease of access to information via the internet and other popular media, including the current vast array of TV channels and movies, were not available to at least 90% of respondents as children.
Although this study gathered international respondents, it is acknowledged that being only in English severely limited global input and consequently, the greatest participation (86%) came from USA, Australia, Great Britain and Canada and therefore must be viewed through this lens. Demographic questions not answered included Country (6%) and Age at identification of gender variance (7%). Participants reticence to disclose their country may be to either preserve anonymity or that, perhaps, their country of childhood differed from their current country of residence. It is likely that the missing replies to Age at identification of gender variance were because they were unable to remember these details. We acknowledge that transgender people's needs are not homogenous and that variations in the needs of gender variant children likely exist across cultures. Further research would be required to determine the diversity of the needs of gender variant children across cultures and countries.
Some of these needs of gender variant children appear to be representative of the needs of children with varying conditions and may therefore be used to initiate investigations for these children.
Conclusion
The aims of this study were to identify the needs of gender variant children and their parents via information from transgender adults experiences and views of their childhoods.
This study has explored the experiences of childhood among transgender adults. In doing so, the needs of children that emerged were most notably, for parents, school staff and other authority figures to be educated so that children do not need to hide themselves and their gender expression for fear of adversity. The participants also expressed their need as children to be able to speak about their feelings, to have their gender expression accepted, to be recognised, to be protected, to be given the opportunity to know others with similar feelings and for their parents to be open-minded, able and willing to accept their gender variant children. We identified that the participants parents primarily needed access to information and educated professionals, particularly in schools, counselling and medical contexts. Exposure to successful transgender people and access to parent support groups was also seen as a need to help parents become more accepting of their children's diversity. The need for family and wider support was mentioned as a need for both the gender variant children and the parents as some participants felt that even though support of their parents was necessary, it was not enough for them to live happily and safely within the broader society.
The need for health literacy was highlighted as tool to empower individuals, in this case, parents, to respond effectively in addressing the issues with regard to their gender variant children. In particular, allowing confidence to approach professionals for support with their own and their child's emotional, physical and social well-being.
More research is required in the areas of sexual attractions and preferences where the results imply that a larger spectrum of preferences is necessary to capture and understand this widening area of human sexuality.
The findings of this study highlight the impact that enforced silence, coupled with the inability to identify similar feelings in others, had on the participants self-esteem and confidence in their knowledge and understanding of themselves. In addition, it appears that living in a society where punishment is customary for lack of conformity to gender stereotypes creates a lifelong struggle and sometimes withdrawal that caused some participants great distress and impacts on their self-esteem and ability to thrive.
The needs of gender variant children and their parents identified in this study is important input to education programs that would contribute to the overall well-being of gender variant children and support for their parents. This information also has the potential to contribute to the development of trans-positive guidelines for both parents and the broader community. Wider input from professionals would also be helpful in creating a more comprehensive input into the needs of gender variant children and their parents.