Devita Singh
A
FOLLOW-UP STUDY OF BOYS
WITH GENDER IDENTITY DISORDER
A thesis submitted in conformity with the requirements
for the degree of Doctor of Philosophy
Department of Human Development and Applied Psychology
Ontario Institute for Studies in Education
University of Toronto
© Copyright by Devita
Singh (2012)
Reproduced here by permission of the author.
Devita Singh, Doctor of Philosophy
Department of Human Development and Applied Psychology
University of Toronto
Main Contents:
Abstract
This study provided information on the long term psychosexual and psychiatric outcomes of 139 boys with gender identity disorder (GID). Standardized assessment data in childhood (mean age, 7.49 years; range, 3–12 years) and at follow-up (mean age, 20.58 years; range, 13–39 years) were used to evaluate gender identity and sexual orientation outcome. At follow-up, 17 participants (12.2%) were judged to have persistent gender dysphoria. Regarding sexual orientation, 82 (63.6%) participants were classified as bisexual/ homosexual in fantasy and 51 (47.2%) participants were classified as bisexual/homosexual in behavior. The remaining participants were classified as either heterosexual or asexual. With gender identity and sexual orientation combined, the most common long-term outcome was desistence of GID with a bisexual/homosexual sexual orientation followed by desistence of GID with a heterosexual sexual orientation. The rates of persistent gender dysphoria and bisexual/homosexual sexual orientation were substantially higher than the base rates in the general male population. Childhood assessment data were used to identify within-group predictors of variation in gender identity and sexual orientation outcome. Social class and severity of cross-gender behavior in childhood were significant predictors of gender identity outcome. Severity of childhood cross-gender behavior was a significant predictor of sexual orientation at follow-up. Regarding psychiatric functioning, the heterosexual desisters reported significantly less behavioral and psychiatric difficulties compared to the bisexual/homosexual persisters and, to a lesser extent, the bisexual/homosexual desisters. Clinical and theoretical implications of these follow-up data are discussed.
Acknowledgements
There are a number of individuals who have contributed instrumentally in the various stages of the dissertation project and to whom I would like to express my most sincere gratitude.
First, to my supervisor, Dr. Ken Zucker, there are no words to express what your continued mentorship has meant to me. Thank you for graciously accepting me as a student seven years ago. Your impact in my life extends far beyond research and clinical training–you also helped me to develop as a person and I feel privileged to have worked with you. You have equally inspired, challenged, and, certainly, frustrated me. Looking back, however, it has been the most insightful and rewarding journey these past years. Your immense wisdom and insightfulness never ceased to amaze and inspire me, perhaps rivaled only by your astute attention to detail and editing skills. Thank you for allowing me to complete this fascinating project with you and for the endless hours discussing the meaning of it all. Perhaps most importantly, thank you for holding such high expectations of me. Your relentless ability to “push” me (and prevent me from “whining”) caused me endless grief, but alas helped to create this wonderful piece of work and fostered my growth in numerous ways.
I sincerely thank my thesis committee members for their invaluable contributions and insightful feedback that not only shaped this project in interesting ways, but also enhanced my learning. Dr. Michele Peterson-Badali, you have been instrumental in my Ph.D. research, first as the second reader for my M.A. thesis and now as a committee member for my dissertation. Your insight, feedback, and encouragement have been undoubtedly helpful, especially as I weathered seemingly insurmountable obstacles. Dr. Katreena Scott, I thank you for not only your intellectual commitment to this endeavor, but your ability to help me always remember to see the forest for the trees. I greatly appreciate your selflessness in always making time for me and your incredible capacity to problem solve. Dr. Susan Bradley, I am most grateful for your clinical insights. The commitment, empathy, and skills you bring to clinical work with children and their families have inspired me and provided me with skills which have enabled me to grow as a clinician. Dr. Lana Stermac, thank you for coming on board and offering your insights. Finally, to my external examiner, Dr. Michael Bailey, it was indeed my pleasure to have your insights and reflections on this project. Since I first read your book, I recognized your passion for understanding the lives of gender dysphoric children and was immensely pleased that you agreed to take on this role.
I express sincere gratitude and appreciation to the study participants, for without you this project could not come have come to fruition. Thank you for the hours spent sharing your stories–your candor made data collection enjoyable and added much depth and complexity to this project. Thank you to members of the Gender Identity Service who have been important supports and to the research assistants who tolerated my need for perfection as you entered the large volume of data needed for this project. I would also like to thank Dr. Ray Blanchard and Dr. James Cantor for your statistical support and clinical insights.
Finally, I think my family and friends. This arduous journey would not have been possible without your warmth, support, and patience with the inevitable stress associated with this project. To old and dear friends–Tomoko and Heidy–we have shared countless memories throughout the years and your support helped me complete this journey. Hamed, there are no words! You made so much possible and I am forever grateful for our friendship and for your kindness when I needed it most. Brian, thank you for being an amazing friend and the most patient person I have ever met. The many, many hours you spent listening to my venting and offering technical support made this journey substantially easier. Navin, your unconditional support has not gone unnoticed. To my parents, words cannot express the gratitude I have for unique ways in which you have both supported and encouraged me. Dad, thank you for always understanding and challenging me, and mom, thank you for inspiring me to be better than I think I am capable of. Finally, but by no means least, I sincerely thank my sister, Wanita. You get me in ways no one else can and made the most difficult phases of this project bearable.
Table of Contents
|
xiv |
|
|
xvi |
|
|
xvii |
|
|
1 |
|
|
1 |
|
|
3 |
|
|
1.2.1 Sex and Gender. |
3 |
|
1.2.2 Gender Role. |
4 |
1.2.3 Gender Identity.. |
4 |
|
1.2.4 Gender Dysphoria. |
5 |
|
1.2.5 Sexual Orientation. |
9 |
|
1.2.6 Sexual Identity. |
10 |
|
1.2.7 Transgender and Transsexualism. |
10 |
|
11 |
|
|
1.3.1 GID in Children. |
11 |
|
1.3.2 GID in Adolescents and Adults. |
14 |
|
15 |
|
|
16 |
|
|
1.5.1 The Therapeutic Model. |
16 |
|
1.5.2 Accommodation Model. |
18 |
|
1.5.3 Early Transition Approach. |
19 |
|
22 |
|
|
1.6.1 Diagnostic Reform. |
22 |
|
1.6.2 Is GID a Mental Disorder? . |
24 |
|
27 |
|
|
1.7.1 Gender Identity Outcome of Children with GID. |
27 |
|
1.7.1.1 Methodological Issues. |
31 |
|
1.7.1.2 Process of GID Desistence. |
31 |
|
1.7.2 Gender Identity Outcome of Adolescents with GID. |
34 |
|
1.7.3 Sexual Orientation Outcome. |
35 |
|
1.7.4 Gender Identity and Sexual Orientation Outcomes in Boys with GID: Summary. |
40 |
|
1.8 Retrospective Studies of Homosexual Men: Summary of Key Findings. |
41 |
|
1.9 Childhood Sex-Typed Behavior and Sexual Orientation: Explaining the Linkage. |
43 |
|
1.9.1 Biological Explanation: Influence of Genes. |
43 |
|
1.9.2 Biological Explanation: Role of Prenatal Hormones. |
46 |
|
1.9.3 Psychosocial Explanations. |
48 |
|
49 |
|
|
1.10.1 Children with GID. |
49 |
|
1.10.1.1 Behaviour Problems in Children with GID. |
49 |
|
1.10.1.2 Comorbidity in Children with GID. |
53 |
|
1.10.2 Adolescents and Adults with GID. |
55 |
|
1.10.3 Suicidality and Victimization in Transgendered Populations. |
58 |
|
60 |
|
|
1.11.1 Rationale for the Present Study. |
63 |
|
1.11.2 Goals of the Present Study. |
65 |
|
67 |
|
|
67 |
|
|
2.1.1 Routine Contact for Research. |
68 |
|
2.1.2 Participant-Initiated Clinical Contact. |
70 |
|
2.1.3 Participation Rate. |
71 |
|
2.1.4 Demographic Characteristics of Participants. |
71 |
|
71 |
|
|
73 |
|
|
2.3.1 Childhood Assessment. |
73 |
|
2.3.1.1 Cognitive Functioning. |
73 |
|
2.3.1.2 Sex-typed Behavior. |
73 |
|
2.3.1.3 Behavior Problems. |
75 |
|
2.3.1.4 Peer Relations. |
76 |
|
2.3.2 Follow-up Assessment. |
76 |
|
2.3.2.1 Cognitive Functioning. |
77 |
|
2.3.2.2 Behavioral Functioning. |
79 |
|
2.3.2.3 Psychiatric Functioning. |
80 |
|
2.3.2.4 Psychosexual Variables. |
82 |
|
2.3.2.4.1 Recalled Childhood Gender Identity and Gender Role Behaviors. |
82 |
|
2.3.2.4.2 Concurrent Gender Identity. |
83 |
|
2.3.2.4.3 Concurrent Gender Role–Parent Report. |
87 |
|
2.3.2.4.4 Sexual Orientation. |
87 |
|
2.3.2.4.4.1 Sexual Orientation in Fantasy. |
88 |
|
2.3.2.4.4.2 Sexual Orientation in Behavior. |
89 |
|
2.3.2.4.4.3 Sexual Orientation Group Classification. |
91 |
|
2.3.2.5 Social Desirability. |
92 |
|
2.3.2.6 Suicidality Experiences. |
93 |
|
2.3.2.7 Victimization Experiences. |
94 |
|
96 |
|
|
96 |
|
|
3.2 DSM Diagnosis for Gender Identity Disorder in Childhood. |
100 |
|
3.2.1 Childhood Behavior Problems as a Function of Diagnostic Status for Gender Identity Disorder. |
100 |
|
3.2.2 Childhood Sex-Typed Behavior as a Function of Diagnostic Status for Gender Identity Disorder. |
101 |
|
101 |
|
|
3.3.1 Gender Identity at Follow-up. |
101 |
|
3.3.1.1 Criteria for Persistence of Gender Dysphoria. |
103 |
|
3.3.1.2 Rate of Persistence and Desistence. |
104 |
|
3.3.1.3 Persistence of Gender Dysphoria as a Function of GID Diagnosis in Childhood. |
105 |
|
3.3.1.4 Summary of Gender Dysphoric Participants. |
105 |
|
3.3.1.5 Odds of Persistent Gender Dysphoria. |
107 |
|
3.3.2 Sexual Orientation at Follow-up. |
108 |
|
3.3.2.1 Group Classification as a Function of Gender Identity and Sexual Orientation in Fantasy at Follow-up. |
110 |
|
112 |
|
|
3.4.1 Demographic Characteristics in Childhood as a Function of Gender Identity and Sexual Orientation in Fantasy. |
112 |
|
3.4.2 Demographic Characteristics at Follow-up as a Function of Gender Identity and Sexual Orientation in Fantasy. |
117 |
|
118 |
|
|
118 |
|
|
3.6.1 Childhood Sex-Typed Behavior as a Function of Gender Identity and Sexual Orientation at Follow-up. |
118 |
|
3.6.2 Childhood Sex-Typed Behavior and Year of Assessment. |
125 |
|
125 |
|
|
3.8 Childhood Behavior Problems as a Function of Gender Identity and Sexual Orientation at Follow-up. |
126 |
|
128 |
|
|
3.9.1 Gender Dysphoria. |
128 |
|
3.9.1.1 “Caseness” of Gender Dysphoria on the Gender Identity Questionnaire for Adolescents and Adults. |
130 |
|
3.9.2 Recalled Childhood Sex-Typed Behavior. |
133 |
|
3.9.2.1 Recalled Childhood Sex-Typed Behavior as a Function of Group. |
135 |
|
3.9.2.2 Recalled Childhood Sex-Typed Behavior and Childhood-Sex-Typed Behavior. |
135 |
|
3.9.3 Sexual Orientation. |
136 |
|
3.9.3.1 Sexual Orientation in Fantasy. |
136 |
|
3.9.3.2 Sexual Orientation in Behavior. |
137 |
|
3.9.4 Parent Report of Concurrent Gender Role. |
139 |
|
140 |
|
|
3.10.1 Behavior Problems at Follow-up as a Function of Gender Identity and Sexual Orientation: Maternal-Report. |
140 |
|
3.10.2 Behavior Problems at Follow-up as a Function of Gender Identity and Sexual Orientation: Self-Report. |
142 |
|
144 |
|
|
3.11.1 Psychiatric Functioning at Follow-up as a Function of Gender Identity and Sexual Orientation. |
144 |
|
146 |
|
|
3.12.1 Suicidality Questionnaire. |
146 |
|
3.12.2 Suicidality on the Youth Self-Report (YSR)/Adult Self-Report (ASR). |
148 |
|
3.12.3 Parent-Report of Suicidality on the Child Behavioral Checklist (CBCL)/Adult Behavior Checklist (ABCL). |
152 |
|
152 |
|
|
3.13.1 Descriptive Victimization Experiences for the Entire Sample. |
153 |
|
3.13.2 Victimization Experiences as a Function of Sexual Orientation in Fantasy. |
155 |
|
3.13.3 Victimization and Mental Health. |
158 |
|
3.13.4 Victimization and Childhood Sex-Typed Behavior. |
158 |
|
3.13.5 Victimization and Parent-Report of Concurrent Gender Role Behavior. |
159 |
|
3.14 Comparisons with Other Follow-up Studies of boys with Gender Identity Disorder. |
159 |
|
3.14.1 Persistence Rates across Follow-up Studies of Boys with Gender Identity Disorder. |
159 |
|
3.14.2 Threshold vs. Sub-threshold for Gender Identity Disorder. |
160 |
|
162 |
|
|
162 |
|
|
164 |
|
|
166 |
|
|
168 |
|
|
4.4.1 Gender Identity Outcome. |
168 |
|
4.4.1.1 Rate of Persistent Gender Dysphoria. |
168 |
|
4.4.2 Sexual Orientation Outcome. |
169 |
|
4.4.2.1 Rate of Bisexual/homosexual Sexual Orientation. |
169 |
|
4.4.2.2 Sexual Orientation of Persisters. |
171 |
|
4.4.2.3 Age and Sexual Orientation. |
171 |
|
4.4.3 Multiple Long-term Psychosexual Outcomes for Boys with GID. |
173 |
|
173 |
|
|
4.5.1 Demographic Predictors of Gender Identity Outcome. |
174 |
|
4.5.1.1 Social Class. |
174 |
|
4.5.1.1.1 Familial Stress and Parental Psychopathology. |
175 |
|
4.5.1.1.2 Quality of Peer Relationships. |
176 |
|
4.5.1.1.3 Attitudes towards Homosexuality. |
177 |
|
4.5.2 Childhood Sex-Typed Behavior as a Predictor of Gender Identity Outcome. |
181 |
|
4.5.3 Behavior Problems in Childhood as a Predictor of Gender Identity Outcome. |
182 |
|
4.6 Variation in Persistence Rates across Follow-up Studies of Boys with GID. |
185 |
|
4.6.1 Sample Differences. |
186 |
|
4.6.2 Sociocultural Influences. |
190 |
|
4.6.3 Referred vs. Non-Referred Children. |
192 |
|
4.6.4 Treatment Experience. |
193 |
|
193 |
|
|
4.7.1 Theoretical Implications. |
193 |
|
4.7.2 Clinical Implications. |
195 |
|
4.7.2.1 Should Gender Transitioning be Encouraged in Childhood?. |
195 |
|
4.7.2.2 Effects of Treatment on Long-Term Gender Identity Outcome. |
198 |
|
4.7.3 Process of GID Desistence and Persistence Overtime. |
200 |
|
201 |
|
|
203 |
|
|
4.10 Behavioral Problems and Psychiatric Functioning at Follow-up. |
206 |
|
4.10.1 Behavior problems at follow-up. |
206 |
|
4.10.2 Psychiatric functioning at follow-up. |
208 |
|
4.10.2.1 Implications of Psychiatric Outcomes. |
209 |
|
4.10.2.1.1 Distress of Gender Dysphoria. |
209 |
|
4.10.2.1.2 Peer and Family Rejection. |
210 |
|
4.10.2.1.3 Minority Stress. |
211 |
|
4.10.2.1.4 Familial Psychiatric Vulnerability. |
214 |
|
215 |
|
|
4.12 Limitations of the Present Study and Future Directions. |
220 |
|
222 |
|
|
224 |
|
|
275 |
|
Table 1 |
Distribution of Recruitment Across Data Collection Period. |
68 |
|
Table 2 |
Demographic Characteristics of Participants. |
72 |
|
Table 3 |
Measures of Childhood Sex-Typed Behavior. |
74 |
|
Table 4 |
Follow-up Assessment Protocol. |
78 |
|
Table 5 |
Demographic Characteristics and Behavior Problems as a Function of Participant Status. |
97 |
|
Table 6 |
Childhood Sex-Typed Behavior as a Function of Participant Status. |
98 |
|
Table 7 |
Childhood Sex-Typed Behavior as a Function of Diagnostic Status for Gender Identity Disorder in Childhood. |
102 |
|
Table 8 |
Summary of Gender Dysphoric Participants. |
106 |
|
Table 9 |
Kinsey Ratings for Sexual Orientation in Fantasy. |
108 |
|
Table 10 |
Kinsey Ratings for Sexual Orientation in Behavior. |
109 |
|
Table 11 |
Demographic Characteristics in Childhood and at Follow-up as a Function of Group. |
113 |
|
Table 12 |
Correlation Matrix of Childhood Demographic Variables on which the Groups Differed. |
115 |
|
Table 13 |
Multinomial Logistic Regression Predicting Group Outcome at Follow-up from Demographic Variables. |
117 |
|
Table 14 |
Childhood Sex-Typed Behavior as a Function of Group. |
119 |
|
Table 15 |
Correlation Matrix of Childhood Sex-Typed Measures on which the Groups Differed. |
122 |
|
Table 16 |
Multinomial Logistic Regression Predicting Group Outcome at Follow-up from Demographic Variables and Sex-Typed Behavior. |
124 |
|
Table 17 |
Behavior Problems in Childhood and Follow-up as a Function of Group. |
127 |
|
Table 18 |
Psychosexual Measures as a Function of Group. |
129 |
|
Table 19 |
Mean Factor 1 Score on the Recalled Childhood Gender Identity/Gender Role Questionnaire. |
133 |
|
Table 20 |
Sexual Orientation in Fantasy and Behavior on EROS and SHQ. |
138 |
|
Table 21 |
Correlations between Behavior Problems in Childhood (CBCL) and Follow-up (YSR/ASR, CBCL/ABCL). |
141 |
|
Table 22 |
Number of Psychiatric Diagnoses at Follow-up. |
144 |
|
Table 23 |
Psychiatric Functioning at Follow-up as a Function of Group. |
146 |
|
Table 24 |
Suicidal Ideation and Behavior at Follow-up as a Function of Group. |
149 |
|
Table 25 |
Gender Identity-Related Victimization. |
154 |
|
Table 26 |
Mean Frequency of Victimization as a Function of Group. |
156 |
|
Figure 1 |
Distribution of social class for the outcome groups at follow-up. |
116 |
|
Figure 2 |
Distribution of the mean composite z-score for the outcome groups at follow-up. |
123 |
|
Figure 3 |
Distribution of the GIQAA mean score for the outcome groups. |
132 |
|
Appendix A |
DSM-IV-TR Diagnostic Criteria for Gender Identity Disorder. |
275 |
|
Appendix B |
Proposed DSM-5 Diagnostic Criteria for Gender Dysphoria in Children. |
277 |
|
Appendix C |
Phone Script. |
279 |
|
Appendix D |
Vignette: Parent Report on Gender Identity and Sexual Orientation |
281 |
|
Appendix E |
Participant-Initiated Research Contact: Reasons for Clinical Contact. |
283 |
|
Appendix F |
Research Consent Form. |
286 |
|
Appendix G |
Semi-Structured Interview to Assess Gender Identity Disorder in Biological Males. |
289 |
|
Appendix H |
Inter-rater Reliability for Kinsey Ratings of Sexual Fantasy and Sexual Behavior. |
292 |
|
Appendix I |
Suicidality Questionnaire. |
294 |
|
Appendix J |
Victimization Survey. |
297 |
|
Appendix K |
Gender Identity and Sexual Orientation at Follow-up. |
303 |
|
Appendix L |
Diagnostic Interview for Children and Adolescents or Diagnostic Interview Schedule Diagnoses at Follow-up. |
312 |
|
Appendix M |
Gender Identity and Sexual Orientation Outcomes in Follow-up Studies of Boys with GID. |
323 |
Chapter 1
Introduction
Gender identity is usually a central aspect of a person’s sense of self and, once developed, appears to be less malleable as development progresses (e.g., Egan & Perry, 2001; Ruble, Martin, & Berenbaum, 2006). The development of one’s gender identity and, by extension, gender role, is more than a cognitive milestone as it impacts on virtually all aspects of human functioning. In childhood, significant sex differences are seen in such behavioral domains as peer, toy, and activity preferences (e.g., Fagot, Leinbach, & Hagan, 1986; Ruble et al., 2006; Zucker, 2005b). In adolescence and adulthood, significant sex differences are seen in psychosocial domains such as interpersonal relational styles (e.g., Maccoby, 1998) and career choice (e.g., Lippa, 1998, 2005). One can imagine the profound implications on the person whose gender identity development departs from typical pathways and which results in much distress for the individual, a phenomenon that is recognized clinically as Gender Identity Disorder (GID).
Green and Money’s (1960) seminal article on boys with “incongruous gender role” was perhaps the first attempt in the literature to label, describe, and characterize the phenotype of young boys who exhibited a pattern of cross-gender behavior. Fourteen years later, Green’s (1974) seminal book, “Sexual Identity Conflict in Children and Adults,” provided a comprehensive description of children who were “discontent with the gender role expected of them.” Since the publication of these early works and, certainly, with the introduction of GID to the psychiatric nomenclature in the third edition of the Diagnostic and
Statistical Manual of Mental Disorders (DSM; American Psychiatric Association, 1980), tremendous progress has been made in understanding several aspects of this disorder. The phenomenology of GID is now fairly well documented (e.g., Cohen-Kettenis & Pfäfflin, 2003; Zucker, 2000, 2005a; Zucker & Bradley, 1995) and psychometrically robust assessment measures and procedures have been developed to allow for thorough diagnostic evaluation (for reviews, see Zucker, 1992, 2005b; Zucker & Bradley, 1995).
There are, however, some important gaps in the literature on children with GID, two of which are addressed in the current study. Although the natural history or outcome of boys with GID has received some empirical attention, the findings have not been consistent. Studies have generally found that not all boys with GID persist in having GID in adulthood and, in fact, the majority desist and have a homosexual sexual orientation. However, the rates of persistence of GID found across various studies have been variable, ranging from 2.3% to 30% (Green, 1987; Wallien & Cohen-Kettenis, 2008), but are considerably higher than the estimated prevalence of GID in the general population (Zucker & Lawrence, 2009). The reasons for this variability are a matter of conjecture as little is known about the factors that influence GID persistence into adolescence and adulthood. Further complicating the picture is the finding that some children with GID do grow up to have a heterosexual sexual orientation (e.g., Wallien & Cohen-Kettenis, 2008). Thus, given the variation observed in the long-term gender identity and sexual orientation outcome of boys with GID, it is important to examine childhood predictors of outcome in a sample of boys with atypical gender development. Second, very little is known about the long-term psychiatric outcome of boys with GID as the follow-up studies to date have primarily examined gender identity and sexual orientation outcomes.
The present study aimed to fill these gaps in the literature on boys with GID. First, the study examined the gender identity and sexual orientation outcome of boys with GID. Second, the study examined psychiatric outcome at follow-up. Third, using the extensive assessment data collected during childhood, in conjunction with the follow-up data, the study attempted to identify within-group childhood characteristics that were predictive of variations in gender identity and sexual orientation outcome in adolescence and adulthood.
This chapter will begin with a review of relevant psychosexual terminology. Information about the phenomenology of GID in children, adolescents and adulthood is summarized, including associated psychopathology in children, adolescents, and adults with GID. Current controversies in the field, particularly with regard to diagnosis and treatment, are summarized. This is followed by the results of studies that have examined gender identity and sexual orientation outcome in boys with GID. The literature on the relationship between childhood sex-typed behavior and sexual orientation in adulthood is reviewed. The remainder of the chapter includes a conceptual framework for the study within the field of developmental psychopathology. The chapter concludes with the rationale and goals for the present study. Given that the present study was a follow-up of boys with GID, the literature summarized in this chapter is primarily on that of boys with GID.
1.2.1 Sex and Gender
The terms sex and gender have been used interchangeably in the literature (Muehlenhard & Peterson, 2011). In this thesis, sex refers to whether a person is biologically male or female. Some of the common attributes that distinguish a person as male or female include the sex chromosomes, gonads, and internal and external genitalia (Vilain, 2000). Gender refers to psychological and behavioral characteristics associated with males and females (Kessler & McKenna, 1978; Ruble et al., 2006).
1.2.2 Gender Role
The term gender role, originally coined by Money (1955), refers to those behaviors, attitudes, and personality attributes that are consistent with cultural definitions and expectations of masculinity and femininity (Diamond, 2002; Zucker & Bradley, 1995). During childhood, gender role is commonly operationalized according to certain observable behaviors, referred to as sex-typed behaviors, including peer preference, interest in rough-and-tumble play, dress-up play, toy preference, and so on (Ruble et al., 2006). These gender role/sex-typed behaviors are often construed as indirect markers of a child’s gender identity as they are, on average, sex dimorphic (Zucker, 2005b). For example, boys tend to be more active than girls and engage more in rough-and-tumble play (Maccoby, 1998). Boys, on average, prefer to play with toy vehicles and weapons while girls, on average, prefer to play with dolls and toy household items (Berenbaum & Snyder, 1995). The diagnostic criteria for GID are defined, in part, by a profound and pervasive non-conformity to sex-typed behaviors (American Psychiatric Association, 2000). In children, quantitative measurement of sex-typed behavior is obtained through parent-report questionnaires as well as direct observation (Zucker, 2006a; Zucker & Bradley, 1995). In adolescents and adults with GID, descriptions of these childhood behaviors are obtained through retrospective self-report.
1.2.3 Gender Identity
Gender identity refers to a person’s basic sense of self as a male or female, that is, the inner experience of belonging to one gender (Fagot & Leinbach, 1985; Stoller, 1964). Most individuals develop a gender identity that is congruent with their biological sex, such that most biological females have a “female” gender identity and most biological males have a “male” gender identity. From a cognitive-developmental standpoint, gender identity refers to a child’s ability to not only accurately discriminate males from females, but to also correctly identify his or her own gender status as a boy or a girl. Within this framework, the development of gender identity is a cognitive milestone and is thought to represent the first stage in achieving gender constancy, that is, the understanding that being male or female is a biological characteristic and cannot be changed by altering superficial attributes, such as hair style or clothing (Fagot & Leinbach, 1985).[1] In typically developing children, gender identity is established by age 3, at which point children can correctly answer the question, “Are you a boy or are you a girl?” Gender constancy is, on average, established by age 7. The development of a gender identity carries affective significance, as evidenced by the intensity of children’s “emotional commitment to doing what boys and girls are supposed to do” (Fagot & Leinbach, 1985, p. 687). It is also evidenced by the pride with which young children announce their gender and the embarrassment experienced if they are mislabelled by others (Zucker, 2005c).
1.2.4 Gender Dysphoria
The term gender dysphoria refers to the subjective experience of dissatisfaction and discontent about one’s biological status as male or female (Fisk, 1973; Zucker, 2006a). The concept of gender dysphoria is fundamental to clinical work with children, adolescents, and adults with GID as it captures the distress that results from the incongruity between one’s biological/assigned sex and internal experience of gender identity (Cohen-Kettenis & Gooren, 1999; Cohen-Kettenis & Pfäfflin, 2003; Money, 1994). In the DSM-IV criteria for GID (Appendix A), Criterion A1 (“repeatedly stated desire to be, or insistence that he or she is, the other sex”) can be considered the most concrete and direct expression of gender dysphoria (Zucker, 2010a). There are, however, developmental influences on the way in which children, adolescents and adults express their gender dysphoria. Cognitive development, language capacity, and social desirability are among some of the factors that may influence an individual’s expression of gender dysphoria.
Young children may actually state that they are members of the opposite sex (Cohen-Kettenis & Pfäfflin, 2003; for case examples, see Zucker, 1994; Zucker & Green, 1992). Although this misclassification could be related to the child’s age and cognitive development, it may also reflect the severity of the gender dysphoria if the child does truly believe he/she is of the opposite gender. However, most children with GID do not generally misclassify their sex and they know that they are male or female. Thus, when asked, “Are you a boy or a girl,” they answer correctly (Zucker et al., 1993); however, they will voice the desire to be of the opposite sex and find little that is positive about their own sex (Zucker & Green, 1992). Some children may express the wish to be of the opposite sex (i.e., implying that they know which sex they belong to) and simultaneously insist that they are of the opposite sex (e.g., Zucker, 2000, 2006c). These children may have confusion over gender constancy and may be uncertain whether changing aspects of one’s behavior (e.g., hair, clothing) will also change one’s gender. In fact, young children with GID demonstrate more cognitive confusion about gender compared to controls and appear to have a “developmental lag” in their gender constancy acquisition (Zucker et al., 1999).
There is some evidence that overt statements to be of the opposite sex tend to diminish with age. Older children with GID may not verbalize the wish to be of the opposite sex, perhaps for social desirability reasons (Bates, Skilbeck, Smith, & Benter, 1974). For example, they may have received feedback directly or indirectly from parents and peers regarding the appropriateness of their cross-gender wish (Bradley, 1999; Zucker & Bradley, 2004). During clinical evaluation, it is not uncommon for older children who are struggling with their gender identity to not endorse the desire to be of the opposite sex, but later in therapy reveal their cross-gender wishes once they have developed feelings of security in the therapeutic relationship. Indeed, during the preparation phase for the DSM-IV, this clinical observation served as the rationale for collapsing of the verbalized wish to be of the other sex with the other behavioral indicators of cross-gender identification (Bradley et al., 1991). In the DSM-III, the desire to be or insistence that one is of the opposite sex was a required criterion for the diagnosis. Zucker and Bradley (1995) conducted a re-analysis of data from Green’s (1987) follow-up study of effeminate boys and found some research data to support this clinical observation. Of the 60 boys seen in childhood for effeminate behavior, 47 were 3-9 years old and the remaining 13 were 10-12 years old. Of the 47 younger boys, 43 (91.5%) were reported by their mothers to occasionally or frequently state the wish to be a girl, compared to 9 (69.2%) of the boys in the older age group.
That overt statements to be of the opposite sex tend to diminish with age may not be a cross-national observation in children with GID. Wallien et al. (2009) compared a sample of children with GID seen at a specialized gender clinic in Toronto to a sample of children with GID seen at a gender clinic in the Netherlands on the Gender Identity Interview, which is a self-report measure of cognitive and affective gender identity confusion. An age effect was found for the Toronto patients such that the youngest children in the sample (5 years of age and younger) reported more cross-gender feelings than did the older children (6-12 years). In contrast, there was no significant association between age and scores on the Gender Identity Interivew for the Dutch patients. Thus, in the Dutch sample, older patients were as likely to report cross-gender feelings as younger patients.
For developmental reasons, there are limitations on children’s ability to think abstractly about gender and to evaluate the meaning of their gender dysphoria. It is not uncommon that when asked to list reasons for wanting to be of the opposite sex, young children with GID will provide concrete advantages. As an example, one 8-year old boy with GID asserted that it would be better to be a girl because they have better bands, such as the Spice Girls (Zucker & Bradley, 2004). The extent to which a child engages in sex-typed behaviors typical of the opposite sex and their rejection of activities and clothing typical of their own sex can be construed as surface indicators of gender dysphoria. Some children may experience discomfort with their sexual anatomy, which serves as another indicator of their felt gender dysphoria.
Adolescents and adults with GID are generally more straightforward than children in their expression about their unhappiness with their biological sex. In adolescents and adults with GID, verbalization of an intense discomfort with both primary and secondary sex characteristics and the desire for medical treatment (e.g., hormonal treatment, sex reassignment surgery) to address this discomfort is one of the most salient ways in which gender dysphoria is expressed (Cohen-Kettenis & Pfäfflin, 2010; Zucker, 2010a). However, the experience of gender dysphoria does not necessarily imply a desire for sex-reassignment surgery as some adolescents are only interested in hormonal treatment for their gender dysphoria (Cohen-Kettenis & Pfäfflin, 2010). Compared to children, adolescents and adults with GID, on average, have the cognitive and language capacity to think abstractly about their gender identity and gender subjectivity (i.e., beyond surface behaviors) and dialogue about the meaning of their dysphoria and its genesis. They are also more capable of discussing their anatomic dysphoria, which is often at the core of their distress (Bower, 2001). In such discussions, it is not uncommon for these individuals to express feeling trapped or having been born in the wrong body (e.g., Shaffer, 2005).
1.2.5 Sexual Orientation
Sexual orientation refers to a person’s erotic responsiveness to sexual stimuli and is typically measured along the dimension of the sex of the person to whom one is sexually attracted, that is, whether one is attracted to a member of the opposite sex (heterosexual sexual orientation), the same sex (homosexual sexual orientation), or both sexes (bisexual sexual orientation) (LeVay, 1993; Zucker, 2006a; Zucker & Bradley, 1995). Individuals who do not experience sexual attraction are referred to as asexual. Sexual orientation is often assessed with regard to at least two parameters: sexual orientation in fantasy and sexual orientation in behavior (Diamond, 1993; Green, 1987; Sell, 1997). The former refers to erotic fantasies experienced during sexually stimulating events, such as masturbation or while watching erotic pictures or movies, and the latter refers to actual sexual behavior, such as kissing and intercourse.
In contemporary sexology, the assessment of sexual orientation may include psychophysiological techniques to measure sexual arousal (Chivers, Rieger, Latty, & Bailey, 2004), semi-structured interviews (Kinsey, Pomeroy, & Martin, 1948), and self-report questionnaires (e.g., Zucker et al., 1996). From the foregoing definitions, that gender identity and sexual orientation are distinct constructs is obvious, yet, unfortunately, these terms are often conflated (for discussion, see Drescher, 2010b). As discussed later, synonymous use of these terms has implications for how one conceptualizes therapeutic approaches to help children with gender dysphoria feel more comfortable about their biological sex.
1.2.6 Sexual Identity
Sexual identity refers to an individual’s experience and conception of their sexual attraction (Diamond, 2000). Thus, it is the individual’s recognition, definition/labelling, and acceptance of themselves as heterosexual, bisexual, or homosexual (Diamond, 2002; Savin-Williams & Diamond, 2000). It is important to uncouple the construct of sexual orientation from the construct of sexual identity as they are not always synonymous. For example, a person may be predominantly sexually aroused by homosexual stimuli but may not necessarily regard or accept himself as “homosexual” (e.g., Bailey, 2009; LeVay, 2011; Ross, 1983).
1.2.7 Transgender and Transsexualism
The word transgender is an informal (i.e., non-diagnostic) term broadly used to subsume expressions of gender variance or gender nonconformity regardless of whether criteria for GID are met. Typically, individuals who are considered transgendered exhibit significant cross-gendered behaviors or identity. Some adolescents and adults use the term as a self-label of their gender identity (e.g., “I am transgendered” or “I am a trans person”) (Lawrence & Zucker, 2012). The term does not imply a particular sexual orientation (Drescher, 2010b).
Transsexualism, used sometimes synonymously with GID in adolescents and adults (e.g., Cohen-Kettenis & Pfäfflin, 2003; Simon, Zsolt, Fogd, & Czobor, 2011), is not an official diagnostic category in the DSM-IV (APA, 2000), although it is a diagnosis in the ICD-10 classification system that is given to adolescents and adults (World Health Organization, 1993). The term male-to-female transsexual (MtF) refers to biological males who identify as and desire to live (or are actually living) as females, but does not imply degree of transition to the female gender role (e.g., presenting socially, taking cross-sex hormones, received some type of surgical intervention) (Cohen-Kettenis & Gooren, 1999).
1.3 Phenomenology of Gender Identity Disorder
1.3.1 GID in Children
Although GID was only first introduced to the psychiatric nomenclature in the third edition of the DSM (American Psychiatric Association, 1980), its historical background extends over 150 years ago with case descriptions of individuals who experienced conflict over what is now referred to as their gender identity (see Zucker & Bradley, 1995). The incipient DSM-III diagnoses, Gender Identity Disorder of Childhood and Transsexualism, have since been modified into one overarching diagnosis, Gender Identity Disorder, with distinct criteria sets for children versus adolescents and adults, which reflect developmental variations in clinical presentation. In the present revised fourth edition of the DSM, the diagnosis (Appendix A) requires the presence of two components: (1) evidence of a strong and persistent cross-gender identification, which is generally manifested as the desire to be, or insistence that one is, the other sex and/or through the adoption of cross-sex behaviors, and (2) evidence of persistent discomfort with one’s biological sex and/or a sense of inappropriateness in the gender role of that sex, which, in males, is manifested through such behaviors as aversion towards rough-and-tumble play (American Psychiatric Association, 2000). The onset of cross-gender behaviors generally occurs during the preschool period, and signs of GID may be visible as early as two years of age (Cohen-Kettenis & Pfäfflin, 2003). Typically, the behavioral signs of GID precede overt statements about feeling like or wanting to be of the opposite sex (Green 1976, 1987). Parents of boys with GID often report that, from the moment their sons could talk, they insisted on wearing their mothers’ clothes and shoes and were predominantly interested in girls’ toys (Cohen-Kettenis & Gooren, 1999).
The phenomenology of GID in boys has been well-described elsewhere (e.g., Zucker & Bradley, 1995; Zucker & Cohen-Kettenis, 2008; Cohen-Kettenis & Pfäfflin, 2003). Boys with GID experience a strong psychological identification with the other sex, as evidenced by an array of sex-typed behaviors more characteristic of females and a rejection of sex-typed behaviors characteristic of boys (Green, 1976; Zucker & Bradley, 1995). Zucker (2002, 2008a) identified eight categories of sex-typed behavior relevant to the clinical picture of boys with GID: (1) identity statements, (2) dress-up play/cross dressing, (3) toy play, (4) roles in fantasy play, (5) peer relations, (6) motoric and speech characteristics, (7) involvement in rough-and-tumble play, and (8) statements about sexual anatomy. Boys with GID are usually interested in playing with girls’ toys, such as Barbie dolls, and are more intrigued by girls’ games and activities (e.g., skipping rope) than boys’ activities (e.g., hockey). Although they may be equally interested in play as same-aged peers, they tend to dislike and refrain from rough-and-tumble play and gravitate more towards female peers than male peers.
Some boys with GID do not typically object to wearing stereotypically masculine clothing (e.g., pants) in social settings, such as school, but will engage in cross-dressing when the setting is amenable (Zucker, 2010a) while others will insist on wearing female clothing in public and may demonstrate oppositional behavior if allowed to cross-dress only in private (e.g., Ehrensaft, 2011). In a recent approach to treatment of children with GID, some parents and clinicians allow and even encourage gender transition in childhood. Boys with GID treated within this approach demonstrate strong resistance to wearing male-typical clothing. Instead, they insist on dressing socially and privately in female-typical clothing and are allowed to do so as part of their social gender transition (for case examples, see English, 2011; Rosin, 2008; Spiegel, 2008).
In pretend and dress-up play, boys with GID often take on the female role (e.g., a princess or mother). As discussed earlier, some boys with GID express distress about being a boy and having a male body and some will verbalize the wish to be a girl (for clinical examples, see Zucker 2006c, Zucker et al., 2012b). Some boys with GID also experience “anatomic dysphoria,” which is a dislike of one’s genitals. They may verbalize this dislike, attempt to hide their genitals or pretend to have female genitalia (Cohen-Kettenis & Pfäfflin, 2003; Zucker & Bradley, 1995). Indeed, mothers of boys with GID rated their sons as experiencing higher dissatisfaction with their sexual anatomy compared to mothers of clinical and community control boys (Johnson et al., 2004; Lambert, 2009).
On a terminological note, in referring to children with marked cross-gender behavior, some authors avoid formal nosology (i.e., GID) and, instead, use alternative terms such as “gender nonconforming” or “gender variant” on the premise that these terms are less stigmatizing than GID. The issue in using non-standardized terminology is that the populations to which the term refers is less well defined. “Gender variant,” for example, may refer broadly to children who display varying degrees of cross-gender behavior, some of whom may meet diagnostic criteria for GID but others may not. Further complicating matters, it is not always clear in the literature whether “gender variant” was used as an alternative to GID or as a general term to represent all children with marked cross-gender behavior. Some authors, however, use these alternative terms when referring to children in non-clinical samples (e.g., Rieger, Linsenmeier, Bailey, & Gygax, 2008). In these cases, a gender nonconforming boy is one who is relatively feminine or less masculine compared with other boys and a gender conforming boy is one who is relatively unfeminine compared to other boys. In this thesis, GID is used to refer to children who meet criteria for GID and gender atypical/gender nonconforming is used when referring more broadly to children with marked cross-gender behavior whose GID status is unknown.
1.3.2 GID in Adolescents and Adults
A core characteristic of adolescents and adults with GID is psychological identification with the opposite sex (American Psychiatric Association, 2000). This generally manifests in the verbalization of an intense desire to be a member of the opposite sex. Some adolescents and adults with GID attempt to adopt the social role or “pass” as a member of the opposite sex through alteration of surface level physical attributes such as hair or clothing style. Another core characteristic of adolescents and adults with GID is discomfort with their sexual anatomy (anatomic dysphoria), though this is not experienced by all individuals with GID (American Psychiatric Association, 2000; Bradley & Zucker, 1997). Anatomic dysphoria may manifest as an interest in taking contra-sex hormones and, in some cases, receiving sex reassignment surgery to alter their physical appearance (Cohen-Kettenis, Delemarre-van de Waal, & Gooren, 2008; Cohen-Kettenis & Pfäfflin, 2003; de Vries, Steensma, Doreleijers, & Cohen-Kettenis, 2011a; Smith, van Goozen, & Cohen-Kettenis, 2001; Zucker, Bradley, Owen-Anderson, Kibblewhite, & Cantor, 2008; Zucker, 2006a). Treatment for adolescents with GID typically involves biomedical interventions that facilitate the transition from one gender to another. It is also recommended and, at times, required that the adolescent also engage in psychotherapy, though with a different treatment philosophy compared to psychotherapy for children with GID (Zucker et al., 2011; Zucker, Wood, Singh, & Bradley, 2012a). In general, this approach to treating adolescents and adults with GID is uncontroversial, though there may be cross-clinic/clinician variations in timing of treatment (e.g., minimum age for cross-sex hormones).
1.4 Prevalence of Gender Identity Disorder
More than 25 years ago, Meyer-Bahlburg (1985) characterized GID as a rare phenomenon. While there have been no formal epidemiological studies on the prevalence of GID in children, adolescents, and adults, other lines of evidence suggest that Meyer-Bahlburg’s observation still holds true. Information about the prevalence of cross-gender behavior in children has come from studies using the Child Behavior Checklist (CBCL) (Achenbach & Edelbrock, 1983), a parent-report measure of emotional and behavior problems. The CBCL[2] has two items that measure cross-gender identification, “Behaves like opposite sex” and “Wishes to be of opposite sex,” which can be summed (range, 0-4) to provide a composite of gender identity. In a Dutch study of 7526 7-year-old twin pairs from the general population, 4.7% of children had a summed score (across the two items) of 1 or higher (van Beijsterveldt, Hudziak, & Boomsma, 2006). More recently, Steensma, van der Ende, Verhulst, and Cohen-Kettenis (2012) reported on 879 Dutch children (406 boys, 473 girls) from the general population followed prospectively for 24 years. The mean age in childhood was 7.5 years (range, 4-11 years). Fifty one (5.8%) of the 879 children were classified as gender variant (i.e., summed score on gender identity items was 1 or higher), which is similar to the percentage found by van Beijsterveldt et al.
Since the 1960s, a number of studies have reported estimated prevalence rates for GID in adults (for a review, see Zucker & Lawrence, 2009). Rates have varied, in part, depending on the inclusion criteria (e.g., including individuals who have had, at least, hormonal treatment but have not necessarily had any surgical interventions vs. only including individuals who have had sex reassignment surgery). For example, De Cuypere et al. (2007) estimated that 1 in 12,900 biological adult males in Belgium have GID, while Weitze and Osburg (1996) estimated a prevalence rate of 1 in 42,000 in Germany. The estimated prevalence rate in most other studies have fallen within this range (i.e., 1/12,900-1/42,000). Based on these estimated rates, it seems reasonable to presume that the prevalence of GID is low. In Steensma et al.’s (2012) prospective study, only 1 (0.1%) of the 879 participants, a biological male, had undergone gender reassignment (cross-sex hormonal treatment and surgery) when followed up in adulthood.
1.5 Treatment of Children with Gender Identity Disorder
At present, there are three general approaches that guide the clinical management of children with GID, each of which rests on its own conceptualization of gender identity development and GID. It is beyond the scope of this thesis to review in detail treatment approaches and the debates surrounding them (for detailed reviews, discussions, and clinical examples see, for example, Dreger, 2009; Stein, 2012; Zucker, 2001a, 2006c, 2007, 2008b; Zucker & Bradley, 1995; Zucker et al., 2012b).
1.5.1 The Therapeutic Model
In one approach, the goals of treatment are: (1) to circumvent the consistently observed sequelae of GID (e.g., ostracism by peers, depression), (2) to help children feel more comfortable with their biological sex, thereby reducing/alleviating gender dysphoria, (3) to increase the likelihood of desistance of GID in adolescence and adulthood, and (4) to alleviate co-occurring socioemotional problems in the child or difficulties within the family dynamic that may play a role in the child’s gender confusion (e.g., Meyer-Bahlburg, 2002; Zucker & Bradley, 1995; Zucker et al., 2012b). Dreger (2009) labeled this approach the “therapeutic model,” in contrast to the “accommodating” model described below. However, depending on the clinician’s theoretical perspective on the etiology of GID, the specific interventions used may vary.
Some clinicians view cross-gender behaviors as a result of inappropriate learning and attempt to extinguish them using principles of behavior therapy (e.g., Reker & Lovaas, 1974). Zucker et al. (2012b) proposed a multifactorial theory in which cross-gender identification is influenced by several factors, including biological, psychosocial, psychological, and psychodynamic variables. Within this framework, a biopsychosocial model of treatment is used to address the underlying factors that contribute to the child’s cross-gender identification (e.g., socioemotional problems within the child, family dynamics). In addition to therapy with the child, intervention may also include parent and/or family counselling. Some clinicians use a strictly psychodynamic formulation in which GID is viewed as a defense against distress and anxiety. Thus, psychodynamically informed therapy is used to address the underlying factors that perpetuate this defensive response (Coates & Wolfe, 1997). Regardless of the etiological framework, a common thread among these clinicians is the assumption that it is possible to modify a child’s gender identity (e.g., Meyer-Bahlburg, 2002; Zucker, 2008b). In a variation of the therapeutic approach, clinicians in the Netherlands place the emphasis of treatment on concomitant emotional/behavioral problems in the child as well as family dynamics rather than on direct attempts to modify gender identity (Cohen-Kettenis & Pfäfflin, 2003; de Vries & Cohen-Kettenis, 2012). The rationale for this approach is that, if the concomitant problems have contributed to causing or maintaining the gender dysphoria, then the dysphoria will likely disappear by addressing these problems. de Vries and Cohen-Kettenis have recently referred to the approach used in the Netherlands as the “Dutch approach.”
Both the Dutch approach as well as that espoused by Zucker et al. (2012b) utilizes a developmental perspective to treatment. When gender dysphoria persists from childhood into adolescence, it is less likely alleviated by psychological intervention and more likely to be treated by hormonal and surgical interventions (e.g., Cohen-Kettenis & van Goozen, 1997; de Vries et al, 2011a; Zucker, 2006). Thus, the therapeutic approach for adolescents is one that supports transitioning on the grounds that it will lead to better psychosocial adjustment (Zucker et al., 2011, 2012b).
The therapeutic model has faced intense criticism because some clinicians have claimed that, in addition to treating gender dysphoria, they were also preventing homosexuality, which they viewed as disordered (e.g., Rekers, Bentler, Rosen, & Lovaas, 1977). Some critics of the therapeutic model, and of Zucker’s approach in particular, view it as “homophobic” and similar to reparative therapy that has been used in attempts to change an individual’s sexual orientation (e.g., Pickstone-Taylor, 2003). Most contemporary clinicians emphasize that the goal of treatment is to resolve conflicts associated with the GID, regardless of the child’s eventual sexual orientation (Cohen-Kettenis, 2001; Zucker & Cohen-Kettenis, 2008). Moreover, Bradley and Zucker (2003) have explicitly stated that they do not endorse the prevention of homosexuality as a therapeutic goal. However, some parents of children with GID who request treatment do so, in part, because they hope to prevent homosexuality in their child (Zucker, 2008c). The therapeutic approach has also been criticized on the grounds that it does not appreciate the distinction between children with GID (i.e., children with gender dysphoria) and children who show gender-variant behaviors but without concomitant gender dysphoria (e.g., Stein, 2012). Discussed later, this criticism is a reflection of a broader conceptual and diagnostic debate in the field regarding the conflation of GID proper with presumably innocuous cross-gender behavior.
1.5.2 Accommodation Model
A second approach to treatment of GID has been referred to as the “wait and see” or “accommodation model” (Dreger, 2009; Hill, Rozanski, Carfagnini, &Willoughby, 2005). Within this framework, there is no direct attempt to help the child feel more comfortable about their biological sex or to modify their cross-gender behaviors. Rather, parents are encouraged to support the child’s cross-gender behaviors in order to reduce feelings of stigmatization in the child and to promote the child’s overall adjustment (Ehrensaft, 2012; Menvielle, 2012; Menvielle & Hill, 2011; Menvielle & Tuerk, 2002;). Ehrensaft (2011), in her case description of a 6-year-old biological male, explained that, essentially, the family and therapist tolerate a state of “not knowing” until the child “unfolds an authentic gender identity and expression,” which may or may not be aligned with their biological sex. If a child’s “authentic gender self” is not aligned with their biological sex, early social gender transition is then supported (e.g., Ehrensaft, 2012). The accommodation treatment approach is viewed as supportive and accepting of children’s authentic gender role expression on the premise that it does not steer children down a particular gender path (e.g., Bocking & Ehrbar, 2005; Hill et al., 2005). It is arguable, however, that by allowing cross-gender behavior, one is, in fact, steering children down a cross-gendered path. More than two decades ago, Green (1987) speculated that boys whose parents do not attempt to discourage cross-sex behavior might be more likely to become transsexuals as adults. Within this treatment approach, there appears to be an assumption that gender identity can change as indicated by the recognition that some children who socially transition at an early age may want to reverse the gender role transition later on (Ehrensaft, 2012; Menvielle, 2012).
1.5.3 Early Transition Approach
A third, more recent, approach takes an extreme stance on childhood cross-gender behavior and has likely been fuelled by changing ideas about what constitutes appropriate expression of gender (Drescher, 2010a). In this model, pre-pubescent children with GID, sometimes as young as 5 years of age, are allowed and encouraged to socially transition from one gender to another (e.g., Vanderburgh, 2009; see also Brown, 2006; English, 2011; Rosin, 2008; Spiegel, 2008). There is no attempt to decrease cross-gender behavior and identification. A social transition may involve, for example, a biological male using a female name and registering at school as a female (e.g., Saeger, 2006). This approach is partly rooted in the assumption that the onset of cross-gender behavior is an indication of innate (cross) gender identity rather than as a sign of gender confusion or a GID. Further, it is argued that an early transition (i.e., before puberty) may circumvent associated mental health issues seen in individuals with GID (Vanderburgh, 2009). The role of the therapist is to help families navigate aspects of the transition process, such as advocacy within the social setting and educating families about the medical aspects of transitioning.
There are some serious concerns about this approach. The most striking implication of an approach that facilitates early transitioning is that it may steer some children down a transgendered path who might have otherwise not desired to transition as they progress in development. Proponents of the early transitioning model have not addressed how this approach fits conceptually or clinically with the finding that the majority of children with GID show a desistence in adolescence (e.g, Drummond et al., 2008; Green, 1987; Wallien and Cohen-Kettenis, 2008). This is an important issue because an approach that encourages transitioning in childhood assumes that these children would persist in their GID into adolescence, which is not supported by the follow-up studies of children with GID.
There have been no quantitative follow-up studies on children who socially transition in childhood, probably, in part, because this approach is still relatively recent. However, one qualitative study conducted in The Netherlands suggests that socially transitioning children is not without its drawbacks (Steensma, Biemond, Boer, & Cohen-Kettenis, 2011). In this study, 25 adolescents who had met criteria for GID in childhood were interviewed regarding stability/instability of their gender identity from childhood into adolescence, among other things. The results of two adolescent (biological) females are of relevance to this discussion. In childhood, these females were seen and treated as boys by other children and they dressed in male-typical clothing all the time. It is unclear, however, the extent to which these females were socially transitioned (e.g., name and pronoun use). In adolescence, both girls experienced a desistence of their gender dysphoria and wanted to live in the female gender role. Both girls found it a struggle to attempt living in the female role after having lived to some extent in the male gender role. One girl commented, “At high school, I wanted to make a new start. I did not want people to know that I had looked like a boy and had wanted to be a boy in childhood.” While it is arguable that an approach that supports social transition in childhood may be beneficial to children who will turn out to be persisters, it is not the advisable approach for children who will desist. The challenge, however, is the difficulty in predicting the gender identity outcome of very young children with GID (Steensma & Cohen-Kettenis, 2011).
To date, there is no consensus on the best treatment approach for children with GID. This state of affairs has been maintained by the paucity of empirical data on treatment and also, in part, by theoretical disagreements among clinicians about gender identity development and its malleability in childhood. As a point of agreement, proponents of both the therapeutic and accommodation model agree that, if it is apparent that an adolescent is committed to transitioning, the recommended treatment approach is to provide cross-sex hormonal therapy, to be followed by surgery, if desired, in adulthood. Unfortunately, the debate about therapeutics for children is far from over largely because of scant research attention in this area. There have been no rigorous treatment outcome studies on children with GID and, certainly, no randomized controlled treatment trials that have compared the effects of these therapeutic approaches on gender identity outcome (Bradley & Zucker, 2003; de Vries & Cohen-Kettenis, 2012; Zucker, 2001a). In addition, there have been no studies that compared any of the different treatment approaches for GID to a condition of no treatment. Beyond resolving debate, there is an even more important reason to evaluate treatment approaches. As noted previously, most children with GID seem to desist in their gender dysphoria by adolescence. It remains unknown whether the aforementioned treatment approaches are associated with different long term outcomes (e.g., persistence vs. desistence of GID, general psychiatric functioning, psychosocial adjustment).
GID is arguably one of the most contentious diagnoses in the DSM. A detailed review of the controversies surrounding the diagnosis is beyond the scope of this chapter, but can be found elsewhere (e.g., Bockting, 2009; Bradley & Zucker, 1998; Bryant, 2006; Drescher 2010a, 2010b; Hill et al., 2005; Meyer-Bahlburg, 2010; Wilson, Griffin, & Wren, 2002; Zucker & Bradley, 1995; Zucker, Drummond, Bradley, & Peterson-Badali, 2009). Essentially, one group of critics argue for a reform of the diagnosis while a second group question the legitimacy of GID as a diagnostic category.
1.6.1 Diagnostic Reform
One major criticism of the GID diagnosis is that it fails to differentiate between children who have both cross-gender identity (gender dysphoria) and pervasive cross-gender behaviors from those who show signs of pervasive cross-gender behavior but without the co-occurring unhappiness about their biological sex (i.e., without co-occurring gender dysphoria) (Bockting, 1997). In the current form of the GID diagnosis (Appendix A), the Point A criterion is met if a child has at least 4 of 5 markers of persistent cross-gender identification: the desire to be, or insistence that one is, of the other sex (Criterion A1) and marked/pervasive cross-gender role behaviors, such as peer and clothing preference (Criteria A2-A5). Critics have argued that Criterion A1 (which is viewed as capturing gender dysphoria) should not be condensed with criteria pertaining to cross-gender behaviors; otherwise, a child may receive a diagnosis of GID through demonstration of cross-gender behaviors but in the absence of gender dysphoria (e.g., Bartlett, Vasey, & Bukowski, 2000; Bockting & Ehrbar, 2005; Hill et al., 2005; Richardson, 1996, 1999; Wilson et al., 2002). The concern is that a diagnosis and subsequent treatment may be harmful to the child (e.g., Langer & Martin, 2004). Presumably, these critics are arguing that the absence of verbal statements of cross-gender identification or wish is an indicator that the child is not gender dysphoric, regardless of the degree of cross-gender behavior. However, as discussed earlier, a child may experience unhappiness with their biological sex but not verbalize it. It is conceptually possible for children to meet diagnostic criteria for GID if they endorse items A2-A5 and also express unhappiness about their sexual anatomy (i.e., anatomic dysphoria, Criterion B), but yet do not make explicit statements of wanting to be of the opposite sex. These children may actually be struggling with their gender identity and, without a diagnosis, the way in which the cross-gendered behaviors are managed may not be in the best interest of the child (Zucker, 2010a). From a clinical standpoint, however, it is not common for a child to express anatomic dysphoria but not verbalize cross-gender identification.
It has been recommended that the diagnostic criteria be revised such that a distinction is made between children who have both cross-gender identification (manifested as explicit statements of wanting to be of the opposite sex) and cross-gender behaviors from children who only demonstrate cross-gender behaviors (e.g., Bartlett et al., 2000). Zucker (2005c) suggested that one solution to this debate is a modification of the DSM-IV diagnostic criteria such that it would be necessary for the child to systematically verbalize the wish to be of the opposite sex in order for the Point A criterion to be met. In a re-analysis of a parent-report measure of cross-gender identification, Zucker (2010a) found that children who frequently stated the desire to be of the other gender also showed more pervasive cross-gender behaviors. In part because of this finding, the DSM-5 Workgroup on GID has recommended that the persistent desire to be or insistence that one is of the opposite gender should be a necessary criterion for the diagnosis of GID. It is hoped that this change would result in a tightening of the diagnostic criteria and may better separate children with GID from those displaying marked variance in their gender role behaviors but without the desire to be of the other gender. The proposed revision to the DSM-IV diagnostic criteria for GID in children is summarized in Appendix B. The Workgroup on GID proposed retention of the diagnosis in DSM-5 with a name change (“Gender Dysphoria in Children”). In addition to statements of cross-gender identification (Criterion A1), children need to have at least 5 of 7 other manifestations of incongruence between expressed and assigned gender. In the proposed diagnostic criteria, rejection of sex-typical toys, games and activities, and anatomic dysphoria are part of Point A criteria. Point B criteria pertain to distress or impairment.
1.6.2 Is GID a Mental Disorder?
That GID is not a mental disorder and should, therefore, be removed from the DSM has been argued from at least four perspectives: (1) the GID diagnosis pathologizes normal variation in gender role expression, (2) children with GID are not impaired or inherently distressed, (3) the diagnosis was introduced to the DSM as a veiled attempt to repathologize homosexuality, and (4) GID is a childhood manifestation of homosexuality.
It has been argued that the cross-gender behaviors observed in children with GID are no more than normal, though sometimes extreme, variation in gender role behavior. The GID diagnosis, therefore, pathologizes children who exhibit harmless gender non-conformity and who are simply expressing their interests and inherent tendencies (e.g., Langer & Martin, 2004; Pickstone-Taylor, 2003). Proponents of the GID diagnosis argue that this line of thinking represents biological essentialism and is a simplistic view of a complex phenomenon that is influenced by biological, psychological, and interpersonal processes (Bradley & Zucker, 2003; Zucker, 2006b; Zucker et al., 2012b). Thus, while the critics who argue for a reform of the diagnosis recommend that the criteria should be more stringent to better distinguish gender dysphoric from non-gender dysphoric children with cross-gender behaviors, these critics argue that all children who receive the GID diagnosis are actually displaying nonpathological gender nonconformity.
The GID diagnosis has also been criticized on the grounds that it does not meet the criteria for a mental disorder because children with GID do not show evidence of inherent distress or impairment in functioning (Point D criterion), and, if they do experience distress or socioemotional difficulties, it is simply a reaction to social intolerance of their cross-gender behaviors (e.g., Bartlett et al., 2000; Menvielle, 1998; Wilson et al., 2002). Some argue that the disorder is more a reflection of a gender oppressive society rather than signaling a disorder within the individual (Ault & Brzuzy, 2009). Supporters of the diagnosis have provided compelling reasons to retain GID in the diagnostic nomenclature (Bradley & Zucker, 1998, 2003). For instance, clinic-referred children with GID sometimes verbalize significant unhappiness over their status as males or females and often state the desire to change themselves into the opposite gender (for clinical examples, see Zucker et al., 2012b; Zucker & Bradley, 1995). It is also argued that, even in the absence of explicit statements to be of the opposite sex, pervasive enactments of cross-gender fantasies, such as through role-play and dress-up, is a behavioral manifestation of underlying unhappiness with one’s biological sex (Zucker, 2006b).
On a more political level, it has been argued that the inclusion of GID into the DSM was a veiled political maneuver to repathologize homosexuality, which was simultaneously removed from the DSM at the time that GID was introduced (e.g., Ault & Brzuzy, 2009; Sedgwick, 1991). Zucker and Spitzer (2005) noted that the DSM-III included a diagnostic category of ego-dystonic homosexuality; thus, there was no need for a backdoor diagnosis to replace homosexuality. These authors also brought attention to the fact that several clinicians and scientists who recommended the inclusion of GID in the DSM had argued in favor of delisting homosexuality.
The strong association between GID in childhood and homosexuality in adulthood has also added to the controversy surrounding the diagnosis. Follow-up studies of boys with GID have found that the most common outcome in adulthood is desistance of GID with a homosexual sexual orientation (e.g., Green, 1987). Some have interpreted this finding to mean that the cross-gender behaviors observed in children with GID is simply an early manifestation of later homosexuality (e.g., Minter, 1999) and, therefore, should not be pathologized or treated (e.g., Corbett, 1998; Isay, 1997). However, cross-gender behaviors in childhood are not isomorphic with a later homosexual sexual orientation. Some boys with GID grow up to have a later heterosexual sexual orientation (e.g., Green, 1987; Wallien & Cohen-Kettenis, 2008). A second response to this particular criticism is that what constitutes a mental disorder is its operational definition (Green, 2011). Thus, if a child meets diagnostic criteria for a disorder, it is irrelevant to the assignment of a current diagnosis whether the child will meet the diagnosis in the future.
As discussed above, GID is a controversial diagnosis. The diagnosis itself has received much criticism and there remains a significant lack of consensus in the field regarding clinical management of the disorder. Discussions and debates on best treatment practices have raised the issue of the long-term outcomes for boys with GID, particularly in regard to gender identity and sexual orientation (e.g., Zucker, 2008b), a topic now addressed in the present literature review.
1.7 Psychosexual Outcome of Boys with GID
One approach to understanding the developmental trajectory of boys with GID is to retrospectively assess the childhood experiences of adult male-to-female transsexuals. These studies have found that adolescents and adults with GID, particularly those with a co-occurring homosexual sexual orientation (in relation to their birth sex), invariably recall a pattern of childhood cross-gender behavior that corresponds to the DSM criteria for GID (Green, 1974; Smith, van Goozen, Kuiper, & Cohen-Kettenis, 2005; Zucker et al., 2006). However, given the potential problems with retrospective research (for an overview, see Hardt & Rutter, 2004), most notably that the recollections may not be accurate, the ideal methodology to understand the long-term outcome of boys with GID is to identify a group of such children and follow them prospectively. Since the 1960s, a number of such studies have been conducted. Of these, Green’s (1987) study and Wallien and Cohen-Kettenis’ (2008) study constitute the two most comprehensive long-term follow-up of boys with GID. In addition, the results of 6 other follow-up studies which utilized much smaller sample sizes are also summarized. For clarity, the results on gender identity outcome are presented first followed by the results on sexual orientation outcome. Across all studies, sexual orientation is classified in relation to birth sex.
1.7.1 Gender Identity Outcome of Children with GID
Zucker and Bradley (1995) summarized data from six published follow-up studies of
boys who displayed marked cross-gender behavior (Bakwin, 1968; Davenport, 1986; Kosky, 1987; Lebovitz, 1972; Money & Russo, 1979; Zuger, 1978). The results of these studies are presented as a group due to the small sample size of each study. Across these six studies, a total of 55 boys were seen at follow-up (range, 16-36 years). Of these, 5 (9.1%) were classified as transsexual at follow-up (i.e., they showed persistent gender dysphoria). All 5 persisters had a homosexual sexual orientation.
One of the earliest prospective follow-up studies to utilize a reasonably large sample size was conducted by Green (1987). Green’s sample consisted of 66 behaviorally “feminine”[3] boys and 56 control boys[4] who were unselected for their gender identity. Both groups of boys were initially assessed at a mean age of 7 years (range, 4-12 years) and were recruited through various forms of advertisement. Although Green did not utilize a formal DSM diagnosis,[5] from his clinical descriptions it appears that most of the behaviorally feminine boys would have met criteria for GID. Most of the feminine boys stated their wish to be girls or to grow up to be women, avoided male-typical activities (e.g., rough-and-tumble play, sports), preferred female roles in pretend play, and showed a preference for girls’ clothes, toys, and peers (Green, 1974, 1976). Forty-four feminine boys and 35 control boys were available for follow-up assessment in adolescence and adulthood (M age, 18.9 years; range, 14-24). Only a minority of the feminine boys (n = 12) received formal therapy between the childhood assessment and the follow-up interview. At follow-up, only one (2.3%) of the 44 behaviorally feminine boys continued to experience gender dysphoria and desired sex reassignment surgery. None of the control boys reported any gender dysphoria.
More recently, Wallien and Cohen-Kettenis (2008) conducted the largest follow-up study to date on boys and girls with GID (77 children; 59 boys, 18 girls). The childhood data were collected as part of the standard assessment of children seen in their specialized gender identity clinic in The Netherlands. At follow-up, 54 participants (40 boys, 14 girls) were successfully traced and completed the follow-up assessment. The remaining 23 participants (19 boys, 4 girls) could not be traced. However, Wallien and Cohen-Kettenis assumed that these untraced participants were desisters on the premise that had they been persisters they would have likely had contact with the clinic and, therefore, included them in the calculation of a persistence rate. Of the 77 children followed prospectively, Wallien and Cohen-Kettenis reported that 21 (12 boys, 9 girls) were still gender dysphoric at follow-up, which yielded a persistence rate of 27% for the total sample of boys and girls with GID. However, when calculated based only on those participants who were actively involved in the follow-up assessment (i.e., excluding the 23 participants who could not be traced at follow-up), the persistence rate was 38.8%.[6]
For comparative purposes, I provide additional details for the boys in Wallien and Cohen-Kettenis’ study. The mean age for all 59 boys was 8.3 years (range, 5-12 years) at the initial assessment and 19.4 years (range, 16-28 years) at follow-up. Unfortunately, separate demographic data were not available on the subgroup of boys who were successfully contacted at follow-up. When calculated using only the 40 boys who were successfully traced at follow-up, the rate of persistent gender dysphoria was 30% (12 persisters, 28 desisters). If, however, one used Wallien and Cohen-Kettenis’ more liberal calculation of persistence by also including the 19 boys who could not be traced and classifying them as desisters, the persistence rate for boys was 20.3%.[7] All of the persisters met complete diagnostic criteria for GID at follow-up, were treated with puberty suppressing hormonal treatment before the age of 16, and with cross-sex hormones after the age of 16 years.
The rates of GID persistence found by Wallien and Cohen-Kettenis (2008), regardless of whether one uses the liberal or conservative calculation, were considerably higher than that reported by Green (1987) (in fact, more than 8 times as high) and approximately 2-3 times as high as the rate found by Zucker and Bradley (1995) in their review of six studies.[8]
Wallien and Cohen-Kettenis’ sample size was large enough to allow for group comparisons to identify potential differences in childhood between the boys who persisted in their gender dysphoria from those who desisted.[9] There was a significant difference between the persisters and desisters on the diagnosis received in childhood. All of the boys who showed persistent gender dysphoria had met the full criteria for GID in childhood. However, of the 28 (traced) boys who desisted, 17 met full criteria for GID while the remaining 11 were subthreshold. Of the 19 boys who could not be traced at follow-up, 15 met full criteria for GID and 4 were subthreshold. The persisters were also more extreme in their childhood cross-gender behaviors and identification on two dimensional measures, both of which were also used in the present study: (1) the Gender Identity Interview for Children (Wallien et al., 2009; Zucker et al., 1993), a child-report measure, and (2) the Gender Identity Questionnaire for Children (Johnson et al., 2004), a parent-report measure.[10] These data indicated that boys with more extreme cross-gender identification in childhood were more likely to be persisters than desisters.
1.7.1.1 Methodological Issues
Two methodological issues regarding the follow-up studies need to be mentioned. First, with the exception of Green’s (1987) study, none of the follow-up studies included a clinical control group (i.e., referred for reasons other than gender identity concerns) or community control group. Therefore, interpretation of follow-up data relied on evidence from the literature on adults with GID (Zucker, 1985). Second, during the follow-up assessments, particularly those in which data were obtained through clinical interview (e.g., Green, 1987), participants were asked to discuss an extremely sensitive and personal aspect of their lives–their psychosexual development. Due to the potential effects of social desirability on participants’ responses, it is possible that the rates of persistent gender dysphoria (and also homosexual outcomes) in these studies were an underestimate. It is unlikely that participants would have reported a homosexual or GID outcome if, in fact, they were not homosexual or experiencing gender dysphoria; thus, an overestimation was unlikely to have occurred. Unfortunately, social desirability was not measured by Green or Wallien and Cohen-Kettenis; thus, the effects of this phenomenon on their respective results are unknown.
1.7.1.2 Process of GID Desistence
There have been no quantitative follow-up studies that have systematically examined the developmental process through which GID desists (e.g., how and at what age). Some authors suggest that desistence typically occurs sometime around puberty or early adolescence (de Vries & Cohen-Kettenis, 2012; Wallien & Cohen-Kettenis, 2008). However, one should be skeptical in viewing puberty as the transformative period in the lives of children with GID with regard to their gender identity. Some gender-referred children show changes in their gender identity before puberty and, in fact, desist in their dysphoria during childhood (for case examples, see Zucker, 2006c; Zucker & Bradley, 1995).
The results of a recent qualitative study by Steensma et al. (2011) suggested that desistence may occur between the ages of 10-13 years and is likely influenced by psychosocial and psychosexual factors. In this study, 25 adolescents (13 boys, 12 girls; M age, 15.88 years; range, 14-18) who had been seen in a specialized gender identity clinic in The Netherlands in childhood and diagnosed with GID were contacted in adolescence for a follow-up interview. During the follow-up interview, participants were asked to discuss their childhood gender role behaviors, stability of gender identity, sexual orientation, and physical development. Thus, the data on childhood gender-role behavior and change in gender identity between the initial assessment and follow-up were based on retrospective recall. The primary goal of the study was to obtain qualitative data on the developmental course of GID, including factors that contributed to GID persistence and desistence. Of the 13 biological males in this study, 7 had applied for sex reassignment surgery and can, therefore, be considered persisters. The remaining 6 were desisters. One should not, however, extract a persistence rate from these data because this was not the goal of this study. Second, persistence and desistence were not clearly operationalized. Third, as this was a qualitative study, there was no quantitative comparison between the participants and non-participants and differences between the groups could have affected gender identity outcome. Thus, given that the participants might have represented a biased sample, caution should be exercised in drawing conclusions about the obtained persistence rate.
Several findings from this study warrant mention. First, both persisters and desisters recalled that around the age of 6 or 7 years they started to identify with and expressed a wish to be of the opposite sex, though they had exhibited cross-gender behavior prior to this. The underlying “motives” for childhood cross-gender identification appeared to be different for the persisters and desisters. The persisters recalled having felt as though they were the opposite sex. In contrast, the desisters recalled having wished they were of the opposite sex but did not feel they were the opposite sex. Second, the period from age 10 to 13 years of age appeared to be significant in the developmental trajectory for both persisters and desisters. Both groups of adolescents reported that three factors affected their feelings of gender dysphoria and either lessened or intensified it: their social environment (e.g., peer relations), anticipation about and experience of puberty, and emerging sexual attraction. This study highlighted the need for studies to prospectively follow children with GID beyond adolescence and into adulthood while periodically monitoring stability and change in their psychosexual development, particularly during the transition from childhood to adolescence. For example, one of the males in the desister group continued to experience some feelings of gender dysphoria but was not interested in living as woman. As the authors noted, a longer follow-up period may help to clarify whether this participant was experiencing protracted gender dysphoria that would eventually diminish or whether some form of mild gender dysphoria would remain a stable aspect of his psychological functioning.
The results of Steensma et al.’s study can be considered preliminary given the small sample size and retrospective recall of gender experiences from assessment to follow-up. This study also represents the first attempt in the literature to account for the process through which GID persists or desists. Future studies utilizing a prospective systematic design (i.e., regular follow-up intervals following the childhood assessment) with quantitative measurements of relevant variables are needed. Further, there are other factors beyond those examined by Steensma et al. that may potentially contribute to the developmental course of GID (e.g., psychiatric functioning, psychotherapy) and that would require empirical investigation.
1.7.2 Gender Identity Outcome of Adolescents with GID
Clinical observation and empirical evidence suggest that persistence of gender dysphoria, including the desire for sex change, is higher among patients assessed for the first time during adolescence and then followed up than among patients first assessed in childhood and then followed prospectively (Zucker & Bradley, 1995).
Cohen-Kettenis and van Goozen (1997) reported follow-up data on 33 adolescents with GID seen at a specialized gender identity clinic in The Netherlands. Of the 33 adolescents (M age at initial assessment, 17.5 years; range, 15-20), 22 (66.6%) went on to receive cross-sex hormonal therapy and some form of sex reassignment surgery. Of the remaining 11 adolescents, 8 were not diagnosed with “transsexualism” (presumably, they did not meet criteria for GID) and were, therefore, not recommended for sex reassignment surgery. The remaining 3 participants were diagnosed with transsexualism but, for a variety of reasons, including severe comorbid psychopathology, were not recommended for any cross-sex hormonal treatment. The “true” persistence rate of these adolescents could be higher than 66.6% because there were no data on whether any of the 11 participants who did not initially receive cross-sex hormonal or surgical interventions did so at a later date. This persistence rate of 66.6% is much higher than the persistence rates found in follow-up studies of boys who are first referred in childhood.
Zucker et al. (2011) reported on 109 adolescents who were assessed in the Gender Identity Service at the Centre for Addiction and Mental Health (CAMH) in Toronto, Canada. Of the total sample, 66 (60.6%) were recommended for puberty blocking hormonal therapy and 43 (39.4%) were not. The percentage of adolescents referred for hormonal therapy was similar to the 66.6% reported by Cohen-Kettenis and van Goozen (1997). It should be noted that the Zucker et al. study was geared towards examining which factors (e.g., demographic, psychosexual) influenced the clinical decision to recommend or not recommend puberty blocking hormones. Blockers were more likely to be recommended for those adolescents who were more extreme in their current gender dysphoria and childhood cross-gender behavior. Thus, while follow-up data were available for some participants, this study was not a systematic follow-up study per se. It would be informative to know whether the participants who did not receive blockers persisted or desisted in their gender dysphoria.
1.7.3 Sexual Orientation Outcome [11]
In their review of six follow-up studies of boys with GID (Bakwin, 1968; Davenport, 1986; Kosky, 1987; Lebovitz, 1972; Money & Russo, 1979; Zuger, 1978), Zucker and Bradley (1995) also summarized data on sexual orientation outcome. Of the 55 boys reported on in these studies, 13 were classified as “Uncertain” with regard to sexual orientation, in part, because they were not sexually active and data regarding sexual orientation in fantasy were not definitive. Of the remaining 42 cases, 26 (61.9%) were classified as homosexual (this includes the 5 individuals who were persisters with a homosexual sexual orientation) and 16 (38.1%) were classified as heterosexual. In these six follow-up studies, it is unclear if sexual orientation was classified according to fantasy or behavior.
In Green’s (1987) study, sexual orientation in fantasy and behavior was assessed using a semi-structured interview and rated using Kinsey’s 7-point scale where 0 = exclusively heterosexual and 6 = exclusively homosexual (Kinsey et al., 1948). Of the 44 feminine boys assessed at follow-up, 33 (75%) were classified as bisexual/homosexual in fantasy (Kinsey ratings of 2-6) and 11 (25%) were classified heterosexual in fantasy (Kinsey ratings of 0-1). Of note, the persister in Green’s study reported a homosexual sexual orientation, in both fantasy and behavior. Unlike the feminine boys, all of the clinical control boys were classified as heterosexual in fantasy. At follow-up, only 30 of the feminine boys reported having had sexual experience. Of these, 24 (80%) were classified as bisexual/homosexual in their sexual behavior and the remaining 6 (20%) were classified as heterosexual in behavior. In the control group, 25 of the 35 boys reported sexual experiences at follow-up. Of these, 1 (4.0%) was classified as non-heterosexual (he reported bisexual sexual experiences) and the others were classified as heterosexual. Therefore, depending on whether sexual orientation was classified according to fantasy or behavior, 75-80% of the 44 feminine boys were classified as bisexual/homosexual in their sexual orientation compared to only 0-4% of the control boys.
In Wallien and Cohen-Kettenis’ (2008) study, sexual orientation was assessed using the 9-item Sexual Orientation Questionnaire (SOQ) (http://links.lww/com/A569). Items on the SOQ pertained to four domains of sexual orientation: sexual behavior (4 items), sexual fantasy (2 items), sexual attraction (2 items), and sexual identity (1 item). Response options for questions pertaining to sexual behavior and fantasy reflected Kinsey’s 7-point scale. Although this study included biological males and females, only data for males are presented here. Of the 40 males who were contacted for follow-up, data on sexual orientation in fantasy were only available for 21. Of these, 17 (81%) were classified as bisexual/homosexual and 4 (19%) as heterosexual. Data on sexual orientation in behavior were available for 19 males (13 desisters, 6 persisters). Of these, 15 (79%) were classified as bisexual/homosexual and 4 (21%) were classified as heterosexual. When sexual orientation was examined according to gender identity outcome, [12] 10 (77%) and 13 (81%) of the desisters were classified as bisexual/homosexual in behavior and fantasy, respectively. The remaining desisters were classified as heterosexual, (3) 23% in behavior and (3) 19% in fantasy. For the 6 persisters on which requisite data were available, 5 (83%) were classified as bisexual/homosexual in both fantasy and behavior and 1 (17%) was classified as heterosexual in fantasy and behavior.
In the studies by Green (1987) and Wallien and Cohen-Kettenis (2008), most boys with GID later developed a bisexual/homosexual sexual orientation, with rates that ranged from 75-81%. These rates are substantially higher than the currently accepted base rate of a homosexual sexual orientation in males of 3.1% (Laumann, Gagnon, Michael, & Michaels, 1994).
That some males with GID develop a heterosexual sexual orientation in adulthood is not fully understood. It has been suggested that perhaps the degree of cross-gender identification may affect sexual orientation outcome (Zucker, 1985). On the latter point, Wallien and Cohen-Kettenis (2008) found a significant difference between their sexual orientation groups on a parent-report measure of childhood sex-typed behavior (the Gender Identity Questionnaire for Children). However, when these analyses were redone for the desisters only, the difference was no longer significant and suggested that the extreme cross-gender scores of the persisters was responsible for the overall group difference on this measure.
Green (1987) also examined the relationship between degree of cross-gender behavior in childhood and sexual orientation at follow-up. For all participants, Green (1987) computed a childhood composite “extent of femininity” score on the basis of six behaviors: cross-dressing, rough-and-tumble play, wish to be a girl, desire to be like father, attention to mother’s fashion, and female-type doll-play. Across the entire sample, there was a significant correlation between “extent of femininity” and sexual orientation; however, within the “feminine” group only, this association was not significant for sexual orientation in fantasy or behavior. Green (1987) concluded that the lack of “range” (i.e., variability) in “extent of femininity” and sexual orientation contributed to the insignificant finding.
Green also examined whether there were specific childhood features that distinguished which “feminine” boys developed a homosexual sexual orientation from those who developed a heterosexual sexual orientation. Of 14 variables of childhood sex-typed behavior, three variables were related to sexual orientation at follow-up: female role-play, doll-play, and female peers. With age at childhood assessment controlled for, preference for female peers and doll play were significantly correlated with sexual orientation in fantasy, but not behavior. Female role play was, however, significantly correlated with both fantasy and behavior (Green, Roberts, William, Goodman, & Mixon, 1987).
One criticism of these prospective studies is that they followed up children who showed extreme forms of cross-sex behavior and identification, most of whom were clinically referred. As such, the generalizability of these studies is limited to similar groups of children. In the context of this limitation, Steensma et al. (2012) conducted a 24-year prospective study of 879 (406 boys, 473 girls) non-clinically referred children, unselected for their gender identity, who were part of a population-based study (for a description of the study, see section on Prevalence of GID). At follow-up, sexual orientation was assessed by asking four questions, each of which pertained to a different domain of sexual orientation: sexual attraction (“To whom do you feel attracted?”), sexual fantasy (“About whom do you fantasize sexually?”), sexual behavior (“With whom do you have sexual contact?”), and sexual identity (“How do you identify yourself?”). For sexual attraction, fantasy, and behavior, participants’ responses were coded using Kinsey’s 7-point scale. At follow-up, 11 (2.7%) of the 406 boys were bisexual/homosexual in fantasy and 10 (2.5%) were bisexual/homosexual in behavior. Steensma et al. also examined sexual orientation outcome separately for the gender-variant (10 males, 41 females) and non-gender variant (396 males, 432 females) groups. Of the 10 gender variant boys, 2 (20%) were bisexual/homosexual in fantasy and behavior and the remaining 8 (80%) were heterosexual in fantasy and behavior. Of the 396 non-gender variant boys, 9 (2.3%) and 8 (2.1%) were bisexual/homosexual in fantasy and behavior, respectively. I used Fisher’s exact test to determine if these represented significant differences in sexual orientation across the two subgroups of boys (i.e., gender variant versus non gender-variant). For both fantasy and behavior, there was a significant difference in the number of boys classified as bisexual/homosexual versus heterosexual (both ps < .05). Depending on whether one looks at fantasy or behavior, the prevalence of bisexuality/ homosexuality in the gender variant boys was 8.7-9.5 times higher than the prevalence rate of bisexuality/homosexuality in the non-gender variant boys. Thus, when a sample of boys unselected for their gender identity were followed up into adulthood, those who were at the cross-gendered end of the spectrum were significantly more likely to develop a bisexual/ homosexual sexual orientation.
The rates of bisexuality/homosexuality obtained by Steensma et al. for the entire sample of males (2.5-2.7%) were substantially lower than those obtained by Green (1987) and Wallien and Cohen-Kettenis (2008) in their follow-up of boys with gender dysphoria. This difference is not surprising and may be attributable to sample differences; however, an interpretative caution is in order. Steensma et al. measured gender variance in childhood using 2 items on the CBCL; they did not include specific measures of gender identity, gender role, or gender dysphoria. Thus, the actual extent of cross-gender behaviors in their sample of males is unclear. On the other hand, the males in Green’s and Wallien and Cohen-Kettenis’ studies were extreme in their cross-gender behaviors on measures of gender identity and gender role. Given that the boys in Steensma et al.’s study were taken from the general population and were unselected for their gender identity it is likely, and expected, they would have significantly less cross-gender behaviors compared to the boys seen by Green and by Wallien and Cohen-Kettenis. Indeed, the rate of bisexuality/homosexuality obtained by Steensma et al. is similar to the base rate of a homosexual sexual orientation in males of 3.1% (Laumann, Gagnon, Michael, & Michaels, 1994). At the same time, and consistent with Green’s (1987) study, which included a control group, the gender variant boys in Steensma et al.’s study were more likely to develop a bisexual/ homosexual sexual orientation compared to the non-gender variant boys. Similar to the developmental course of GID, these results suggest that there may also be a dosage effect on sexual orientation outcome–the more gender variance in childhood, the higher the likelihood of homosexuality.
1.7.4 Gender Identity and Sexual Orientation Outcomes in Boys with GID: Summary
The prospective follow-up studies of boys with GID (or pervasive cross-gender behavior in the case of studies conducted prior to 1980) suggests that there are four outcomes: (1) persistence of GID, with a co-occurring bisexual or homosexual sexual orientation, (2) persistence of GID, with a co-occurring heterosexual sexual orientation, (3) desistance of GID, with a co-occurring homosexual sexual orientation, and (4) desistance of GID, with a co-occurring heterosexual sexual orientation. Of these, a desistence of GID with a co-occurring homosexual sexual orientation appears to be the most common (e.g., Green, 1987; Wallien & Cohen-Ketternis, 2008).
1.8 Retrospective Studies of Homosexual Men: Summary of Key Findings
As the current study utilized a longitudinal follow-up design, the results of retrospective studies are only briefly summarized to highlight the key findings and to inform the extent to which prospective and retrospective results converge. In the 1960s, 1970s, and 1980s, studies were conducted which identified significant differences between heterosexual and homosexual adults on their recollections of childhood sex-typed behaviors (e.g., Whitam, 1977). However, some authors were skeptical about these findings. Carrier (1986), for example, felt these results were obtained using skewed samples and, therefore, could not be generalized to all homosexual men and women. Following the publication of a meta-analysis by Bailey and Zucker (1995), the strong relationship between childhood sex-typed behavior and sexual orientation was more or less confirmed.
Bailey and Zucker reviewed 41 studies, 32 of which compared the recalled childhood (≤ 12 years of age) sex-typed behaviors of heterosexual and homosexual men. Bailey and Zucker found that, on average, homosexual men recalled substantially more cross-gendered behavior during childhood than heterosexual men. The effect sizes were large (Cohen’s d = 1.31) (Cohen, 1988) and “were among the largest effect sizes ever reported in the realm of sex-dimorphic behaviors.” The heterosexual and homosexual adults differed on various domains of childhood sex-typed behavior, including rough-and-tumble play, toy and activity preferences, role playing, cross-dressing, and preferred sex of peers. Several studies conducted after the Bailey and Zucker (1995) meta-analysis yielded similar results (e.g., Bailey & Oberschneider, 1997; Bogaert, 2003; Cohen, 2002; Zucker et al., 2006; for a review, see Zucker, 2008c).
Similar results have also been found in retrospective studies of non-Western cultures, including Samoa (Bartlett & Vasey, 2006), Turkey, and Thailand (Cardoso, 2009). As one example, Bartlett and Vasey conducted a retrospective study of childhood sex-typed behavior in the Samoan fa’afafine, Samoan men, and Samoan women. Fa’afafine are biological males who manifest gender atypical behavior. In Samoa, the fa’afafine are essentially a third gender group and, for the most part, self-identify as such. Some adult fa’afafine present socially as females through clothing choice, hair, voice, and mannerisms, while others adopt only some aspects of female gender roles. Most fa’afafine are androphilic, meaning they are sexually attracted to biological males. The fa’afafine recalled engaging in significantly more female-typical (e.g., playing with girls’ toys, putting on make-up) and less-male typical behaviors (e.g., playing with boys, playing rough sports) in childhood compared to men. Further, their recollections of childhood sex-typed behaviors did not differ significantly from those of Samoan women. Some fa’afafine also recalled an aversion towards male-typical activities.
Despite the consistency of retrospective studies, some authors continue to challenge that a relationship exists between childhood sex-typed behavior and adult sexual orientation, partly on the premise that retrospective recall of childhood behavior may be distorted (e.g., Gottschalk, 2003). A number of studies have utilized methodology that minimizes the chance of a recall bias and the results speak against the retrospective distortion hypothesis. In one study, researchers examined childhood gender nonconformity in homosexual and heterosexual adults by examining videos from their childhood (1-15 years of age) as a visual recording will not be susceptible to memory bias (Rieger, Linsenmeier, Gygax, & Bailey, 2008). The adults who self-labeled as homosexual were judged (by raters masked to their sexual identity) to be significantly more gender nonconforming as children than the adults who self-labeled as heterosexual. In another line of research that utilized heterosexual and homosexual participants, there was a significant correlation between the retrospective recall of childhood sex-typed behavior by the participants and ratings of the participants by his or her mother (Bailey, Miller, & Willerman, 1993; Bailey, Nothnagel, & Wolfe, 1995; Bailey, Willerman, & Parks, 1991).
In sum, the prospective data on sexual orientation outcome of boys with GID converge decently with retrospective studies of homosexual adults. Owing to these two lines of evidence, it is now generally accepted that childhood gender role behavior is not only strongly related to sexual orientation in adulthood in clinical and non-clinical samples but that it can also predict sexual orientation outcome (for a review, see Bailey & Zucker, 1995; Zucker, 2008c). There are, however, a few caveats to keep in mind. Some boys with GID followed prospectively into adolescence and adulthood have a heterosexual sexual orientation (e.g., Cohen-Kettenis & Wallien, 2008; Green, 1987). Studies that systematically examined childhood correlates of sexual orientation differentiation are needed to help us better understand this variability in outcome. As well, a proportion of homosexual men do not recall a childhood history of cross-gender behavior (Bailey & Zucker, 1995). Of the homosexual men who recall a cross-gendered childhood, it is unclear how many of these individuals would have met the full diagnostic criteria for GID as children.
1.9 Childhood Sex-Typed Behavior and Sexual Orientation: Explaining the Linkage
Both biological and psychosocial explanations have been offered to explain the linkage between childhood sex-typed behavior and sexual orientation (for reviews, see Green, 2008; LeVay, 2011; Zucker, 2008c).
1.9.1 Biological Explanation: Influence of Genes
One biological explanation is that childhood cross-gendered behaviors and adult sexual
orientation are strongly linked because they are both components of psychosexual differentiation that develop under the influence of genes. A number of studies have found that homosexuality is highly familial–gay men have more gay siblings than do straight men (e.g., Bailey et al., 1999; Bailey & Bell, 1993; Bailey, Dunne, & Martin, 2000; Bailey, Willerman, & Parks, 1991; Hershberger, 1997; Pillard, Poumadere & Carretta, 1982; Pillard & Weinrich, 1986; Schwartz, Kim, Kolundzija, Rieger, & Sanders, 2010). These studies have found that brothers of homosexual men are homosexual 7% to 22% of the time, with a median rate of approximately 10% (for reviews, see Bailey & Pillard, 1995; Mustanski, Chivers, & Bailey, 2002) which is well above the estimated base rate of homosexuality in the general population of biological males (Laumann et al., 1994). Differences across studies in recruitment process, assessment of sexual orientation, source of information (e.g., the gay men themselves reporting about their siblings vs. interviewing the siblings of gay men) likely account for the variation in these findings. That homosexuality tends to cluster in families could be attributed to genetic or shared environmental factors. If genes do contribute to sexual orientation, one would also expect a clustering of homosexuality among family members without shared environment (e.g., nonsibling relatives). Indeed, increased rates of homosexuality or bisexuality have been found among uncles and male cousins of gay men (Bailey, Bobrow, Wolfe, & Mikach, 1995).
Twin studies have supported a genetic interpretation of the familiality findings described above. One of the earliest twin studies of male homosexuality reported a 100% concordance rate for 37 monozygotic (MZ) twin pairs compared with a 15% rate for 26 dizygotic (DZ) pairs (Kallmann, 1952). This study has since been strongly criticized because subjects were primarily recruited from psychiatric institutions and because the methodology through which zygosity was established was not clearly delineated (Mustanksi, Chivers, & Bailey, 2002). The results of subsequent twin studies suggest that the concordance rates for homosexuality among MZ twins are much lower than 100% and appear to be closer to 50%. In a study of 115 male twin pairs, Bailey and Pillard (1991) found a concordance rate for homosexuality of 52% among MZ twins compared to 22% among DZ twins. Whitam, Diamond, and Martin (1993) found higher concordance rates: 65% for MZ twins and 29% for DZ twins. One criticism of these studies is that they relied on advertisement; thus, there may have been a self-referral bias such that gay individuals with a gay twin might have been more likely to respond to the study advertisement compared to gay individuals without a gay twin and this could have resulted in an inflation of concordance rates (Bailey, Dunne, & Martin, 2000; LeVay, 2011). More recent studies have examined concordance rates for homosexuality among pairs of twin from large registries that were created without reference to the twins’ sexual orientation and these have reported lower concordance rates compared to self-selected samples. In a study of Australian twins, for example, Bailey, Dunne, and Martin (2000) found a concordance rate of 20% among male MZ twins.
The findings from behavior genetics studies also support a genetic basis for homosexuality. In a reanalysis of the Australian twin data (Bailey, Dunne, & Martin, 2000), Kirk, Bailey, Dunne, and Martin (2000) estimated the heritability of homosexuality in males to be approximately 30%. In other words, genetic influences accounted for 30% of the variation of sexual orientation in men. In a more recent population based study of Swedish twins, the heritability of homosexuality in males ranged from 34%-39% (Längström, Rahman, Carlström, and Lichtenstein, 2010).
The strong relationship between cross-gender behavior in childhood and adult homosexuality combined with twin studies demonstrating a genetic basis for homosexuality raises at least two questions: (1) Is there a genetic basis for cross-gender behavior?; and (2) Is there a common genetic basis for both cross-gender behavior and sexual orientation? Bailey, Dunne, and Martin (2000) also measured childhood gender nonconformity of the twins in their study and found that heritability accounted for 50% of variance in recalled childhood gender nonconformity among men. Monozygotic twins who are both gay were more similar in their cross-gender behavior (correlation of gender nonconformity = .54) compared to dizygotic twins who are both gay (correlation of gender nonconformity = .14). Similar results were obtained by Alonko et al. (2010) in a study of Finnish twins taken from a national register: monozygotic (male) twins had higher correlations on both gender atypical behavior and sexual orientation (r = .56 and .50, respectively) compared to dizygotic twins (r = .27 and .25, respectively). These finding suggested that childhood gender nonconformity, like homosexuality, is heritable. In fact, a study of Dutch children taken from a national twin register, and who were therefore unselected for gender identity or sexual orientation, estimated that 70% of the variance in cross-gender behavior was accounted for by genetic factors (van Beijsterveldt, Huzdiak, & Boomsma, 2006). Alonko et al. (2010) found a large genetic correlation (r = .73) between gender atypical behavior and sexual orientation for the male twin pairs, which suggests that a shared set of genes is partially responsible for both childhood gender nonconformity and adult homosexuality.
1.9.2 Biological Explanation: Role of Prenatal Hormones
Another prominent biological explanation for the linkage between childhood sex-typed behavior and sexual orientation is that they are both influenced by common biological processes involving prenatal hormones. Research on biological females with congenital adrenal hyperplasia (CAH) provides evidence for the influence of prenatal hormones on sex-typed behaviors. In CAH, a defect in the enzyme involved in cortisol production results in the adrenal glands producing higher than normal levels of androgens. As the condition is recognized at birth and corrected, the period of abnormal androgen exposure is generally limited to the prenatal period. Data from several groups of researchers consistently show that girls with CAH show a male-typical pattern of toy and activity preferences from childhood through adulthood (for reviews, see Hines, 2002, 2010, 2011). For example, they are, on average, more active and aggressive than girls without CAH (e.g., Pasterski et al., 2007) and have toy preferences similar to those of boy (e.g, Berenbaum & Hines, 1992; Berenbaum & Snyder, 1995; Pasterski et al., 2005, 2011; Servin, Nordenström, Larsson, & Bohlin, 2003). Girls with CAH also appear to have an enhanced preference for boys as playmates (e.g., Pasterski et al., 2011; Servin et al., 2003) and engage in more rough-and-tumble play compared to unaffected girls (e.g., Pasterski et al., 2011).The extent of male-typed interests in childhood in females with CAH appears to be correlated with the degree of prenatal androgen exposure (Nordenström, Servin, Bohlin, Larsson, & Wedell, 2002).
In adulthood, women with CAH have a higher rate of bisexuality/homosexuality compared to unaffected women (Hines, Brook & Conway, 2004; Meyer-Bahlburg, Dolezal, Baker, Ehrhardt, & New, 2006; Meyer-Bahlburg, Dolezal, Baker, & New, 2006; Zucker et al., 1996). Women with CAH also report unhappiness with their female gender role and gender identity (e.g., Hines et al., 2004). In a review of the literature on women with CAH (total n = 250)[13], Dessens, Slijper, & Drop (2005) estimated that approximately 5% experienced gender dysphoria and 1.6% pursued a gender transition (see also for a review, Hines, 2010). These percentages are significantly higher than the estimated prevalence rate of FtM transsexualism in the general population of biological females (1:30,400) (Bakker, van Kestern, Gooren, & Bezemer, 1993). Based on their review, women with CAH were approximately 500 times more likely than women in the general population to experience severe gender dysphoria and transition to the male gender role. It has been argued that the excessive androgen exposure in women with CAH is the linkage factor that explains the behavioral masculinity in childhood and gender dysphoria and bisexuality/homosexuality in adulthood (Zucker, 2008c).
Most boys and adults with GID have normally developed genitalia (Green, 1976). Thus, if prenatal androgen levels are implicated in the etiology of GID, the effects are such that genital development is not affected in any obvious way. Animal studies have shown that there are different sensitive periods for prenatal androgen effects on behavior and genital anatomy. For example, in female rhesus macaques, Goy, Bercovitch, and McBrair (1988) were able to induce behavioral masculinization without accompanying genital ambiguity (i.e., the genitals were not masculinized) by altering the timing of prenatal androgen exposure. These results suggest that, depending on the timing of prenatal exposure to androgens, there may be subsequent effects on behavior, anatomy or both.
1.9.3 Psychosocial Explanations
Psychosocial theories have also been offered in explanation for the association between childhood sex-typed behavior and adult sexual orientation. Green (1987) theorized that, in childhood, pre-homosexual boys identify with their mothers and lack a close relationship with their fathers and other boys, which results in “male affect starvation.” In adolescence, homoerotic contact is used in some compensatory manner to achieve closeness with other males. It is unclear how this formulation would account for males who do not have a close relationship with their father or other adult males but grow up to be heterosexual. In Bem’s (1996, 2008) “exotic becomes erotic” theory of sexual orientation, biological factors influences a child’s temperament which, in turn, influences a child’s preference for same-sex versus opposite-sex peers. Children feel similar to the peers with whom they socialize and different from those with whom they do not socialize. This feeling of being different results in physiological arousal, which is then transformed to sexual arousal. For example, effeminate boys who prefer female peers initially feel different from boys and experience them as “exotic.” Later in development, these exotic feelings become erotic feelings. It is unclear how Bem’s theory would account for homosexual adults who were stereotypically masculine in childhood.
1.10 Associated Psychopathology in GID
One goal of the present study is to identify whether there are within-group childhood
characteristics, including childhood behavior problems, that were predictive of long-term outcomes of boys with GID. Thus, the remainder of this chapter will focus on associated psychopathology in GID and will conclude with a conceptual framework for and goals of the present study.
1.10.1 Children with GID
1.10.1.1 Behavior Problems in Children with GID
Studies on associated psychopathology in children with GID have taken two general approaches. One approach is to examine the presence of general psychopathology or behavior problems as would be reported on such measures as the CBCL. A second approach has been to examine the presence of other DSM diagnoses in children with GID.
Information on associated psychopathology or general behavior problems in children with GID has been systematically obtained from parent-report data on the CBCL. Using maternal-report data, Zucker and Bradley (1995) compared 161 gender-referred boys and 90 siblings on five indices of disturbance: the number of elevated narrow-band scales (T > 70), number and sum of items rated 1 or 2, and T scores for the Internalizing and Externalizing broad-band scales. On all five indices, gender-referred boys had significantly higher levels of behavioral disturbance compared to their siblings. Further, the boys with GID had significantly higher Internalizing T scores than Externalizing T scores; however, there was no significant difference between these scores for their siblings. Zucker and Bradley also compared 46 gender-referred boys pair-matched[14] to 46 clinical control boys on the five CBCL indices described above: there was no significant difference between the groups on any of the indices. Cohen-Kettenis et al. (2003) found similar rates of behavior problems in a cross-national, cross-clinic comparison of 358 gender-referred children assessed at the CAMH in Toronto and 130 gender-referred children assessed in The Netherlands. In this study, boys with GID also showed more internalizing than externalizing problems on the CBCL.
CBCL studies of gender-referred children have found two other noteworthy patterns. First, there appears to be a relationship between age and degree of behavior problems, with older children having more behavior problems than younger children (Cohen-Kettenis et al., 2003; Zucker & Bradley, 1995). For example, in the Cohen-Kettenis et al. study, 26.1% of 3- to 5-year-old children in the Toronto sample had a CBCL sum score that was in the clinical range (>90th percentile) compared to 62.1% of 6- to 12-year-old children. The corresponding percentages for the Dutch sample were 43.8% and 61.7%, respectively.
Second, children with GID appear to have more peer relationship difficulties compared to their siblings (Zucker, Bradley, & Sanikhani, 1997). Further, gender-referred boys seem to have poorer peer relationships and experience more negative social consequences for their cross-gender behavior compared to gender-referred girls (Cohen-Kettenis et al., 2003; Wallien, Veenstra, Kreukels, & Cohen-Kettenis, 2010). Cohen-Kettenis et al. also found that poor peer relations in boys with GID was a significant predictor of CBCL behavior problems and accounted for 32% of the variance. Thus, poor peer relations may mediate the relationship between cross-gender behavior and psychopathology.
These findings are not surprising. Even among children unselected for their gender identity, there is evidence that gender nonconforming behavior is associated with overall adjustment problems (Carver et al., 2003; Rieger & Savin-Williams, 2012; Yunger et al., 2004). Studies of children unselected for their gender identity have also demonstrated that children tend to react negatively to gender-atypical peers and may resist developing friendships with these children (Fagot, 1977; Martin, 1989) and effeminate boys, in particular, receive more negative feedback from peers than masculine girls about their cross-gender behavior (Blakemore, 2003; Fagot, 1977). In an observational study of playmate preferences, non-referred boys were more likely to choose another non-referred boy as a favourite playmate than to choose a boy with GID (Fridell, 2001). On the other hand, a recent study showed that gender referred children are accepted by peers of the opposite sex and have better relations with opposite-sex than same-sex peers (Wallien et al., 2010). Thus, while gender-referred boys may be accepted by female peers, there is likely still a significant amount of ostracism experienced from same-sex peers. Zucker (2005c) conjectured that peer ostracism may also contribute to the above noted relationship between age and behavior problems in children with GID as older children with marked cross-gender behavior may experience relatively more social ostracism compared to younger children who engage in similar behaviors (see Zucker, Wilson-Smith, Kurita, & Stern, 1995).
In recent years, a new line of clinical research has suggested that some children with GID may have comorbid Pervasive Developmental Disorder (PDD), particularly Asperger’s Disorder (e.g., de Vries, Noens, Cohen-Kettenis, van Berckelaer-Onnes, & Doreleijers, 2010; Landén & Rasmussen, 1997; Mukkades, 2002; Zucker et al., 2012b). One explanation for a possible linkage between these two relatively rare disorders is the intense focus/obsessional interest in specific activities (e.g., Klin, Danovitch, Merz, & Volkmar, 2007). Postema et al. (2011) examined two items on the CBCL which measure obsessions (Item 9: “Can’t get his/her mind over certain thoughts; obsession”) and compulsions (Item 66: “Repeats certain acts over and over; compulsions”) in 528 gender referred children (435 boys, 93 girls) and 414 siblings (239 boys, 175 girls). Items are scored based on the past 6 months on a 0-2 scale where 0 = not true, 1 = somewhat or sometimes true, and 2 = very true or often true. For Item 9, 61.5% of gender-referred boys received a score of 1 or 2, compared to 27.3% of their male siblings, and 49% of referred boys in the CBCL standardization sample (Achenbach, 1991). For Item 66, 26.2% of gender referred boys received a score of 1 or 2, compared to 10.5% of their male siblings, and 26% of referred boys in the CBCL standardization sample. For both Items 9 and 66, the comparison between gender-referred boys and their siblings was significant. These preliminary results support the idea that boys with GID (and, generally, children with GID) show an apparent elevation in obsessional interests, which may be one reason for the observed comorbidity of GID and PDD. For the gender-referred boys, gender-related themes constituted more than half (54.6%) of the examples provided by their mothers.
In summary, children with GID display significantly more behavior problems compared to their siblings and non-referred children but typically display as many behavior problems as other clinical populations, with older children with GID having more behavior problems than younger children. Boys with GID typically present with more internalizing than externalizing difficulties, such as separation anxiety. Furthermore, gender-referred children, boys in particular, have poor peer relations and this was postulated to mediate the relationship between cross-gender behavior and behavior problems. The role of peer relations in the lives of children with GID is emphasized by the fact that, for some clinicians, a primary goal of treatment for gender-referred children is to prevent social ostracism and improve peer relations (Zucker & Bradley, 1995).
1.10.1.2 Comorbidity in Children with GID
Over 25 years ago, Coates and Person (1985) found that, in 25 boys (M age, 7.4 years) who met criteria for GID, 15 (60%) also met criteria for separation anxiety disorder (SAD). Coates and Person did not provide details on how they assessed for the presence of SAD, beyond a general statement that DSM-III criteria were used nor did they provide data on inter-rater reliability. A decade later, Zucker, Bradley, and Lowry Sullivan (1996b) examined the relationship between GID and SAD in 115 boys (M age, 6.3 years), of whom 73 (63.5%) met the full diagnostic criteria for GID and the remaining 42 (36.5%) were subthreshold for the diagnosis. To assess the presence of SAD, Zucker et al. developed a 21-item parent-report interview based on the DSM-III diagnostic criteria. The items assessed nine content domains which reflected the DSM-III criteria for SAD. Questions were phrased such that they could be answered by mothers as “Yes,” “Sometimes,” or “No.” Zucker et al. used conservative and liberal criteria to assign a diagnosis of SAD that differed in terms of the frequency of the symptoms reported. A conservative diagnosis was given if the mother answered “Yes” to questions in three of the nine content domains. A liberal diagnosis was given if the mother answered “Yes” or “Sometimes” in three of the nine content domains. Using the conservative criterion for SAD, there was no significant association between the presence of GID and SAD. A significant association existed when the liberal criterion was used. Of the 73 boys who meet full criteria for GID, 47 (64.4%) also met the criteria for SAD. In contrast, only 16 (38.1%) of the 42 boys who were subthreshold for the diagnosis of GID also met criteria for SAD.
A limitation of Coates and Person’s (1985) and Zucker et al.’s (1996) study is that neither included a group of clinical control participants referred for reasons other than GID. Nonetheless, the rates of SAD obtained in these studies are higher than the prevalence rates of SAD in children (for a review, see Masi, Mucci, & Milliepedi, 2005) and suggests that SAD may be overrepresented in boys with GID.
A recent line of research has led some authors to conclude that elevated levels of separation anxiety in childhood may be a component of the more general pattern of childhood femininity seen in some homosexual men (for a review, see VanderLaan, Gothreau, Bartlett, & Vasey, 2011a). Using a retrospective design, VanderLaan, Gothreau, Bartlett, and Vasey (2011b) found that homosexual men recalled, on average, significantly higher levels of separation anxiety compared to heterosexual men but similar to those of women. For the homosexual men but not heterosexual men, increases in recalled childhood femininity were associated with increases in separation anxiety. There is also cross-cultural support for this finding. Vasey, VanderLaan, Gothreau, and Bartlett (2011) found that Samoan fa’afafine recalled significantly more childhood separation anxiety compared to Samoan women and (heterosexual) men. These results raise the question of whether boys with GID who develop a homosexual sexual orientation would have experienced more separation anxiety in childhood compared to those who develop a heterosexual sexual orientation. None of the prospective studies on boys with GID have specifically examined this.
Researchers in The Netherlands systematically assessed the prevalence of DSM diagnoses in children with GID using a structured parent-report interview (Wallien, Swaab, & Cohen-Kettenis, 2007). Wallien et al. compared 120 children referred to a specialized gender identity clinic and diagnosed with GID (86 boys, 34 girls; age range, 4-11 years) to 47 children (37 boys, 10 girls) referred to an ADHD clinic and who served as a clinical control group. Of the 120 children with GID, 62 (51.6%) met criteria for a DSM diagnosis other than GID. There was no significant difference between the GID and ADHD children on number and type of comorbid diagnoses. Of the 86 GID boys, 48 (55.8%) met criteria for a diagnosis other than GID. Of these, more than half (n = 26, 56.1%) met criteria for an anxiety disorder (mostly specific phobia), 22 (25.5%) met criteria for a disruptive disorder (e.g., oppositional defiant disorder), and 4 (4.7%) met criteria for a mood disorder. In contrast to the studies by Coates and Person (1985) and Zucker et al. (1996b), only 5 (5.8%) of boys with GID met criteria for SAD.
The above described associated psychopathology in children with GID can be understood in several ways. First, as noted earlier, it may be the result of social ostracism (Zucker, 2005c). Second, it has been shown that behavior problems in gender-referred children may be significantly associated with measures of parental psychopathology and this may reflect generic familial vulnerability to psychopathology (Zucker & Bradley, 1995; Zucker et al., 2003). Third, associated psychopathology in children with GID may be implicated in the etiology of GID and, therefore, may contribute to its genesis (Coates & Person, 1985; Zucker et al., 2012b). Regardless of the mechanisms underlying the relationship between childhood cross-gender behavior and general behavior problems in gender-referred children, it raises the question of whether the associated psychopathology in childhood is related to long-term psychosexual and psychiatric outcomes, a question the present study will attempt to address.
1.10.2 Adolescents and Adults with GID
CBCL data suggest that adolescents with GID have significantly higher levels of behavioral problems (e.g., Internalizing T score) and poorer peer relations compared to children with GID (Zucker, Owen, Bradley, & Ameeriar, 2002). As discussed earlier, this “age effect” could represent a proxy for social ostracism (i.e., youth with gender identity issues encounter more problems in their social relationships as they age). Similar to that observed in children with GID, gender-referred adolescents are as likely to have as many behavior problems and similar peer relations as other clinically referred adolescents (i.e., referred for reasons other than gender) and to have considerably more behavioral problems and poorer peer relations than nonreferred adolescents (Zucker et al., 2012b; for a review, see Zucker, 2006c).
The presence of comorbid psychiatric diagnoses in adolescents with GID is an extremely important clinical issue as it can influence decisions regarding treatment recommendations (Cohen-Kettenis, Delemarre-van de Waal, & Gooren, 2008; Zucker et al., 2011). Only one study has systematically examined comorbidity of DSM diagnoses in adolescents with GID. Using a structured parent-report interview, de Vries, Doreleijers, Steensma, and Cohen-Kettenis (2011b) examined the presence of DSM diagnoses (other than GID) in 105 gender referred adolescents (53 males, 52 females; M age at assessment, 14.6 years). Of the 105 adolescents, 32.4% met criteria for at least one DSM diagnosis other than GID, which is lower than the obtained prevalence rate of comorbid diagnoses of 52% seen in children with GID (see Wallien et al., 2008). These results are, therefore, in contrast to studies showing more problem behaviors in adolescents compared to children. For the entire sample, the most common disorders were social phobia (9.5%) and major depression (8.6%). The presence of comorbid diagnoses did not vary according to GID diagnosis (i.e., full criteria versus sub-threshold). Of the 53 boys in the study, 39.6% met criteria for at least one concurrent disorder. Social phobia, major depression, and oppositional defiant disorder were the most common diagnoses. Further, the biological males in this study were at increased odds of having a mood or anxiety disorder compared to the natal females. de Vries et al. suggested that perhaps natal males with GID show patterns of psychopathology most typically associated with their desired gender (i.e., females). The most prominent limitation of this study was that parents, not the adolescent themselves, were the informants. This might have resulted in an underestimate of some diagnoses, such as alcohol or substance abuse and, by extension, an underestimate of the prevalence of comorbid diagnoses in adolescents with GID.
Comorbidity with other Axis I psychiatric disorders have been examined in adults with GID. The rates obtained have varied across studies. Cole, O’Boyle, Emory, and Meyer (1997) relied on historical information to assess comorbidity in 318 male-to-female transsexuals seen in a gender identity clinic. Only 6% of the patients reported a history of treatment for an Axis I disorder other than substance use or GID. The most common comorbid diagnosis was major depression. Other studies have used unstructured and semi-structured interviews to assess for other psychiatric conditions and these have typically founds higher rates of comorbidity. In some studies, data were reported for male-to-females and females-to-males combined. Bodlund and Armelius (1994) reported that 44% of a mixed group of male-to-female and female-to-male had another Axis I diagnosis other than GID. Haraldsen and Dahl (2000) reported similar results: in a mixed group of male-to-female and female-to-male transsexuals that included both pre-operative (i.e., applied for sex reassignment surgery) and post-operative patients (i.e., completed sex reassignment surgery), 33% met criteria for another Axis I diagnosis. De Cuypere, Jannes, and Rubens (1995) reported a lower rate of comorbidity. Only 23% of the male-to-female patients in their study met criteria for another Axis I disorder. In a recent study of adult patients with GID in Japan, Hoshiai et al. (2010) reported that 18% of the male-to-female patients had another Axis I diagnosis. Across these studies, the most common comorbid diagnoses were a mood or anxiety disorder. Hoshiai et al. reported that 76% if the male-to-female patients reported a lifetime history of suicidal ideation. De Cuypere, Jannes, and Rubens (1995) and Verschoor and Poortinga (1988) reported high rates of lifetime suicide attempt in their samples of male-to-female patients, 54% and 19% respectively.
Prevalence estimates of comorbid substance use in male-to-female adults with GID have varied. None of the male-to-female patients in Hoshiai et al.’s (2010) study had comorbid substance-related disorders. In contrast, Cole et al. (1997), Hepp, Kraemer, Schnyder, Miller & Delsignore (2005), and De Cuypere et al. (1995) reported fairly high lifetime prevalence figures of substance abuse in the male-to-female patients: 29%, 50%, and 50%, respectively.
De Cuypere et al. (1995) reported personality disorders in 70% of the male-to-female patients in their sample. Most other studies, however, have found lower rates of comorbid Axis II disorders. For example, Hepp et al. (2005), Bodlund and Armelius (1994), and Haraldsen and Dahl (2000) reported prevalence rates of 42%, 33%, and 20% respectively. Of note, these latter studies reported on mixed groups of male-to-female and female-to-male patients. With the exception of De Cuypere et al.’s study, these rates are similar to those seen in other clinical populations but higher than in nonclinical populations (e.g., Newton-Howes et al., 2010; Zimmerman, Rothschild, & Chelminski, 2005).
1.10.3 Suicidality and Victimization in Transgendered Populations
Even among youth unselected for their gender identity, the presence of gender atypical behavior appears to be associated with poorer well being (Rieger & Savin-Williams, 2012) and places these youth at higher risk for victimization compared to gender-typical youth. Thus, transgender youth are particularly vulnerable to victimization because of their atypical gender role presentation (for a discussion, see Stieglitz, 2010). Nuttbrock et al. (2010) found that 50.1% of male-to-female transgendered adults (from a sample of 517) experienced physical abuse while 78.1% experienced verbal abuse that was related to their gender identity/gender role. In an earlier study, Grossman, D’Augelli, and Salter (2006) found that 87% of male-to-female transgendered youth had experienced some type of victimization. These percentages appear to be higher than the estimated victimization rates for youth in North America of 50%-62% (e.g., Kilpatrick, Saunders, & Smith, 2002; Romano, Bell, & Billette, 2011; Saunders, 2003).
A number of population-based studies have found that transgendered youth/adults may be at an increased risk for suicide attempts compared to youth in the general population (for a review, see Haas et al., 2011). It has been estimated that 3.13%-4.6% of adults in the United States have made at least one suicide attempt (Kessler, Borges, & Walters, 1999; Weissman et al., 1999). In staggering contrast, studies of community samples of youth who self-label as transgendered have found that approximately 30-40% have made at least one suicide attempt (Clements-Nolle, Marx, & Katz, 2006; Grossman & D’Augelli, 2007; Maugen & Shipherd, 2010).
Transgendered individuals may be at even greater risk for suicide ideation and attempts than homosexual males (Mathy, 2003) and this may be directly related to discrimination and victimization pertaining to their gender atypical behaviors (Clements-Nolle et al., 2006; Nuttbrock et al. 2010). Given that the majority of boys with GID later develop a homosexual sexual orientation with desistence of GID, it has been suggested that they may share some of the same risk factors that have been identified in gay and lesbian adolescents, including stigmatization, rejection by the peer group, discrimination, and mental health difficulties (see e.g., D’Augelli, 2002; Lombardi, Wilchins, Priesing, & Malfouf, 2001; Mathy, 2003; Meyer, 2003; Morrow, 2004; Sandfort, Bakker, Schellevis, & Vanwesenbeeck, 2006; Savin-Williams & Ream, 2003). A large body of evidence, including well conducted epidemiological studies indicates that individuals from sexual minority populations are at an increased risk for various mental health difficulties, most notably depression, suicide, anxiety, and substance use, compared to their heterosexual counterparts (Cochran, 2001; Cochran & Mays, 2000; Cochran, Sullivan, & Mays, 2003; D’Augelli, 2002; Faulkner & Cranston, 1998; Ferguson, Horwood, & Beautrais, 1999; Gilman et al. 2001; King et al., 2008; Meyer, 2003; Remafedi, French, Story, Resnick, & Blum, 1998), with prevalence rates of suicide attempts ranging from 23% to 42% (D’Augelli & Hershberger, 1993; D’Augelli, Hershberger, & Pilkington, 1998, 2001; Safren & Heimberg, 1999; for a review, see McDaniel, Purcell, & D’Augelli, 2001). Furthermore, studies have found that the increased risk for suicide attempts among sexual minority youth is maintained even after controlling for substance abuse and other psychiatric comorbidity, such as depression (e.g., Herrell et al., 1999). That an association exists between homosexuality and mental health risk is now generally accepted (see meta-analysis by King et al., 2008).
1.11 A Conceptual Framework for the Present Study
The extent to which childhood behavior is predictive of behavior in adulthood has been a central question in the field of developmental psychology. Historically, researchers took a retrospective approach to examining the relationship between adult and child psychopathology. The major methodological limitation with retrospective studies, however, pertains to possible distortions in memory in recalling childhood symptoms or behavior (e.g., Verhulst, 1995). This limitation, combined with the increased recognition that some childhood problems continued into adulthood while others did not, argued for a prospective approach (Achenbach, 1997) and resulted in a wave of prospective studies which examined the developmental course of psychopathology in children.
Prospective studies of children with a particular disorder have found that some children continue to have the same disorder in adolescence and adulthood. Other children, however, show a desistence of the disorder from childhood to adolescence and, therefore, demonstrate discontinuity of the disorder over time (Maughan & Rutter, 2008). Thus, children with the same diagnosis in childhood can have multiple outcomes in adolescence and adulthood, which is commonly referred to as multifinality (Cicchetti & Rogosch, 1996). A longitudinal approach is necessary if one is to understand both continuities and discontinuities in psychopathology over time (Verhulst & Koot, 1991).
These developmental psychopathology concepts are particularly relevant to any prospective follow-up studies of boys with GID. The extant literature on boys with GID indicates that most grow up to feel comfortable with their biological sex and show a desistence of GID. Of the boys who show desistence of GID, most develop a homosexual sexual orientation and a minority develops a heterosexual sexual orientation. Thus, it appears that only a minority of boys with GID show persistence of the disorder into adolescence and adulthood. Therefore, within a group of boys with GID, discontinuity of the disorder from childhood to adolescence appears to be the most common developmental trajectory; however, there are multiple long-term outcomes for boys with GID. To understand this finding, it is necessary to conduct within-group analyses (McNeil & Kaij, 1979) to identify childhood factors that can predict outcome in adolescence and adulthood (e.g., with regard to persistent GID vs. desistent GID). Further, the percentage of children with GID who show persistent gender dysphoria into adolescence and adulthood is higher than the estimated prevalence rate of GID in the general population. Children with GID, then, can be conceptualized as “high-risk” for GID in adulthood when compared to children without GID.
The present study can be conceptualized as a within-group comparison of a group of children “at risk” for GID to develop an understanding of the childhood factors that can predict the various observed outcomes. Four decades ago, Green (1970) recognized that the developmental picture leading to “transsexualism” in adulthood can only be clearly understood by conducting longitudinal research. On understanding the development of adult transsexualism, Green wrote, “One way is to study a group of young children who would appear to be of high risk with respect to later manifestation of anomalous sexual and gender behavior, and to study their families. Most adults who request sex reassignment report difficulties in adopting appropriate gender-typic behavior during childhood (p. 271).”
Several studies using prospective designs have been conducted to examine predictors of outcome in children with other psychiatric disorders, including schizophrenia (Werry & McCleenan, 1991), bipolar disorder (Geller, Fox, & Clark, 1993; Werry, McClellan, & Chard, 1991), attention deficit-hyperactivity disorder (Dalsgaard, Mortensen, Frydenberg, & Thomsen, 2002), conduct disorder (see Robins, 1966), and pervasive developmental disorders (Szatmari, Bryson, Boyle, Streiner, & Duku, 2003). Notably, in adults with antisocial disorder, a similar disjunction between retrospective and prospective studies as observed in GID is also found: severely antisocial adults were antisocial children; however, only about half of antisocial/ conduct disordered children grow up to become antisocial adults (for a review, see Maughan & Rutter, 2008). Longitudinal studies have also been conducted on children identified as “at-risk” for developing schizophrenia later in life, with the goal of identifying predictors of within-group outcome (i.e., development of schizophrenia versus no schizophrenia later in life) (Erlenmeyer-Kimling et al., 1997; Neale & Weintraub, 1975;). These studies have suggested attempts to predict outcome should include demographic, psychosocial, and psychological factors.
1.11.1 Rationale for the Present Study
There are several reasons why a systematic examination of the long-term outcome of boys with GID is urgently needed, with both theoretical and clinical implications. The follow-up studies on boys with GID have focused predominantly on examining outcome vis-à-vis gender identity and sexual orientation. At present, very little is known about the long-term psychiatric functioning among boys with GID.
Although a large majority of boys with GID no longer have the disorder in adulthood, there is variation in the rates of persistence obtained in follow-up studies. Additional follow-up studies are needed to better clarify what proportion of boys may persist in having the disorder in adolescence and adulthood. Further, there are very limited data on childhood characteristics that may differentiate persisters from desisters. For example, it appears that children with more severe cross-gender identification are more likely to show persistence of GID compared to children who are less severe (Wallien & Cohen-Kettenis, 2008). However, other childhood factors may also contribute to the developmental course of GID. None of the follow-up studies to date have systematically conducted an evaluation of childhood demographic, psychosocial, and psychological variables and their role in the persistence and desistence of GID. Green (1970) stated, “The developmental picture leading to adult transsexualism remains smudgy” (p. 271). Four decades later, the picture is still “smudgy.”
The identification of predictors of GID outcome also carries clinical implications. In children with GID who appear to be on a trajectory for GID in adolescence and adulthood, intervention efforts can attempt to steer them away from a transsexual outcome onto one in which comfort with one’s biological sex is the outcome. The rationale for such an intervention is the observed complexity of embarking on a life course of cross-sex hormonal and surgical treatment combined with the pervasive social discrimination and victimization that many people with gender dysphoria encounter (Zucker, Drummond, Bradley, & Peterson-Badali, 2009). Green (2008), more directly, expressed that living as a homosexual adult is generally easier than living as a transsexual. Some clinicians have argued for early recognition of children who may persist in their gender dysphoria, but from a different standpoint. If a clinician is certain that a child with GID is committed to a pathway leading to transsexualism (i.e., persisting GID), interventions with gonadotropin releasing hormone (GnRH) blockers (commonly referred to as “puberty blockers”) could be used to delay the onset of puberty (Wallien & Cohen-Kettenis, 2008).
It is also clinically relevant to examine childhood factors that may predict outcome with regard to psychological functioning in adolescence and adulthood. If it were possible to identify children who may be at risk for developing psychiatric problems in adulthood, treatment can also focus on reducing the risk for psychopathology. In the field of developmental psychopathology, in general, the identification of predictors of change in psychopathology has been regarded theoretically important for advancing our knowledge of the development of psychopathology and as clinically relevant for informing treatment guidelines (Mathijssen, Koot, & Verhulst, 1999).
The present study is also urgently needed given the intense controversy in the field regarding best treatment practice for children with GID. While some parents seek therapeutic support that helps their child feel more comfortable with a gender identity that matches the child’s birth sex, a more extreme group of parents, and some therapists, actively promote an early social transition in the child, sometimes as young as preschool (Zucker et al., 2009). Unfortunately, there are no comparative data on the effects of these treatment approaches on long-term psychosexual and psychological outcome of children with GID. Given that the follow-up studies conducted thus far have found that most children with GID show a desistence, treatment approaches, particularly those that espouse early transitioning, need to be evaluated. Although the present study does not include an evaluation of therapeutics, data on persistence, desistence, and the factors that can predict outcome may, in the interim, inform treatment approaches.
Beyond the contextual importance of this study, the strong methodological design warrants specific mention. This present study differs from previous follow-up studies in several ways. First, the number of boys in our sample was considerably larger than the sample sizes of its predecessors. Second, I have extensive assessment data on psychological functioning in childhood and at follow-up. Third, at follow-up, cross-informant data (via parent-report) on psychological functioning and gender role are available. Fourth, the present study includes a measure of social desirability, which is a particularly important construct to measure in studies that examine gender identity and sexual orientation.
1.11.2 Goals of the Present Study
The first goal of the study was to provide descriptive data on the long-term outcome of boys with GID with regard to four possible outcomes: (1) persistence of gender dysphoria with a bisexual/homosexual sexual orientation, (2) persistence of gender dysphoria with a heterosexual sexual orientation, (3) desistence of GID with a bisexual/homosexual sexual orientation, and (4) desistence of GID with a heterosexual sexual orientation.
The second goal of the study was to provide descriptive data on the long-term psychiatric outcomes of boys with GID in terms of DSM psychiatric diagnoses and general behavior problems, both for the overall group of boys and according to their psychosexual outcome.
The third goal of the study was to identify childhood factors which can predict outcome at follow-up with regard to gender identity and sexual orientation. This included a systematic examination of demographic, psychological, and psychosocial variables as potential predictors of outcome.
The fourth goal of the study was to provide preliminary data on adult victimization experiences of boys with GID and its relationship to their psychiatric functioning.
Chapter 2
Method
The participants were biological males who had been referred to and then assessed in the Gender Identity Service, Child, Youth, and Family Program at the Centre for Addiction and Mental Health (CAMH) in Toronto, Ontario during their childhood and were adolescents or adults at the time of follow-up. Data collection occurred over three decades, 1986-2011 (Table 1).
Participants entered the follow-up study through two methods of recruitment. Most participants were recruited through routine contact for research follow-up. From 1986-2011, there were two main waves of participant recruitment through research contact, from 1986-1993 and, more recently, from 2009-2011.[15] In addition, during the period of data collection, some adolescents who had been assessed in the clinic during childhood contacted the service for clinical reasons (e.g., persistent gender dysphoria, emerging sexual identity, or other clinical issues). These participants were informed about the opportunity to participate in the follow-up study and subsequently completed the study protocol. The majority of the patient-initiated participants had contacted the clinic between the two main waves of research recruitment. Thus, from 1994-2008, the participants who entered the study were primarily those who had contacted the service for clinical reasons. As such, the final study sample consisted of participants who entered the study through standard research contact or following participant-initiated involvement with the clinic.
|
Table 1 |
|
|
|
|
Distribution of Recruitment Across Data Collection Period |
|||
|
|
|
Method of Study Entry |
|
|
Year |
Number of participants recruited |
Research |
Clinical |
|
1986 |
8 |
8 |
0 |
|
1987 |
7 |
7 |
0 |
|
1988 |
8 |
8 |
0 |
|
1989 |
3 |
3 |
0 |
|
1990 |
4 |
4 |
0 |
|
1991 |
4 |
4 |
0 |
|
1992 |
0 |
0 |
0 |
|
1993 |
3 |
3 |
0 |
|
1994 |
0 |
0 |
0 |
|
1995 |
2 |
1 |
1 |
|
1996 |
0 |
0 |
0 |
|
1997 |
1 |
0 |
1 |
|
1998 |
2 |
1 |
1 |
|
1999 |
0 |
0 |
0 |
|
2000 |
2 |
0 |
2 |
|
2001 |
1 |
0 |
1 |
|
2002 |
6 |
2 |
4 |
|
2003 |
5 |
1 |
4 |
|
2004 |
3 |
0 |
3 |
|
2005 |
3 |
1 |
2 |
|
2006 |
2 |
1 |
1 |
|
2007 |
2 |
0 |
2 |
|
2008 |
2 |
0 |
2 |
|
2009 |
40 |
36 |
4 |
|
2010 |
25 |
23 |
2 |
|
2011 |
6 |
4 |
2 |
2.1.1 Routine Contact for Research
A chart review was conducted of all boys (range, 3-12 years) assessed in the Gender
Identity Clinic Service at the CAMH since 1975 to identify eligible participants. Between 1975
and 2009, the clinic evaluated 463 boys referred for gender identity issues. To participate in the follow-up study, patients from this sample had to be at least 16 years of age. Using this cut-off,
the chart review identified 294 eligible participants, of which contact was attempted in 132 cases. For the remaining 162 cases, contact was not attempted due to lack of study resources and time constraints.
Of the 132 cases where contact was attempted, 19 (14.3%) potential participants could not be reached/traced through previous addresses, registrars, and personal contacts (e.g., the patient and/or family had moved and a current telephone number, mailing address, or e-mail could not be identified). Initial telephone contact was first made with the parents because participants were minors at the time of the childhood assessment and may have had no recollection of their clinic attendance (see Appendix C for phone script). In general, the response from parents and participants was positive. Of the 113 patients where contact was successful, 79 (69.9%) agreed to complete the study protocol and came into the clinic for a face-to-face assessment. In 28 (24.8%) cases, some follow-up data on gender identity and sexual orientation were provided over the phone by the parents or the patients themselves or were obtained through a chart review. For a variety of reasons, these 28 participants did not complete the standard follow-up assessment (e.g., geographic limitations, too busy). Appendix D summarizes the information acquired during a telephone conversation with the parent of a follow-up participant and serves as an exemplar of the information provided by parents, and which was used as the basis for group classification at follow-up. In the remaining 6 (5.3%) cases, either the parents did not allow us to speak to their now grown up child or the potential participant himself declined to participate in the study. In total, 107 participants entered the study through routine research recruitment.
2.1.2 Participant-Initiated Clinical Contact
An additional 32 participants were recruited into the study after they had contacted the Gender Identity Service for clinical reasons. In 7 cases, either the participant or the parents contacted the clinic due to persistent gender dysphoria. In 6 cases, the clinic was contacted because either the participant or the parent was concerned about sexual orientation and in 1 case there was concern about gender dysphoria and sexual orientation. Lastly, in the remaining 18 cases, the participants or parents contacted the clinic for other heterogeneous clinical concerns, including depression, substance abuse, parent-child conflict, and conduct problems. Appendix E lists the reasons for contacting the clinic for each of the 32 participants.
Some of the participants who contacted the clinic were younger than 16 years of age. It is important to note that all participants were aware that completing the follow-up study was voluntary and a decision to decline participation in the study would not have affected their involvement with the clinic. Of these 32 participants, 31 completed the standard follow-up protocol and 1 participant provided some data on gender identity and sexual orientation but did not complete the formal study.[16]
2.1.3 Participation Rate
In total, 145 participants were approached about participating in the follow-up study, either through routine contact (n = 113) or following their clinical involvement with the Gender Identity Service (n = 32). Six participants declined, which yielded a participation rate of 95.9%.
2.1.4 Demographic Characteristics of Participants
The demographic characteristics of the participants in childhood and at follow-up are shown in Table 2. The GID diagnosis in childhood was based on the DSM (3rd ed. [DSM-III]; 3rd ed., rev. [DSM-III-R]; or 4th ed. [DSM-IV]; American Psychiatric Association [APA], 1980, 1987, and 1994, respectively) criteria applicable at the time of assessment. A total of 88 (63.3%) boys met complete DSM criteria for GID in childhood. The remaining 51 (36.7%) boys were subthreshold for a DSM diagnosis, but all had some indicators of GID, and, based on the historical information provided during the assessment, some would have met the complete DSM criteria at some point in their lives prior to their assessment in childhood.
The mean age of assessment in childhood was 7.49 years (SD = 2.66; range, 3.33-12.99) and the mean age at follow-up was 20.58 (SD = 5.22; range, 13.07-39.15). The mean time interval between childhood assessment and follow-up was 12.88 years (SD = 6.07; range, 2.77-29.29).
The study was approved by the Institutional Review Boards at the CAMH and the University of Toronto. The majority of participants who completed the face-to-face assessment were evaluated on a single day. Three participants were seen twice. In these instances, the participants completed the self-report measures during their second visit as the complexity of their clinical presentation extended the duration of the assessment. Participants were provided a
Table 2 |
||||
|
Demographic Characteristics (N = 139) |
||||
|
Characteristic |
M |
SD |
Range |
% |
|
From childhood |
|
|
|
|
|
Age (in years) |
7.49 |
2.66 |
3.33-12.99 |
|
|
Year of birth |
1981.87 |
7.50 |
1966-1996 |
|
|
Year of assessment |
1989.36 |
7.50 |
1975.42-2004.84 |
|
|
IQa |
105.93 |
15.47 |
69-138 |
|
|
Social Classb |
40.74 |
15.15 |
8.0-66.0 |
|
|
Marital Statusc |
|
|
|
|
|
Two-parent family |
|
|
|
64.7 |
|
Other |
|
|
|
35.3 |
|
Caucasian |
|
|
|
84.9 |
|
At follow-up |
|
|
|
|
|
Age (in years) |
20.58 |
5.22 |
13.07-39.15 |
|
|
Follow-up interval (in years)d |
12.88 |
6.07 |
2.77-29.29 |
|
|
IQa,e,f |
105.88 |
16.03 |
65-138 |
|
|
aFull-Scale IQ was obtained with age-appropriate Wechsler intelligence scales. bHollingshead’s (1975) Four Factor Index of Social Status (absolute range: 8-66), which is based on educational level and occupation. cOther included the following family constellations: single parent, separated, divorced, living with relatives, or in the care of a child protection agency. dInterval denotes the time between childhood assessment and follow-up assessment. eFull Scale IQ estimated using four subtests: Vocabulary, Comprehension, Block Design and Object Assembly. fIQ were only available for participants who completed the face-to-face assessment. Of these, scores were not available for 1 participant. |
||||
stipend for their participation in the follow-up assessment and reimbursement for travel expenses.
All participants who completed the face-to-face assessment gave written informed consent prior to their involvement in the follow-up assessment (see Appendix F). Participants were explained their right to participate, their right to withdraw at any time during the study, and assured anonymity. Concerns about emotional distress (e.g., endorsement of suicidality in the psychiatric interview) were addressed; although no participants required acute immediate care, there were instances in which intervention or clinical care was required. The majority of the follow-up procedures were conducted by the author of this thesis (n = 71) under the supervision of Dr. Kenneth Zucker. However, for participants assessed prior to 2009, the study procedures were carried out by Dr. Kenneth Zucker (n = 68).
Participants who completed the face-to-face interview responded positively to the assessment process. With one exception, rapport with the participants appeared to be good. At the time of follow-up, two participants were currently being seen in our clinic for therapy.
2.3.1 Childhood Assessment
2.3.1.1 Cognitive Functioning
Based on the age of clients at the time of assessment, the appropriate version of the Wechsler Intelligence Scale for Children was administered (WISC-R, WISC-III, WISC-IV or the WPPSI-R).[17] Full scale IQ scores were used to characterize level of cognitive functioning.
2.3.1.2 Sex-typed Behavior
A variety of methods and measures were used to assess sex-typed behavior in childhood (i.e., gender identity and gender role), which are summarized in Table 3. A total of five child informant and two parent informant measures were used to assess the participants’ sex-typed behavior in childhood: (1) Draw-a-Person test (Zucker, Finegan, Doering, & Bradley, 1983); (2) a free-play task (Zucker, Doering, Bradley, & Finegan, 1982); (3) the Playmate and Playstyle Preferences Structured Interview (Fridell, Owen-Anderson, Johnson, Bradley, & Zucker, 2006); (4) sex-typed responses on the Rorschach test (Zucker, Lozinksi, Bradley & Doering, 1993); (5) the Gender Identity Interview for Children (Wallien et al., 2009; Zucker et al., 1993); (6) The Gender Identity Questionnaire for Children (Johnson et al., 2004); and (7) a measure of activity
Table 3 Measures of Gender Identity and Gender Role in Childhood |
|||
|
Measure |
Informant |
Mode |
Description of Variables |
|
Draw-a-Person (Jolles, 1952 ; Zucker, Finegan, Doering, & Bradley 1983)
|
Child |
Test |
Sex of first drawn person. |
|
Free-play task (Reckers & Yates, 1976; Zucker, Doering, Bradley & Finegan, 1982)
|
Child |
Observation |
Difference between cross-sex and same-sex play. Positive score indicates more cross-sex play. |
|
Rorschach inkblot test (Zucker, Lozinski, Bradley, & Doering, 1992) |
Child |
Test |
Difference between number of same-sex and cross-sex responses. A higher score indicates more cross-sex than same-sex responses.
|
|
Gender Identity Interview (Wallien et al., 2009; Zucker et al., 1993)
|
Child |
Interview |
Semi-structured gender identity interview schedule with questions that establish gender dysphoric feelings and confusion one’s gender status. Higher scores reflect more gender-atypical responses.
|
|
Playmate and Playstyle Preferences Structured Interview (Alexander & Hines, 1994; Fridell, Owen-Anderson, Johnson, Bradley, & Zucker, 2006)
|
Child |
Test |
Yields two scores: cross-sex peer preference and cross-sex play preference. A higher score indicates more cross-sex playmate/peer choices. |
|
Gender Identity Questionnaire for Children (Johnson et al., 2004; Zucker et al., 2003)
|
Parent |
Questionnaire |
Higher scores reflect more cross-gendered behavior. |
|
Temperament: Activity Level/Extraversion (Zucker & Bradley, 1995 pp. 189-193) |
Parent |
Questionnaire |
Higher ratings indicate elevated activity levels and more rough-and-tumble play. |
|
Note. With the exception of Draw-a-Person, which is a categorical variable, variables based on other measures of childhood sex-typed behavior are continuous. |
|||
level/extraversion (Zucker & Bradley, 1995). Some of these measures have been designed to assess gender identity constructs or a child’s general discomfort with his or her gender status, as well as gender role behaviors (e.g., toy preferences, fantasy play). Other measures assess well-established normative gender differences for dimensions of temperament that included ratings of activity level and involvement in rough-and-tumble play (see review in Zucker, 2005b).
2.3.1.3 Behavior Problems
The Child Behavior Checklist (CBCL; Achenbach, 1991; Achenbach & Edelbrock, 1983) was completed by a parent or guardian during the child’s initial assessment. This measure is a standardized parent-report questionnaire for ratings of behavior problems in children 4 to 18 years of age. It consists of 118 behavior problems that are rated on a 3-point scale (0 = not true, 1 = sometimes true or somewhat true, 2 = very true or often true). The questionnaire identifies two “broad-band” factors, “Internalizing” and “Externalizing,” that assess dimensions of child psychopathology. Internalizing disorders are described as covert emotional disturbances (e.g., depression, social withdrawal, anxiety) and the Externalizing disorders are described as disorders of overt conduct (e.g., aggression, hyperactivity). Parent ratings on the CBCL yield T scores for Total, Internalizing, and Externalizing problems. Reports indicate extensive evidence for the reliability and validity of the CBCL as an index of behavioral psychopathology in clinical and nonclinical populations (Achenbach, 1985, 1991; Achenbach & Edelbrock, 1983; Achenbach, McConaughy, & Howell, 1987). The intra-class correlations for individual items were more than .90. Test-retest reliability over a one-week period was .89, and inter-parent agreement for total behavior problem scores was .66. Furthermore, the long-term stability estimates for total behavior problem scores over 3-, 6-, and 18-month periods were .74, .60, and .46, respectively (Achenbach & Edelbrock, 1983). The CBCL discriminates well between children referred to mental health agencies from demographically-matched non-referred children (Achenbach & Edelbrock, 1983).
2.3.1.4 Peer Relations
Zucker, Bradley, and Sanikhani (1997) constructed a three-item Peer Relations Scale derived from the CBCL using Items 25, (“Doesn’t get along with other kids”), 38 (“Gets teased a lot”), and 48, (“Not liked by other kids”). Based on maternal ratings on the CBCL, both boys and girls with GID had poorer peer relations than did their siblings. Cronbach’s alpha was .81 and the mother-father correlation for the scale was .66 (n = 312, p < .001). The Peer Relations Scale was subsequently used in comparative study of children and adolescents with GID (Zucker, Owen, Bradley, & Ameeriar, 2002) where it was the strongest predictor of behavioral psychopathology on the CBCL for both children and adolescents. Cohen-Kettenis et al. (2003) used the Peer Relations Scale in a cross-clinic study in which children with gender identity issues seen at the Gender Identity Service at the CAMH were compared to children with gender identity issues seen at the Gender Clinic housed within the Department of Child and Adolescent Psychiatry at the University Medical Center Utrecht (The Netherlands) on demographic characteristics, social competence, and behavior problems. Across both clinics, boys with gender identity issues had poorer peer relations than did girls.
2.3.2 Follow-up Assessment
Table 4 summarizes the follow-up assessment protocol. The gender identity and sexual orientation measures, along with self-report measures of behavior problems, are used as part of the current standardized clinical assessment of adolescents referred to the Gender Identity Service (Zucker, 2005b; Zucker et al., 2012b; Zucker & Bradley, 1995). The victimization and suicidality questionnaires were novel to this follow-up evaluation, as was the standardized interview schedule to assess the presence of DSM psychiatric disorders.
All interviews were conducted in a private office. The follow-up assessment protocol was administered in the following order to all participants: (a) cognitive testing, (b) psychiatric diagnostic interview, (c) semi-structured clinical interview, and (d) self-report questionnaires. The semi-structured clinical interview consisted of four parts: (a) the participant’s current functioning (e.g., family, school, and work), (b) recollections of and thoughts about the childhood assessment and childhood gender role/gender identity, (c) current gender identity, and (d) sexual orientation in fantasy and behavior. The semi-structured interview always preceded the self-report questionnaires and was audiotaped, except in one instance where the participant did not give consent. The self-report questionnaires provided an immediate cross-check of the interview and served additional quantitative purposes. The contents of the follow-up assessment are described below.
2.3.2.1 Cognitive Functioning
Four subtests from the age-appropriate version of the Wechsler Intelligence Scales were administered (Vocabulary, Comprehension, Block Design, and Object Assembly). The scaled scores from these subtests were used to provide an estimated IQ score for cognitive functioning (Sattler, 2001). Data collection occurred over a period of 24 years. During this time, the Wechsler Intelligence Scales underwent revisions and the most recent version at the time of assessment was used for cognitive testing. As a result, over the period of data collection, several versions of the Wechsler scales were used. Participants 17 years or older were administered the Wechsler Adult Intelligence Scale-Revised (n = 8; WAIS-R; Wechsler, 1981), the Wechsler Adult Intelligence Scale-Third Edition (n = 16; WAIS-III;
|
Table 4 |
|
|
Variable |
Measure |
|
Cognitive Functioning |
Selected subtests from the WAIS-III, WAIS-IV, WISC-III, or WISC-IV |
|
Psychiatric and Behavioral Functioning |
Diagnostic Interview for Children and Adolescents (Herjanic & Reich, 1982) or Diagnostic Interview Schedule-Version III-A (Robins & Helzer, 1985) Parent report: Child Behavior Checklist (Achenbach, 1991) or Adult Behavior Checklist (Achenbach & Rescorla, 2003) Self report: Youth Self-Report Scale (Achenbach & Edelbrock, 1983) or Young Adult Self-Report Scale (Achenbach, 1997) or Adult Self Report Scale (Achenbach and Rescorla, 2003)
|
|
Childhood Gender Identity and Gender Role Behaviors |
Recalled Childhood Gender Identity/Gender Role Questionnaire (Zucker et al., 2006)
|
|
Current Gender Identity and Gender Role Behaviors |
Self Report : 1) Gender Identity Questionnaire for Adolescents and Adults (Deogracias et al., 2005; Singh et al., 2010) or Gender Dysphoira Questionniare ( Zucker et al., 1996) 2) Semi-structured interview for Gender Identity Disorder (Appendix G) Parent Report: 3) Gender Identity/Gender Role Questionnaire for Adolescents (Zucker, Bradley, Owen-Anderson, & Singh, 2010)
|
|
Sexual Orientation in Fantasy (past 12 months) |
Kinsey Ratings (Kinsey et al., 1948) Erotic Response and Orientation Scale (Storms, 1980)
|
|
Sexual Orientation in Behavior (past 12 months) |
Kinsey Ratings (Kinsey et al., 1948) Sexual History Questionnaire (Langevin, 1985)
|
|
Social Desirability |
Marlowe-Crowne Social Desirability Scale (Crowne & Marlowe, 1960)
|
|
Victimization Experiences |
Victimization Survey (Drummond, 2006)
|
|
Suicidality |
Suicidality Questionnaire (Drummond, 2006) |
|
Note. WAIS-III = Wechsler Adult Intelligence Scale-Third Edition; WAIS-IV = Wechsler Adult Intelligence Scale-Fourth Edition; WISC-III = Wechsler Intelligence Scale for Children-Third Edition; WISC-IV = Wechsler Intelligence Scale for Children-Fourth Edition. |
|
Wechsler, 1997) or the Wechsler Adult Intelligence Scale-Fourth Edition (n = 32; WAIS-IV; Wechsler, 2008). Participants under the age of 17 were administered either the Wechsler Intelligence Scale for Children-Revised (n = 25; WISC-R; Wechsler, 1974), the Wechsler Intelligence Scale for Children-Third Edition (n = 16; WISC-III; Wechsler, 1991), or the Wechsler Intelligence Scale for Children-Fourth Edition (n = 12; WISC-IV, Wechsler, 2003).
2.3.2.2 Behavioral Functioning
For participants younger than 19 years, the Youth Self-Report (YSR; Achenbach, 1991) was used to assess behavior and emotional problems. For participants 19 years and older, the Young Adult Self-Report (YASR; Achenbach, 1997) or the Adult Self-Report (ASR; Achenbach & Rescorla, 2003) was used. T scores for Internalizing, Externalizing, and Total Behavior Problems were derived for each participant. The YSR is a 103 item self-report questionnaire that assesses emotional and behavior problems for ages 11 to 18 years. The YASR, the predecessor of the Adult Self-Report, contains 119 items to measure psychopathology in individuals 18 to 30 years. The YASR was utilized in data collection until the ASR was published. The ASR contains 126 items to measure psychopathology for individuals aged 18 to 59 years. The YSR, YASR, and ASR are variations of the CBCL and have the same 3-point format (0 = not true, 1 = sometimes true or somewhat true, 2 = very true or often true). The YSR has been reported to have good reliability and validity for identifying adolescent behavior problems (Achenbach, 1997). Several studies have used these scales to examine the course and predictive value of self-reported problems among adolescents and adults (Hofstra, van der Ende, & Verhulst, 2000, 2001).
Although assessment of adult psychopathology relies extensively on self-report, meta-analyses of studies comparing self-report and an informant’s report revealed moderate correlations between cross-informant data for substance abuse, internalizing, and externalizing problems (Achenbach, Krukowski, Dumenci, & Ivanaova, 2005). Participants gave permission to have their parent/guardian or spouse/partner complete the Child Behavior Checklist (CBCL; Achenbach, 1991) for those participants less than 18 years or the Adult Behavior Checklist (ABCL; Achenbach & Rescorla, 2003) for participants 18 years or older. Forms were given to those parents or guardians that came to the clinic with the participant or sent by mail to those that did not accompany the participant. T scores for Internalizing, Externalizing, and Total Behavior Problems were derived from the informant forms. Of the 110 participants who completed the follow-up assessment, parent report data were missing for 16 participants, either because the adult participants did not give consent to have their parents complete questionnaires or the parents did not return the questionnaires.
2.3.2.3 Psychiatric Functioning
Selected modules of the Diagnostic Interview for Children and Adolescents (DICA; Herjanic & Reich, 1982) or the Diagnostic Interview Schedule (DIS, Version IIIA; Robins, Helzer, Croughan, & Ratcliffe, 1981) were administered depending on age at follow-up. Participants younger than 18 were administered the DICA (n = 64) and those 18 years or older were administered the DIS (n = 44). Psychiatric data were not available for two of the 110 participants who completed the face-to-face assessment.
The DICA is a semi-structured psychiatric interview for youth between 6 and 17 years to assess the presence or absence of psychiatric diagnoses based on the third edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-III, American Psychiatric Association, 1980). The DICA was patterned after the DIS. Ten DICA modules were included in this study: (1) Oppositional Disorder, (2) Conduct Disorder (Aggressive and Non-aggressive), (3) Alcohol Abuse and Alcohol Dependence, (4) Major Depression, (5) Adjustment Disorder with Depressed Mood, (6) Mania, (7) Separation Anxiety, (8) Overanxious Disorder, (9) Marijuana Abuse, and (10) Other Drug Abuse and Drug Dependence. The total number of possible diagnoses a participant could meet criteria for on this measure was 13. The DICA has been demonstrated to have good reliability (Welner et al., 1987) and adequate validity (Carlson et al.1987; Ezpeleta et al., 1997).
The DIS is a standardized structured interview devised to assess the presence or absence of psychiatric diagnoses in adults based on the DSM-III (American Psychiatric Association, 1980). Fourteen modules were included in this study: (1) Depression (Major Depression [single episode], Major Depression [recurrent], Grief Reaction), (2) Dysthymic Disorder, (3) Obsessive-Compulsive Disorder, (4) Agoraphobia, (5) Social Phobia, (6) Simple Phobia, (7) Panic Disorder, (8) Agoraphobia with Panic Attacks, (9) Generalized Anxiety Disorder, (10) Alcohol Abuse and Alcohol Dependence, (11) Drug Abuse and Drug Dependence, (12) Anorexia Nervosa and Bulimia, (13) Schizophrenia, and (14) Bipolar Disorder . The total number of possible diagnoses a participant could meet criteria for on this measure was 17. The DIS has been found to have excellent inter-rater reliability (Anduaga, Forteza, & Lira, 1991; Hesselbrock et al., 1982). There have been some concerns about the validity of the DIS (e.g., Helzer et al., 1985) as studies have yielded mixed results with kappas ranging from low to moderate (for review, see Rogers, 2001). Following the publication of the DSM-IV, the Diagnostic Interview Schedule for DSM-IV (DIS-IV) was published (Robins, Cottler, Bucholz, & Compton, 1995) to correspond to the updated DSM diagnostic criteria. Test-retest reliability and validity of the DIS-IV was assessed in a sample of drug users (Dascalu, Compton, Horton, & Cottler, 2001; Horton, Compton, & Cotter, 1998). Test-retest reliability and validity ranged from excellent to fair for most disorders. However, test-retest reliability was considered poor for generalized anxiety disorder and specific phobia, kappa = .35 and .25, respectively (for more details on specific diagnoses, see Compton & Cottler, 2004).
For the DIS and the DICA, the total number of diagnoses each participant met criteria for was calculated.
2.3.2.4 Psychosexual Variables
The present study examined seven self-report measures of psychosexual outcome and one parent-report measure pertaining to sex-typed behavior.
2.3.2.4.1 Recalled Childhood Gender Identity and Gender Role Behaviors
Participants completed the Recalled Childhood Gender Identity/Gender Role Questionnaire (Zucker et al., 2006). This questionnaire consists of 23 items pertaining to various aspects of childhood sex-typed behavior and identification (e.g., peer preferences, toy preferences, roles in fantasy play, and feelings about being a male as a child), as well as relative closeness to mother and father during childhood. Items were rated on a 4-point or 5-point scale. For some items, however, an additional response option allowed the participant to indicate that the behavior did not apply (e.g., for the question about favorite playmates, there was the option “I did not play with other children”). Each participant was instructed to make ratings for their behavior as a child (“between the years 0 to 12”). Factor analysis identified two factors, accounting for 37.4% and 7.8% of the variance, respectively (all factor loadings ≥ .40). Factor 1 consisted of 18 items that pertained to childhood gender role and gender identity and Factor 2 consisted of three items that pertained to parent-child relations (relative closeness to one’s mother vs. father). Significant variation in factor scores between groups completing the RCGI was reported (e.g., heterosexual versus homosexual adults, adolescents with GID versus transvestic fetishism, women with CAH versus their sisters or female cousins), demonstrating that the questionnaire has good discriminant validity (Singh et al., 2010; Zucker et al., 1996a, 2006). For the present study, this questionnaire was used as a measure of recalled gender role and gender identity behaviors and, as such, the mean Factor 1 score was computed for each participant. Lower scores represent more recalled childhood cross-gender behaviors. The RCGI was added to the assessment protocol in 1993, after data collection had begun, so some data were missing for individuals who completed the follow-up prior to the inclusion of this measure.
2.3.2.4.2 Concurrent Gender Identity
Concurrent gender identity was evaluated using interview and self-report data. During an audiotaped interview, each participant was asked to describe their current feelings about being a biological male. They were also asked to describe positive and negative aspects about their gender identity. For example, participants who reported a “male” gender identity were asked to describe positive and negative aspects of being male. Participants were also administered a semi-structured gender identity interview (see Appendix G) based on the adolescent and adult GID criteria outlined in the DSM-IV-TR (American Psychiatric Association, 2000). The interview contained five questions related to the Point A criteria (e.g., the stated desire to be a woman, passing as a woman, the desire to live or be treated as a woman) and four questions from the Point B criteria (e.g., a preoccupation with getting rid of their penis, belief that they should have been born a woman). Participants were asked to respond to these questions according to the last 12 months with No, Sometimes, or Yes.
Two self-report measures were also used to assess current gender identity and gender dysphoria: (a) The Gender Identity/Gender Dysphoria Questionnaire for Adolescents and Adults (GIQAA; Deogracias et al., 2007; Singh et al., 2010), or (b) the Gender Dysphoria Questionnaire (GDQ; Zucker et al., 1996a). The GDQ was developed prior to the GIQAA. As such, the GIQAA was introduced to the clinical battery subsequent to the GDQ and, as a result, the more recent participants were administered the GIQAA while earlier participants were given the GDQ. The GIQAA and GDQ differ in number of items and rating scale. They also differ in the wording of questions. In order to integrate the data collected from the GIQAA and GDQ, participants’ score on each measure was converted to a proportion score which ranged from 0-1. The proportion score, referred to hereafter as the gender dysphoria score, was used in all analyses instead of the mean scores on the GIQAA and GDQ. The gender dysphoria score reflects the proportion of the highest possible score that each participant received on either the GIQAA or the GDQ. For example, a participant with a proportion score of 1.00 on either the GIQAA or GDQ received the maximum score on that measure. A higher proportion score indicates more gender dysphoria. There were, however, some participants who completed the GIQAA and the GDQ (n = 17). In these cases, the GIQAA proportion score was used as it is a more psychometrically sophisticated measure of gender dysphoria compared to the GDQ.
The male version of the GIQAA (Deogracias et al., 2007; Singh et al., 2010) was completed. This 27-item questionnaire measures gender identity and gender dysphoria in adolescents or adults; participants over the age of 17 completed the adult version and younger participants completed the adolescent version. The adolescent and adult versions are identical in all regards except that, in the adult version, the words “man” and “woman” are used instead of “boy” and “girl.” The items were developed by the North American Task Force on Intersexuality (NATFI) Research Protocol Working Group (S. J. Kessler, H. F. L. Meyer-Bahlburg, J. M. Schober, and K. J. Zucker) based on prior measures, expert panels, and clinical experience, and were designed to capture multiple indicators of gender identity and gender dysphoria, including subjective (n = 13 items), social (n = 9 items), somatic (n = 3 items), and sociolegal (n = 2 items) parameters. Each item was rated on a 5-point response scale from Never (coded as 1) to Always (coded as 5) based on a time frame of the past 12 months. Item examples include the following: “In the past 12 months, have you felt unhappy about being a man?” and “In the past 12 months, have you had the wish or desire to be a woman?” Principal axis factor analysis identified a one-factor solution that accounted for 61.3% of the variance. All factor loadings were ³ .30 (median, .86; range, .34-.96). The GIQAA demonstrated evidence for discriminant validity and a high threshold for specificity (i.e., low false positive rate for non-GID individuals).
In a replication and extension of this study, Singh et al. (2010) compared adults and adolescents with GID to clinical controls (i.e., evaluated for reasons other than GID or transvestic fetishism). There was strong evidence for discriminant and convergent validity, with high sensitivity and specificity rates. Males and females with GID reported significantly more gender dysphoria than clinical controls, with large effect sizes (Cohen, 1988). Deogracias et al. (2007) suggested that the mean score on the Gender Identity Questionnaire for Adolescents and Adults (GIQAA) can be used to determine whether a participant was gender dysphoric, and, in their sample, used a mean score of ≤ 3[18] to indicate a “case” of gender dysphoria. Using this criterion for caseness, the measure was able to identify gender dysphoric adolescents with 93.3% sensitivity. For the clinical control participants, specificity (i.e., low false positive rate for non-GID individuals) was 100% (i.e., none of the clinical control participants met criteria for caseness). For adults, sensitivity was 87.8% for the GID participants and specificity was 100% for the clinical controls. In a subsequent study, Singh, McMain, and Zucker (2011) administered the GIQAA to 100 women diagnosed with borderline personality disorder (BPD), none of whom were ever evaluated in a gender clinic. Using the suggested GIQAA mean score of 3 as the cut-off for identifying gender dysphoria, none of the women with BPD met this criterion for caseness. Zucker et al. (2010) reported on 105 adolescent males with GID, of whom, 91.7% met criterion for caseness. Additional psychometric evidence for discriminant validity and clinical utility can also be found in Singh et al. (2011).
The Gender Dysphoria Questionnaire (Zucker et al., 1996a) contains 8 items pertaining to gender identity and gender dysphoria. Each item was rated on a 3-point or 5-point scale based on a time frame of the past 6 months. Item examples include the following: “In the past 6 months, how often have you wished that you had been a born a girl instead of a boy?” (with response options ranging from “never” to “a lot”) and “In the past 6 months, how have you felt about being a boy?” (with response options ranging from “very satisfied” to “very dissatisfied”). Factor analysis identified two factors, accounting for 31.4% and 12.5% of the variance, respectively (all factor loadings ≥ .45). Factor 1 consisted of 5 items pertaining to gender dysphoria and Factor 2 consisted of 3 items pertaining to gender role identification. For the present study, the mean Factor 1 score was computed for each participant.
Using the questionnaire data on concurrent gender identity, participants were classified as either gender dysphoric (“persisters”) or not gender dysphoric (“desisters”) at follow-up. The Results section outlines the specific criteria used to make this classification.
2.3.2.4.3 Concurrent Gender Role–Parent Report
The Gender Identity/Gender Role Questionnaire for Adolescents (GIGRQ-Ad) is a 13-item parent-report questionnaire pertaining to various aspects of concurrent sex-typed behavior (e.g., sex-of-peer affiliation preference, masculine vs. feminine interests, cross-dressing, the desire to be of the other sex; Zucker, Bradley, Owen-Anderson, & Singh, 2010b). Items were rated on a 5-point response scale, with the exception of a Peer Composite item, in which a difference score between the number of male and female friends was calculated. Factor analysis of the GIGRQ-Ad was based on a sample of 403 youth, including various comparison groups, such as siblings and clinical controls. A principal axis factor analysis identified a one-factor solution, accounting for 44.8% of the variance. Ten of the 14 items had factor loadings >.43 (range, .43-.82) and, for these items, a unit-weighted mean total score was derived. Cronbach’s alpha for this measure was .91. A lower score indicates more cross-gender behavior. Discriminant validity was reported in Zucker et al. (2010b).
2.3.2.4.4 Sexual Orientation
As stated previously, in sexology research sexual orientation is often measured using two metrics: sexual orientation in fantasy and sexual orientation in (overt) behavior (Green, 1987). For the present study, participants’ sexual orientation in fantasy and behavior was assessed using a multi-method approach: face-to-face interview and self-report. Participants’ sexual orientation was classified in relation to their biological (birth) sex.
2.3.2.4.4.1 Sexual Orientation in Fantasy
Each participant’s sexual orientation in fantasy was assessed with specific questions from an audiotaped face-to-face interview and the self-report Erotic Response and Orientation Scale (EROS; Storms, 1980).
Questions posed in the audiotaped interview asked about four types of sexual fantasy: (1) crushes on other people; (2) sexual arousal to visual stimuli (e.g., strangers, acquaintances, partners, and individuals presented in the media [video, movies, magazines, internet]; (3) sexual content of night dreams; and (4) sexual content of masturbation fantasies. During the interview, participants were not asked directly about the gender of the person or persons who elicited sexual arousal, thus allowing time for the participant to provide this information spontaneously. Directed questions about the gender of the person(s) who elicited sexual arousal were asked only if the participant did not volunteer specific information about whether their arousal was directed to same-sex or opposite-sex partners, or both. By the end of the interview, each participant provided information about sexual arousal to both same-sex and opposite-sex individuals. Using the Kinsey scale criteria (Kinsey, Pomeroy, & Martin, 1948), the interviewer assigned Kinsey ratings that ranged from 0 (exclusively heterosexual in fantasy) to 6 (exclusively homosexual in fantasy) for each question.[19] A dummy score of 7 denoted that the participant did not experience or report any fantasies. A global fantasy score was also derived based on ratings from the four questions. In the present study, only ratings for the last 12 months are reported since one goal of the study was to assess sexual orientation at the time of follow-up. During the interview, however, participants were asked about their “lifetime” (i.e., from age 13 until present) history of sexual fantasies. Kinsey ratings for sexual orientation in fantasy were available for 129 participants.
Inter-rater reliability on Kinsey ratings for sexual orientation in fantasy was examined for 29 participants, which were selected at random. The second scorer listened to the audio recordings of the semi-structured interview, with specific attention to the information collected on sexual orientation. The second coder was masked to participants’ group status at follow-up. The inter-rater agreement on the Kinsey Global Fantasy rating was very good (kappa = .95). For reference purposes, Appendix H lists the inter-rater agreement for each type of sexual fantasy evaluated during the semi-structured interview.
The Erotic Response and Orientation Scale (EROS) is a 16-item self-report measure assessing sexual orientation in fantasy over the past 12 months. Half of the questions pertained to heterosexual fantasy (e.g., “How often have you noticed you had sexual feelings (even the slightest) while looking at a woman?”) and the other half pertained to homosexual fantasy (e.g., “How often have you noticed you had sexual feelings (even the slightest) while looking at a man?”). Each item was rated on a 5-point scale for frequency of occurrence, ranging from “none” to “almost every day.” Mean homoerotic and heteroerotic fantasy scores were derived for each participant. Previous use of the EROS has shown good evidence of discriminant validity, such that it is able to discriminate between responses of self-identified heterosexual and homosexual men and women (Storms, 1980; Zucker et al., 1996a).
2.3.2.4.4.2 Sexual Orientation in Behavior
Each participant’s sexual orientation in behavior was assessed with specific questions
during the face-to-face interview and with a modified version of the Sexual History
Questionnaire (SHQ; Langevin, 1985).
In the interview, questions asked about five types of sexual behavior: (a) dating; (b) holding hands in a romantic manner; (c) kissing; (d) genital fondling or touching a woman on the breasts, and (e) intercourse (penile-vaginal and anal). Kinsey ratings for behavior in the past 12 months were made in the same manner as fantasy ratings.
Inter-rater reliability on Kinsey ratings for sexual orientation in behavior was examined for 29 participants, which were selected at random. The second scorer listened to the audio recordings of the semi-structured interview, with specific attention to the information collected on sexual orientation. The second coder was masked to participants’ group status at follow-up. There was perfect inter-rater agreement on the Kinsey Global Behavior rating (kappa = 1.0). For reference purposes, Appendix H lists the inter-rater agreement for each type of sexual behavior evaluated during the semi-structured interview.
The modified Sexual History Questionnaire (SHQ) consists of 20 questions. Ten questions pertained to heterosexual experiences (e.g., “How many women have you kissed on the lips in a romantic way?”) and 10 questions pertained to homosexual experiences (e.g., “How many men have you kissed on the lips in a romantic way?”). Participants who were 18 years and older completed the adult version and younger participants completed the adolescent version. The adolescent and adult versions are similar in all regard except that, in the adult version, the words “man” and “woman” are used instead of “boy” and “girl.” Each item was rated on a 5-point scale for frequency of occurrence, ranging from none to 11 or more, based on a time frame of the past 12 months. Mean total scores for heterosexual and homosexual experiences were derived.
2.3.2.4.4.3 Sexual Orientation Group Classification
On the basis of Kinsey ratings, participants who completed the face-to-face interview were classified into the following three sexual orientation groups for both fantasy and behavior: (1) heterosexual (Kinsey global ratings of 0-1); (2) bisexual/homosexual (Kinsey global ratings of 2-6), and (3) no sexual fantasy or behavior. Participants’ sexual orientation was classified in relation to their birth sex.
A comment is warranted on the decision to combine the bisexual and homosexual participants. This validity of this procedure has been questioned (e.g., MacDonald, 1983; Paul, 1993) on the basis that combining bisexuals with homosexuals in research samples, though standard among sex researchers, confounds the research on both groups. In the present study, and similar to Green’s (1987) follow-up study, participants who were categorized as bisexual or homosexual on the basis of their Kinsey ratings were combined for a number of reasons. On the basis of extensive clinical experience, Zucker and Bradley (1995) stated that it is common for homosexual men to recall a period of bisexual behavior during adolescence. It is, therefore, conceivable that some adolescent participants who reported bisexual behavior and/or fantasies will move toward an exclusively homosexual sexual orientation in adulthood. Research on sexual identity development has demonstrated that men who adopt a homosexual identity might go through a stage in which they identify as bisexual (e.g., Lever, 1994; Stokes, Damon, & McKirnan, 1997). Recent research on the sexual arousal patters of men who identify as bisexual has found that most were more strongly aroused by homosexual stimuli than by heterosexual stimuli and, therefore, appear to be homosexual with respect to their genital arousal (Rieger, Chivers, & Bailey, 2005). Moreover, decades of research on “coming out” as gay or homosexual has shown that the period of first disclosure can range from during mid-adolescence, around 16 or 17 years of age (e.g., D’Augelli, Hershberger, & Pilkington, 1998; Grov, Bimbi, Nanin, & Parson, 2006) to late adolescence and early 20s (e.g., McDonald, 1982; Savin-Williams, 1998; Savin-Williams & Ream, 2003) and depends on numerous factors, including ethnicity, relationship with parents and their anticipated reaction, and person to whom the individual is disclosing–individuals with same-sex attractions typically come out to a supportive friend before coming out to parents (Beaty, 1999; Savin-Williams & Dube, 1998). Finally, it was not a goal of the present study to embark on a comparison of exclusively homosexual versus bisexual participants.
2.3.2.5 Social Desirability
Social desirability refers to the desire to cast a favorable impression on others. It can threaten the validity of self-report scales if in answering questions respondents seek social approval or try to represent themselves in a favorable manner (King & Brunner, 2000; Tan & Grace, 2008). People scoring high on social desirability tend to provide socially acceptable answers regardless if their response accurately describes them. As such, researchers have recognized that, particularly when assessing attributes of a personal or sensitive nature, such as an individual’s sexual history, the respondents’ propensity to give socially desirable responses should be measured (e.g., Wallien & Cohen-Kettenis, 2008). Participants 18 years and older were given the Marlow-Crowne Social Desirability Scale (M-CSDS; Crowne & Marlowe, 1960), which consists of 33 true-false items. The scale consists of 18 culturally acceptable but unlikely statements keyed in the true direction and 15 socially undesirable but probable statements keyed in the false direction for a maximum possible score of 33. Participants 17 years and under, were given a shorter version of the M-CSDS (Strahan & Gerbasi, 1972), containing 20 items that consists of 12 culturally acceptable but improbable statements keyed in the true direction and 8 socially undesirable but probable statements keyed in the false direction for a maximum possible score of 20. For the present study, the percentage of endorsed socially desirable items was calculated for each participant. In order to integrate the data from both versions of the M-CSDS, participants’ percentage score on each measure was converted to a proportion score which ranged from 0-1, which was used in all analyses. A higher proportion score indicates a greater propensity to give socially desirable responses. Several studies have found that the MCSDS is a reliable and valid measure of social desirability (Crowne & Marlowe, 1960; Holden & Feeken, 1989; Silverthorn & Gekoski, 1995).
2.3.2.6 Suicidality Experiences
Suicidal experiences were assessed with a Suicidality Questionnaire (see Appendix I) that consists of 13 items derived from Centre for Disease Control and Prevention Survey on Youth Risk Behavior Surveillance System (Brener et al., 2002; CDC, 2002) and questionnaires given in other studies (D’Augelli et al., 2002; Savin-Williams & Ream, 2003). Six of the questions pertained to “lifetime” experiences (since the age of 13) and 7 pertain to suicidal thoughts and/or experiences within the past 12 months. Frequencies of suicidality experiences were derived. Participants’ responses on this questionnaire were reviewed before they left the clinic. A procedure was set in place such that participants who expressed suicidal thoughts would be asked additional questions as part of a risk assessment; however, none of the study participants were at imminent risk for suicide. The Suicidality Questionnaire was introduced to the study protocol after data collection had begun; therefore, some participants did not complete this measure. In these instances, data on suicidality were extracted from their psychiatric interview (i.e., the Diagnostic Interview Schedule or the Diagnostic Interview for Children and Adolescents).
2.3.2.7 Victimization Experiences
Victimization experiences were assessed through a 12-item Victimization Survey (see Appendix J), which was adapted from previous studies on sexual orientation victimization of lesbian and gay youth and adults (D’Augelli et al., 2002; D’Augelli & Grossman, 2001; Herek, Gillis, Cogan, & Glunt, 1997). The survey was modified to target victimization due to cross-gender behavior. Questions ask participants’ frequency of victimization experiences over the past 12 months and since the age of 13 (i.e., “lifetime” victimization experiences). Seven types of victimization experiences were asked, including three verbal and four physical types. Verbal victimization included: (a) verbal insults, (b) threats of violence, and (c) threats by other to disclose gender identity. Physical victimization consisted of: (a) objects being thrown at the individual, (b) physical assault (e.g., being punched, kicked, or beaten), (c) threat of an attack, using a knife, gun, or weapon, and (d) sexual assault. Participants responded to each question based on the frequency of occurrence for each type of victimization with 0 = “Never,” 1 = “Once,” 2 = “Twice,” and 3 = “Three or more times.” An average verbal victimization score, an averge physical victimization score, and an average total victimization score was computed (the sum of all items divided by the relevant number of items) for ratings based on lifetime experiences as well as the past 12 months (D’Augelli, Pilkington, & Hershberger, 2002). Participants were also asked about the location of their victimization experiences (e.g., home, school, neighborhood, work place) and the type of relationship they had with the assaulter (e.g., parent, sibling, significant other, peer, or stranger). The Victimization Survey was added to the assessment protocol in 2008, after data collection had begun, so data were missing for individuals who completed the follow-up prior to the inclusion of this measure.
Chapter 3
Results
3.1 Participants vs. Non-Participants
The non-participants represent three groups: (1) patients who were eligible to participate in the study but were not contacted (n = 163), (2) patients who declined to participate in the study (n = 6), and (3) patients who were not successfully traced (n = 19). Two sets of analyses were conducted to compare the study participants with the non-participants. First, the study participants were compared to the boys who were eligible but were not contacted for research follow-up. Second, the study participants were compared to those who refused to participate in the study and to those where contact was attempted but the families were not successfully traced. Group comparisons were conducted on demographic variables (age at assessment, IQ, social class, marital status, ethnicity), CBCL behavior problems (Internalizing T score, Externalizing T score, Total T score), and nine measures of childhood sex-typed behavior.
Table 5 shows the childhood assessment data (demographics and CBCL behavior problem ratings) of the 139 boys who participated in the study compared to the 163 boys who were eligible to participate but were not contacted due to time constraints and lack of study resources. There were no significant differences between the participants and non-participants on the demographic variables of age at assessment, social class, ethnicity or marital status (ps > .05). However, the comparison on childhood IQ was significant, t(289)[20] = 2.01, p = .046, with the participants having a higher IQ than the non-participants. The effect size for this comparison was small (unpooled d = .22). With regard to parent-report of behavior problems on the CBCL, there were no significant differences between the
|
Table 5 |
|||||||||
|
Demographic Characteristics and Behavior Problems as a Function of Participant Status |
|||||||||
|
|
Participants (n = 139) |
Non-Participantsa (n = 163) |
χ2 |
p |
|||||
|
Demographic Characteristics |
|||||||||
|
Marital Status of Parents |
|
|
|
|
|||||
|
Two-Parent |
90 (64.7) |
109 (66.9) |
<1 |
ns |
|||||
|
Otherb |
49 (35.3) |
54 (33.1) |
|
|
|||||
|
|
|
|
|
|
|
|
|||
|
Ethnicity |
|
|
|
|
|
|
|||
|
Caucasian |
118 (84.9) |
136 (83.4) |
<1 |
ns |
|||||
|
Non-Caucasian |
21 (15.1) |
27 (16.6) |
|
|
|||||
|
|
|
|
|
|
|
|
|||
|
|
M |
SD |
M |
SD |
t |
p |
|||
|
Age at Assessment |
7.49 |
2.66 |
7.03 |
2.30 |
1.59 |
ns |
|||
|
Social Class |
40.74 |
15.15 |
43.05 |
14.48 |
-1.35 |
ns |
|||
|
IQc |
105.93 |
15.47 |
102.11 |
16.88 |
2.01 |
.046 |
|||
|
|
|
|
|
|
|
|
|||
|
Behavioral Problems |
|||||||||
|
Internalizing T Score |
62.20 |
9.86 |
62.19 |
11.35 |
<1 |
ns |
|||
|
Externalizing T Score |
60.86 |
10.93 |
61.29 |
12.14 |
<1 |
ns |
|||
|
Total T Score |
62.77 |
11.38 |
62.70 |
12.79 |
<1 |
ns |
|||
|
aBoys who were eligible to participate but were not contacted. b“Other” includes single parent, separated, divorced, living with relatives. cAge appropriate version of the Wechsler Intelligence Scale was administered. |
|||||||||
participants and non-participants on Internalizing problems, Externalizing problems, and Total problems (ps > .05). The participants and non-participants were also compared on their diagnosis in childhood and their scores on measures of sex-typed behavior (Table 6). There was no significant difference between the participants and non-participants in terms of
whether they were diagnosed with GID in childhood or were subthreshold for the diagnosis, χ2(1) < 1. There were also no significant differences between the participants and non-participants on any of the eight measures of sex-typed behavior (ps > .05). In sum, of the 17 analyses conducted to examine the differences between the participants and those who were eligible to participate but were not contacted, only one comparison (childhood IQ) was
|
Table 6 |
||||||||||
|
Childhood Sex-Typed Behavior as a Function of Participant Status |
||||||||||
|
|
Participants (n = 139) |
Non-Participants (n = 163) |
|
|
||||||
|
|
N |
% |
N |
% |
χ2 |
p |
||||
|
DSM Diagnosisa N (%) |
|
|
|
|
|
|
||||
|
Threshold for GID |
88 |
63.3 |
105 |
64.4 |
<1 |
ns |
||||
|
Subthreshold for GID |
51 |
36.7 |
58 |
35.6 |
|
|
||||
|
|
|
|
|
|
|
|
||||
|
Draw-a-Person |
|
|
|
|
|
|
||||
|
Same-Sex |
63 |
45.7 |
67 |
44.7 |
<1 |
ns |
||||
|
Cross-Sex |
75 |
54.3 |
83 |
55.3 |
|
|
||||
|
|
|
|
|
|
|
|
|
|
||
|
|
M |
SD |
N |
M |
SD |
N |
t |
p |
||
|
Child measures |
||||||||||
|
Free Play Taskb |
.11 |
.64 |
121 |
.09 |
.58 |
146 |
<1 |
ns |
||
|
|
|
|
|
|
|
|
|
|
||
|
Rorschach Difference Scorec |
.57 |
3.74 |
125 |
.72 |
3.83 |
78 |
<1 |
ns |
||
|
|
|
|
|
|
|
|
|
|
||
|
Gender Identity Interviewd |
6.31 |
5.82 |
85 |
6.03 |
5.52 |
145 |
<1 |
ns |
||
|
|
|
|
|
|
|
|
|
|
||
|
Playmate and Playstyle Preferences Structured Interview: Cross-sex peer playe |
8.44 |
5.37 |
41 |
8.48 |
5.23 |
108 |
<1 |
ns |
||
|
|
|
|
|
|
|
|
|
|
||
|
Playmate and Playstyle Preferences Structured Interview: Cross-sex toy playf |
7.07 |
2.99 |
41 |
6.90 |
2.97 |
108 |
<1 |
ns |
||
|
|
|
|
|
|
|
|
|
|
||
|
Parent measures |
||||||||||
|
Gender Identity Questionnaire for Childreng |
2.86 |
.66 |
97 |
2.90 |
.59 |
149 |
<1 |
ns |
||
|
|
|
|
|
|
|
|
|
|
||
|
Temperament: Activity Levelh |
3.05 |
.53 |
136 |
3.09 |
.61 |
151 |
<1 |
ns |
||
|
aFor diagnosis, GID means that the patient met complete DSM-III, DSM-IIIR, or DSM-IV criteria for GID. bDifference between cross-sex and same-sex play during a free-play task. Positive score indicates more cross-sex play. cDifference between number of same-sex and cross-sex responses. Positive score indicates more cross-sex responses. dAbsolute range, 0-24. A higher score reflects more gender identity confusion. eAbsolute range, 0-14. A higher score indicates more cross-sex playmate/peer choices. fAbsolute range, 0-14. A higher score indicates more cross-sex toy choices. gAbsolute range, 1-5. A lower score indicates more cross-gender behavior. h Higher ratings indicate elevated activity levels and more rough-and-tumble play. |
||||||||||
significant.
Using one-way ANOVA or chi-square, the study participants were also compared to the 6 cases where either the parents or the potential participant himself refused to participate and to the 19 cases where the families could not be traced. Group comparisons were conducted on demographic variables, CBCL behavior problems, and measure of sex-typed behavior. There were no significant group differences on the demographic variables of age, social class, and ethnicity (ps > .05). The ANOVA on childhood IQ approached significance, F(2, 162) = 2.99, p = .053. Duncan’s multiple range test for unequal Ns showed that the participants did not differ significantly from the other two groups; however, the non-participants who refused had a higher IQ in childhood than those who could not be traced. The three groups differed significantly on marital status, χ2(2, N = 164) = 9.02, p = .011. Post-hoc analyses were done using chi-square or Fisher’s Exact Test. The participants did not differ significantly from the non-participants who refused; however, they differed significantly from the cases that could not be traced, χ2(1, N = 158) = 6.39, p = .012. The participants were more likely to have originated within a two-parent household while those who could not be traced were more likely to have come from a family composition other than two-parent (e.g., single parent, living with relatives). The comparison between the non-participants who refused and those who could not be traced approached significance (p = .056, Fisher’s exact test). Again, the non-participants who could not be traced were more likely to have come from a family composition that was not two-parent. With regard to parent-report of behavior problems on the CBCL, there were no significant differences between the three groups on Internalizing problems, Externalizing problems, and Total problems (ps > .05). The three groups were also compared on their diagnosis in childhood and on measures of sex-typed behavior. There was no significant difference between the three groups on their diagnosis in childhood; the participants were as likely to have met full diagnostic criteria for GID as the non-participants. There were also no significant group differences on any of the measures of sex-typed behavior (ps > .05). In sum, of the 17 analyses conducted to compare the participants to those who refused and to those who could not be traced, one (marital status) was significant and one (childhood IQ) approached significance. The other 15 group comparisons were not significant.
3.2 DSM Diagnosis for Gender Identity Disorder in Childhood
Of the 139 participants, 88 (63.3%) met diagnostic criteria for GID in childhood and the remaining 51 (36.7%) were subthreshold for the diagnosis. These two groups were compared on demographic variables, CBCL behavior problems, and measures of sex-typed behavior. There were no significant group differences on the demographic variables of IQ in childhood, marital status or ethnicity (ps > .05). However, the threshold participants were significantly younger in age at the time of the childhood assessment, t(108) = -6.31, p < .001, and originated within a family of higher social status compared to the subthreshold participants, t(108) = 2.31, p = .023. The effect size for these differences was medium, .34 and .46, respectively.
3.2.1 Childhood Behavior Problems as a Function of Diagnostic Status for Gender Identity Disorder
One-way ANCOVAs, with age and social class covaried, were conducted to evaluate whether the two diagnostic groups differed on CBCL behavior problems and sex-typed behavior in childhood. There were no significant differences between the threshold and subthreshold participants on Internalizing T score and Total T score (both ps > .05). The subthreshold participants were rated by their parents as having, on average, significantly more externalizing difficulties (M = 61.02, SD = 11.78) compared to the threshold participants (M = 60.77, SD = 10.48), F(1, 138) = 7.86, p = .006, partial η2 = .06. Visual inspection revealed modest differences in Externalizing T scores between the two groups.
3.2.2 Childhood Sex-Typed Behavior as a Function of Diagnostic Status for Gender Identity Disorder
Table 7 shows the means and SDs (for continuous variables) or percentage scores (for dichotomous variables) for the threshold and subthreshold participants on measures of childhood sex-typed behavior. With age and social class covaried, the threshold participants had, on average, more cross-gender behavior in childhood than did the subthreshold participants. There were significant group differences on five of eight measures of childhood sex-typed behavior: (1) the Draw-a-Person test (p < .001), (2) free play, F(1, 120) = 28.94, p < .001, partial η2 = .19, (3) Gender Identity Interview, F(1, 84) = 9.07, p < .001, partial η2 = .10, (4) Gender Identity Questionnaire for Children, F(1, 96) = 19.13, p < .001, partial η2 = .17 and (5) cross-sex toy choice on the Playmate and Play Style Preferences Structured Interview, F(1, 40) = 9.72, p = .004, partial η2 = .21. The groups did not differ on temperament/activity level, cross-sex peer preference on the Playmate and Play Style Preferences Structured Interview, and difference between cross-sex and same-sex responses on the Rorschach (ps > .05).
3.3 Psychosexual Differentiation
3.3.1 Gender Identity at Follow-up
A summary of the psychosexual differentiation follow-up data, including gender
identity and sexual orientation for each participant is shown in Appendix K.
Table 7 |
|
|
|
|
|
|
|
|
|
|
Childhood Sex-Typed Behavior as a Function of Diagnostic Status for Gender Identity Disorder in Childhood |
|||||||||
|
|
Thresholda (n = 88) |
Subthreshold (n = 51) |
|
|
|||||
|
|
N |
% |
N |
% |
χ2 |
p |
|||
|
Draw-a-Person |
|
|
|
|
|
|
|||
|
Same-Sex |
26 |
29.5 |
37 |
74.0 |
25.40 |
<.001 |
|||
|
Cross-Sex |
62 |
70.5 |
13 |
26.0 |
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
SD |
N |
M |
SD |
N |
F |
p |
|
|
|
|
|
|
|
|
|
|
|
|
|
Child measures
|
|||||||||
|
Free Play Taskb |
.33 |
.53 |
85 |
-.40 |
.55 |
36 |
28.94 |
<.001 |
|
|
|
|
|
|
|
|
|
|
|
|
|
Rorschach Difference Scorec |
.58 |
3.74 |
78 |
.55 |
3.71 |
47 |
<1 |
ns |
|
|
|
|
|
|
|
|
|
|
|
|
|
Gender Identity Interviewd |
8.11 |
5.82 |
57 |
2.64 |
3.77 |
28 |
9.07 |
<.001 |
|
|
|
|
|
|
|
|
|
|
|
|
|
Gender Identity Questionnaire for Childrene |
2.65 |
.60 |
64 |
3.27 |
.58 |
33 |
19.13 |
<.001 |
|
|
|
|
|
|
|
|
|
|
|
|
|
Parent measures
|
|||||||||
|
Playmate and Playstyle Preferences Structured Interview: Cross-sex peer playf |
10.17 |
4.68 |
30 |
3.73 |
4.27 |
11 |
3.69 |
ns |
|
|
|
|
|
|
|
|
|
|
|
|
|
Playmate and Playstyle Preferences Structured Interview: Cross-sex toy playg |
8.03 |
2.72 |
30 |
4.45 |
2.02 |
11 |
9.72 |
.004 |
|
|
|
|
|
|
|
|
|
|
|
|
|
Temperament: Activity Levelh |
3.10 |
.49 |
88 |
2.95 |
.59 |
48 |
<1 |
ns |
|
|
aThreshold means that the patient met complete DSM-III, DSM-IIIR, or DSM-IV criteria for GID. bDifference between cross-sex and same-sex play during a free-play task. Positive score indicates more cross-sex play. cDifference between number of same-sex and cross-sex responses. Positive score indicates more cross-sex responses. dAbsolute range, 0-24. A higher score reflects more gender identity confusion. eAbsolute range, 1-5. A lower score indicates more cross-gender behavior. fAbsolute range, 0-14. A higher score indicates more cross-sex playmate/peer choices. gAbsolute range, 0-14. A higher score indicates more cross-sex toy choices. h Higher ratings indicate elevated activity levels and more rough-and-tumble play. |
|||||||||
3.3.1.1 Criteria for Persistence of Gender Dysphoria
Classification as either a persister or desister with regard to gender dysphoria was based on participants’ mean scores on the dimensional measures of concurrent gender identity, either the Gender Identity/Gender Dysphoria Questionnaire for Adolescents and Adults or the Gender Dysphoria Questionnaire, depending on which measure was administered.
Some participants completed both measures and, in these cases, the Gender Identity/Gender Dysphoria Questionnaire for Adolescents data were used as the basis for classification as it is a more psychometrically sophisticated measure of gender dysphoria compared to the Gender Dysphoria Questionnaire.
Participants were classified as having persistent gender dysphoria if their mean score on the Gender Identity/Gender Dysphoria Questionnaire for Adolescents was ≤ 3.00 (Deogracias et al., 2007). For participants who did not complete the Gender Identity/Gender Dysphoria Questionnaire for Adolescents, the Gender Dysphoria Questionnaire was used to make the classification. A participant was classified as a persister if he endorsed two or more of the following 5 items on the Gender Dysphoria Questionnaire: wish to have been born a girl (Item 1), wish to have surgery to change body (Item 2), feel more like a girl than a boy (Item 3), wonder if would be happier as a girl (Item 4), and very or somewhat dissatisfied with being a boy (Item 5).
Information regarding participants’ gender identity/gender dysphoria was also collected during the semi-structured clinical interview and, therefore, allowed for cross-validation of these questionnaire data. For those participants who did not complete the face-to-face interview, clinical information regarding gender identity/gender dysphoria was obtained through self- or parent-report or chart review. Across the entire sample, the Gender Identity/Gender Dysphoria Questionnaire for Adolescents and Adults was used to classify persistence or desistence for 64 participants, the Gender Dysphoria Questionnaire for 42 participants, and interview/parent report/chart data for 33 cases.
3.3.1.2 Rate of Persistence and Desistence
Of the 139 participants, 17 (12.2%) were classified as persisters and the remaining
122 (87.8%) were classified as desisters at follow-up. For the 42 participants where the Gender Dysphoria Questionnaire was used to determine gender identity status at follow-up, 38 were classified as desisters and 4 were classified as persisters. Of the 38 desisters, three endorsed one item on the Gender Dysphoria Questionnaire –one participant endorsed Item 4 and two participants endorsed Item 3. The four participants classified as persisters using the Gender Dysphoria Questionnaire endorsed three or more items. Specifically, one persister endorsed three items, one endorsed four items, and two endorsed five items. In regard to the specific items endorsed, all four persisters endorsed Item 1, three endorsed Item 2, four endorsed Item 3, four endorsed Item 4, and two endorsed Item 5.
For the 64 participants where the Gender Identity/Gender Dysphoria Questionnaire for Adolescents and Adults was used to determine gender identity status at follow-up, 12 were classified as persisters and the remaining 52 were classified as desisters. All 52 desisters had a mean score > 3.00 on the Gender Identity/Gender Dysphoria Questionnaire for Adolescents and Adults. Of the 12 persisters, 10 had a mean score ≤ 3.00 and two had mean scores that were > 3.00. In spite of having mean scores on the Gender Identity/Gender Dysphoria Questionnaire for Adolescents and Adults that were above the recommended cutoff for caseness (Deogracias et al., 2007), these two participants were considered persisters because their responses on the Gender Dysphoria Questionnaire as well as clinical interview data indicated that they were experiencing significant gender dysphoria. Thus,
clinical judgment was used to make the final classification for these two participants.
3.3.1.3 Persistence of Gender Dysphoria as a Function of GID Diagnosis in Childhood
The persistence rate of gender dysphoria was examined as a function of participants’ GID diagnostic status in childhood, that is, whether they met full diagnostic criteria or were subthreshold for the diagnosis. Of the 88 participants who met the full diagnostic criteria for GID in childhood, 12 (13.6%) were gender dysphoric at follow-up and the remaining 76 (86.4%) were no longer gender dysphoric. Of the 51 participants who were subthreshold for the GID diagnosis in childhood, 5 (9.8%) were gender dysphoric at follow-up and the remaining 46 (90.2%) were not. A chi-square analysis revealed that these rates of persistence across subthreshold and threshold groups did not differ significantly, χ2(1) < 1.
3.3.1.4 Summary of Gender Dysphoric Participants
Table 8 summarizes information on some domains of gender role outcome for the 17 participants classified as having persistent gender dysphoria. There was notable variation within the group of persisters in the extent to which they had socially and medically transitioned to the female gender role.
At follow-up, the majority of the gender dysphoric participants (n = 9) were not receiving any medical/biologic treatments to either suppress physical development of secondary sex characteristics/masculinization of their body or to feminize their body. The remaining 8 (47.1%) participants were taking puberty suppressing hormones or were on cross-sex hormonal therapy to feminize their physical appearance. Of the 9 participants who were not taking puberty suppressing or cross-sex hormones, 6 did not report any attempt to
|
Table 8 |
|||||||
|
Summary of Gender Dysphoric Participants |
|||||||
|
ID |
Year of childhood assessment |
Age at follow-up (in years) |
Legal name change
|
Using female name |
Living in female role |
On puberty blockers and/or cross-sex hormones |
Any surgery |
|
1 |
1975 |
18.24 |
No |
No |
Androgynous |
No |
No |
|
2 |
1979 |
19.38 |
No |
Yes |
Androgynous |
No |
No |
|
3 |
1980 |
35.14 |
Yes |
Yes |
Yes |
Yes |
No |
|
4 |
1980 |
19.08 |
No |
Yes |
Yes |
No |
No |
|
5 |
1983 |
26.04 |
No |
Yes |
Yes |
Yes |
No |
|
6 |
1984 |
18.82 |
No |
No |
No data |
No |
No |
|
7 |
1984 |
15.47 |
No |
No |
No |
No |
No |
|
8 |
1987 |
23.55 |
Yes |
Yes |
Yes |
Yes |
No |
|
9 |
1995 |
22.32 |
Noa |
Yes |
Yes |
Yes |
No |
|
10 |
1997 |
13.62 |
No |
No |
No |
No |
No |
|
11 |
1997 |
19.77 |
No |
Yes |
Yes |
Yes |
No |
|
12 |
1997 |
16.90 |
No |
No |
No |
No |
No |
|
13 |
1998 |
22.18 |
No |
Yes |
Partially |
Nob |
No |
|
14 |
2000 |
17.68 |
No |
Yes |
Yes |
Yes |
No |
|
15 |
2001 |
16.61 |
No |
No |
No |
No |
No |
|
16 |
2002 |
15.97 |
No |
Yes |
Yes |
Yes |
No |
|
17 |
2003 |
15.69 |
No |
Yes |
Yes |
Yes |
No |
|
aThis participant was in the process of applying for a legal name change. bPuberty suppressing hormones (blockers) were recommended. |
|||||||
present socially in the female gender role (e.g., using a female name, living in the female role). Of the remaining 3 participants, 2 were attempting to live socially in the female gender role and data were incomplete for 1 participant. None of the 17 gender dysphoric participants had received any type of surgery to feminize their appearance (e.g., breast implants, facial feminization surgery, genital reconstruction).
Among the 17 persisters, 11 were using a female name. Of these 11 participants, 2 had legally changed their name on official documents (e.g., driver’s license) and 1 was in the process of pursuing a legal name change. Nine of the gender dysphoric participants were living in the female gender role and 4 of them were living in the male gender role. Of the remaining 4 participants, 1 was living partially in the female role (e.g., would sometimes wear make-up and at others times presented androgynously, but did not wear stereotypic female clothing), 2 presented androgynously, and data were not available for 1 participant.
None of the 122 participants classified as desisters desired cross-sex hormones or sex reassignment surgery to feminize their bodies nor did they express a desire to get rid of their male sex characteristics. None of the desisters presented socially as women nor did they express the desire to socially transition to the female gender role (e.g., name change, clothing choice).
3.3.1.5 Odds of Persistent Gender Dysphoria
Formal epidemiological studies on the prevalence of GID in adolescents and adults have not been conducted. Since the 1960s, a number of studies have reported estimated prevalence rates (for a review, see Zucker & Lawrence, 2009). Rates have varied, in part, depending on the inclusion criteria (e.g., including individuals who have had, at least, hormonal treatment vs. only including individuals who have had sex reassignment surgery). For example, De Cuypere et al. (2007) estimated that 1 in 12,900 biological adult males have GID. Weitze and Osburg (1996) estimated a prevalence rate of 1 in 42,000. The estimated prevalence rate in most other studies have fallen within this range (i.e., 1/12900-1/42,000). Using the prevalence values estimated by De Cuypere et al. and Weitze and Osburg, the odds of persistent gender dysphoria (12.2%) in the present sample was 1794-5840 times higher than it is in biological males in the general population.
3.3.2 Sexual Orientation at Follow-up
On the basis of Kinsey ratings, participants who completed the face-to-face interview were classified into the following three sexual orientation groups for both fantasy and behavior: (1) heterosexual (Kinsey global ratings of 0-1); (2) bisexual/homosexual (Kinsey global ratings of 2-6), and (3) no sexual fantasy or behavior. Throughout this thesis, sexual orientation was classified in relation to birth sex, rather than the participants’ subjective sexual identity at follow-up. This is a particularly relevant issue for those participants who had persistent gender dysphoria. For example, if a biological male participant identified as female at follow-up, was sexually attracted to other biological males and self-labeled their sexual identity as heterosexual, they would be classified in the study as homosexual in relation to their birth sex.
Table 9 shows the frequency of ratings for sexual orientation in fantasy. Appendix K lists the individual global fantasy ratings for all participants for whom these data were available. Data were not available for 10 participants,[21] all of whom were desisters with regard to gender dysphoria. Based on the global ratings for sexual orientation in fantasy, 43 (33.3%) participants were classified as heterosexual in fantasy and 82 (63.6%) were classified as bisexual/homosexual in fantasy. In the remaining 4 (3.1%) cases, the participants were classified as having no sexual fantasies and, therefore, a Kinsey rating could not be assigned. In all 4 cases, the participants were desisters.
|
Table 9 |
||||||||||||||||
|
Kinsey Ratings for Sexual Orientation in Fantasy |
||||||||||||||||
|
|
Kinsey Ratinga |
|||||||||||||||
|
|
0 |
1 |
2 |
3 |
4 |
5 |
6 |
No Fantasy |
||||||||
|
Variable |
N |
% |
N |
% |
N |
% |
N |
% |
N |
% |
N |
% |
N |
% |
N |
% |
|
Crush |
36 |
36.7 |
0 |
0 |
2 |
2.0 |
4 |
4.1 |
2 |
2.0 |
11 |
11.2 |
29 |
29.6 |
14 |
14.3 |
|
Visual |
31 |
31.6 |
1 |
1.0 |
2 |
2.0 |
10 |
10.2 |
3 |
3.1 |
12 |
12.2 |
29 |
29.6 |
10 |
10.2 |
|
Dreams |
13 |
13.3 |
1 |
1.0 |
1 |
1.0 |
4 |
4.1 |
3 |
3.1 |
3 |
3.1 |
27 |
27.6 |
46 |
46.9 |
|
Masturbation |
21 |
21.9 |
2 |
2.1 |
3 |
3.1 |
6 |
6.3 |
2 |
2.1 |
7 |
7.3 |
33 |
34.4 |
22 |
22.9 |
|
Global Fantasy Rating |
40 |
31.0 |
3 |
2.3 |
3 |
2.3 |
8 |
6.2 |
2 |
1.6 |
14 |
10.9 |
55 |
42.6 |
4 |
3.1 |
|
aKinsey Ratings: 0 = Exclusively heterosexual 1 = Predominantly heterosexual, only incidentally homosexual 2 = Predominantly heterosexual but more than incidentally homosexual 3 = Equally homosexual and bisexual 4 = Predominantly homosexual, but more than incidentally heterosexual 5 = Predominantly homosexual, but incidentally heterosexual 6 = Exclusively homosexual |
||||||||||||||||
Of the 17 participants classified as gender dysphoric, 1 (5.9%) was heterosexual in fantasy and 16 (94.1%) were bisexual/homosexual in fantasy. Chi-square analysis revealed that the rates of sexual orientation in fantasy across this study, Green (1987), and Wallien and Cohen-Kettenis (2008) did not differ significantly, χ2(2) = 2.82, p > .05.
Table 10 shows the frequency of ratings for sexual orientation in behavior. Appendix K lists the individual global behavior ratings for all participants for whom these data were available. Data were available for 108 participants. Based on global ratings for sexual orientation in behavior, 29 (26.9%) participants were classified as heterosexual and 51 (47.2%) were classified as bisexual/homosexual. The remaining 28 (25.9%) participants did not report any sexual behaviors in the 12 months preceding the follow-up assessment.
For those participants who could be assigned a Kinsey rating (i.e., excluding those participants who did not report any sexual fantasies or behavior or for whom data were not available), the correlation between Kinsey global fantasy and global behavior ratings was very strong, r(78) = .92, p < .001.
3.3.2.1 Group Classification as a Function of Gender Identity and Sexual Orientation in Fantasy at Follow-up[22]
Combining gender identity (i.e., persister or desister) and sexual orientation in fantasy (i.e., heterosexual or bisexual/homosexual) at follow-up, the participants were classified into one of the following four outcome groups: (1) persistence of gender dysphoria with bisexual/ homosexual sexual orientation (n = 16); (2) desistence of gender dysphoria with
|
Table 10 |
||||||||||||||||
|
Kinsey Ratings for Sexual Orientation in Behavior |
||||||||||||||||
|
|
Kinsey Ratinga |
|||||||||||||||
|
|
0 |
1 |
2 |
3 |
4 |
5 |
6 |
No Sexual Behavior |
||||||||
|
Variable |
N |
% |
N |
% |
N |
% |
N |
% |
N |
% |
N |
% |
N |
% |
N |
% |
|
Dating |
27 |
27.3 |
0 |
0 |
0 |
0 |
4 |
4.0 |
1 |
1.0 |
0 |
0 |
33 |
33.3 |
34 |
34.0 |
|
Holding hands |
26 |
26.3 |
0 |
0 |
0 |
0 |
5 |
5.1 |
1 |
1.0 |
1 |
1.0 |
35 |
35.4 |
31 |
31.3 |
|
Kissing |
21 |
21.2 |
0 |
0 |
0 |
0 |
6 |
6.1 |
2 |
2.0 |
2 |
2.0 |
34 |
24.3 |
34 |
34.3 |
|
Genital/breast contact |
13 |
13.1 |
0 |
0 |
0 |
0 |
3 |
3.0 |
2 |
2.0 |
1 |
1.0 |
35 |
35.4 |
45 |
45.5 |
|
Intercourse |
8 |
8.2 |
0 |
0 |
0 |
0 |
3 |
3.1 |
2 |
2.0 |
0 |
0 |
27 |
27.6 |
58 |
59.2 |
|
Global Behavior Rating |
28 |
25.9 |
1 |
0.9 |
0 |
0 |
4 |
3.7 |
3 |
2.8 |
1 |
0.9 |
43 |
39.8 |
28 |
25.9 |
|
aKinsey Ratings: 0 = Exclusively heterosexual 1 = Predominantly heterosexual, only incidentally homosexual 2 = Predominantly heterosexual but more than incidentally homosexual 3 = Equally homosexual and bisexual 4 = Predominantly homosexual, but more than incidentally heterosexual 5 = Predominantly homosexual, but incidentally heterosexual 6 = Exclusively homosexual |
||||||||||||||||
bisexual/homosexual sexual orientation (n = 66); (3) desistence of gender dysphoria with heterosexual sexual orientation (n = 42); and (4) persistence of gender dysphoria with heterosexual sexual orientation (n = 1). The participants who reported no sexual fantasies (n = 4) could not be included in this outcome classification. Given that only 1 participant was classified as gender dysphoric with a co-occurring heterosexual sexual orientation (Group 4), this category was excluded from subsequent analyses that compared these outcome groups.
3.4 Demographic Characteristics
3.4.1 Demographic Characteristics in Childhood as a Function of Gender Identity and Sexual Orientation in Fantasy
Table 11 shows the demographic variables in childhood as a function of group.
One-way ANOVAs and chi-square were conducted to evaluate whether the outcome groups differed on demographic variables in childhood. The groups differed significantly on four of the five childhood demographic variables (ps < .05). The group comparison on ethnic background was not significant.
Duncan’s multiple range test for unequal Ns showed that the bisexual/homosexual persisters were, on average, significantly older at the time of the childhood assessment than both the heterosexual desisters and the bisexual/homosexual desisters, who did not differ significantly from each other. Regarding IQ, the bisexual/homosexual desisters had, on average, a higher IQ than the bisexual/homosexual persisters but did not differ significantly from the heterosexual desisters. There was no significant difference in childhood IQ score between bisexual/homosexual persisters and heterosexual desisters. The bisexual/
homosexual persisters were significantly more likely to come from a lower social class background compared to the heterosexual desisters and the bisexual/homosexual
|
Table 11 |
|||||||
|
Demographic Characteristics in Childhood and at Follow-up as a Function of Group |
|||||||
|
|
|
Group |
|
|
|
||
|
Variable |
|
Persisters Bisexual/ Homosexual (n = 16) |
Desisters Bisexual/ Homosexual (n = 66) |
Desisters Heterosexual
(n = 42) |
F or χ2 |
p |
η2 or Cramer’s V |
|
|
|||||||
|
Childhood |
|||||||
|
|
|||||||
|
Age (in years) |
M |
8.85 |
6.96 |
7.49 |
3.57 |
.031 |
.06 |
|
|
SD |
1.67 |
2.69 |
2.62 |
|
|
|
|
|
|
|
|
|
|
|
|
|
IQa |
M |
101.63 |
110.20 |
103.18 |
3.77 |
.026 |
.06 |
|
|
SD |
14.81 |
14.56 |
15.16 |
|
|
|
|
|
|
|
|
|
|
|
|
|
Social Classb |
M |
23.76 |
44.97 |
39.44 |
15.30 |
<.001 |
.20 |
|
|
SD |
10.22 |
13.64 |
15.91 |
|
|
|
|
|
|
|
|
|
|
|
|
|
Year of |
M |
1990.85 |
1989.83 |
1987.80 |
1.33 |
ns |
- |
|
Assessment |
SD |
9.65 |
6.07 |
8.68 |
|
|
|
|
|
|
|
|
|
|
|
|
|
Marital Statusc |
|
|
|
|
|
|
|
|
Two-parent |
N (%) |
7 (43.8) |
49 (74.2) |
24 (57.1) |
6.74 |
.034 |
.23 |
|
Other |
N (%) |
9 (56.3) |
17 (25.8) |
18 (42.9) |
|
|
|
|
|
|
|
|
|
|
|
|
|
Ethnicity |
|
|
|
|
|
|
|
|
Caucasian |
N (%) |
14 (87.5) |
58 (87.9) |
32 (76.2) |
2.77 |
ns |
- |
|
Other |
N (%) |
2 (12.5) |
8 (12.1) |
10 (23.8) |
|
|
|
|
|
|||||||
|
Follow-up |
|||||||
|
|
|||||||
|
Age at follow-up |
M |
20.32 |
22.13 |
17.85 |
10.41 |
<.001 |
.15 |
|
(in years)d |
SD |
5.67 |
4.97 |
3.95 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
IQ at follow-upa,e,f |
M |
99.07 |
110.47 |
104.19 |
3.82 |
.025 |
.07 |
|
|
SD |
16.29 |
13.54 |
17.50 |
|
|
|
|
|
|
|
|
|
|
|
|
|
Follow-up interval |
M |
11.47 |
15.17 |
10.36 |
9.63 |
<.001 |
.04 |
|
(in years) |
SD |
6.77 |
6.03 |
4.85 |
|
|
|
|
|
|
|
|
|
|
|
|
|
Social |
M |
.44 |
.43 |
.52 |
2.50 |
ns |
- |
|
Desirabilityg |
SD |
.17 |
.18 |
.19 |
|
|
|
|
aFull-Scale IQ was obtained with age-appropriate Wechsler intelligence scales. bHollingshead’s (1975) Four Factor Index of Social Status; absolute range, 8-66. cOther included the following family constellations: single parent, separated, divorced, living with relatives, or in the care of a child protection agency. dInterval denotes the time between childhood assessment and follow-up assessment. eFull Scale IQ estimated using four subtests: Vocabulary, Comprehension, Block Design and Object Assembly. fIQ were only available for participants who completed the face-to-face assessment. g Measured using Marlowe-Crowne Social Desirability Scale (Crowne & Marlow, 1960) and expressed as a proportion score. Absolute range, .00 - 1.00. Higher score indicates a greater propensity to give socially desirable responses. |
|||||||
desisters, who did not differ significantly from each other. The bisexual/homosexual desisters were more likely to be living with both parents compared to the bisexual/ homosexual persisters. There was no significant difference on marital status between the two desister groups.
As shown in Table 12, the demographic variables on which the three groups differed–age at assessment, IQ, social class, and marital status–were significantly correlated. To evaluate the influence of these variables on group outcome at follow-up, a multinomial logistic regression was performed. It can be seen from Table 13 that only social class had a significant contribution to the prediction of group outcome at follow-up. The bisexual/ homosexual persisters had a 13% increase in odds of coming from a lower social class background compared to the bisexual/homosexual desisters. However, social class did not predict outcome when the two desister groups were compared. Figure 1 shows the distribution of social class across the outcome groups.
|
Table 12 |
||||
|
Correlation Matrix of Childhood Demographic Variables on which the Groups Differed |
||||
|
Measures |
1 |
2 |
3 |
4 |
|
1. Age at assessment |
- |
-.42*** |
-.44*** |
.32*** |
|
2. IQ |
|
- |
.54*** |
-.35*** |
|
3. Social Class |
|
|
- |
-.58*** |
|
4. Marital Status |
|
|
|
- |
|
***p < .001 |
||||
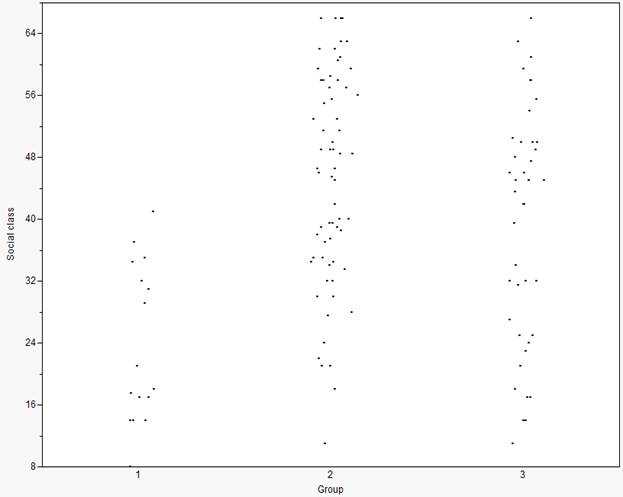
Figure 1. Distribution of social class for the outcome groups at follow-up.
1 = Bisexual/homosexual persisters (n = 16; M = 23.76, SD = 10.22)
2 = Bisexual/homosexual desisters (n = 66; M = 44.97, SD = 13.64)
3 = Heterosexual desisters (n = 42; M = 39.44, SD = 15.91)
Table 13 |
||||||||||
|
Multinomial Logistic Regression Predicting Group Outcome at Follow-up |
||||||||||
|
|
Bisexual/Homosexual Persisters |
Heterosexual Desisters |
||||||||
|
Predictor |
B |
SE |
Wald |
p |
eB |
B |
SE |
Wald |
p |
eB |
|
Age at Assessment |
0.11 |
0.14 |
0.62 |
ns |
1.12 |
-0.02 |
0.09 |
0.03 |
ns |
.98 |
|
IQ |
0.02 |
0.03 |
0.85 |
ns |
1.02 |
-0.02 |
0.02 |
1.91 |
ns |
.98 |
|
Social Class |
-0.14 |
0.04 |
13.66 |
<.001 |
.87 |
-0.01 |
0.02 |
0.13 |
ns |
.99 |
|
Marital Status |
-0.76 |
0.80 |
0.88 |
ns |
.47 |
0.43 |
0.52 |
0.70 |
ns |
1.54 |
|
Note. Reference group is the Bisexual/homosexual Desisters. This group was chosen as the reference because it represents the largest group size. Desistence of GID with a bisexual/ homosexual sexual orientation is also the most common long-term outcome for children with GID. |
||||||||||
3.4.2 Demographic Characteristics at Follow-up as a Function of Gender Identity and Sexual Orientation in Fantasy
Table 11 also shows the demographic variables of age and IQ at follow-up as a function of group. One-way ANOVAs revealed that both variables differed significantly among the three groups (ps < .01). Duncan’s multiple range test for unequal Ns showed that the heterosexual desisters were, on average, younger than both the bisexual/homosexual persisters and the bisexual/homosexual desisters, who did not differ significantly from each other.
Regarding IQ at follow-up, the results were similar to those for IQ in childhood. The bisexual/homosexual desisters had, on average, higher IQ than the bisexual/homosexual persisters but did not differ significantly from the heterosexual desisters. There was no significant difference in IQ between the bisexual/homosexual persisters and the heterosexual desisters.
Table 11shows the mean proportion score on the measure of social desirability as a function of group. A one-way ANCOVA for Group (with age at assessment, age at follow-up, IQ in childhood, IQ at follow-up, social class, and marital status6 covaried) was conducted to evaluate the proportion of socially desirable responses on the Marlow-Crowne Social Desirability Scale for participants according to their group classification at follow-up. There was no significant difference in the proportion of socially desirable responses on the Marlow-Crowne Social Desirability Scale as a function of gender identity and sexual orientation in fantasy (p = .089).
3.6 Childhood Sex-Typed Behavior
3.6.1 Childhood Sex-Typed Behavior as a Function of Gender Identity and Sexual Orientation at Follow-up
Table 14 shows the means and SDs (for continuous variables) or percentage scores (for dichotomous variables) of the childhood sex-typed variables obtained at the assessment as a function of the three outcome groups. ANCOVAs (with age at assessment, IQ, social class, and marital status[23] covaried) or chi-square were used to examine whether the groups differed on any of the reported variables. The corresponding F or chi-square values are also shown.
Of the 9 sex-typed measures, there was a significant difference between the groups on four child-report measures (first drawn person on the Draw-a-Person, free play, Gender Identity Interview, and cross-sex peer preference on the Playmate and Play Style Preferences
Structured Interview, and one parent-report measure (Gender Identity Questionnaire
|
Table 14 |
||||||||
|
Childhood Sex-Typed Behavior as a Function of Group |
||||||||
|
Variable |
|
Persisters Bisexual/ Homosexual |
Desisters Bisexual/ Homosexual |
Desisters Heterosexual
|
F or χ2 |
p |
η2 or Cramer’s V |
|
|
DSM Diagnosisa |
|
|
|
|
|
|
|
|
|
Threshold for GID |
N (%) |
12 (75.0) |
46 (69.7) |
23 (54.8) |
3.29 |
ns |
- |
|
|
Subthreshold for GID |
|
4 (25.0) |
20 (30.3) |
19 (45.2) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Child-report measures |
||||||||
|
Draw-a-Person |
|
|
|
|
|
|
|
|
|
Same-Sex Person Drawn First |
N (%) |
4 (25.0) |
27 (40.9) |
25 (59.5) |
6.61 |
.037 |
.23 |
|
|
Cross-Sex Person Drawn First |
|
12 (75.0) |
39 (59.1) |
17 (40.5) |
|
|
|
|
|
Free Play Taskb |
M |
.24 |
.23 |
-.06 |
7.82 |
.001 |
.13 |
|
|
|
SD |
.43 |
.62 |
.69 |
|
|
|
|
|
|
N |
13 |
60 |
37 |
|
|
|
|
|
Rorschach Difference Scorec |
M |
.40 |
.97 |
-.08 |
.53 |
ns |
- |
|
|
|
SD |
4.75 |
4.07 |
3.11 |
|
|
|
|
|
|
N |
15 |
61 |
36 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Gender Identity Interviewd |
M |
9.78 |
5.91 |
7.43 |
4.24 |
.018 |
.11 |
|
|
|
SD |
5.63 |
5.31 |
7.10 |
|
|
|
|
|
|
N |
9 |
46 |
21 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Playmate and Playstyle Preferences |
M |
9.75 |
8.13 |
8.08 |
3.54 |
.042 |
.20 |
|
|
Structured Interview: Cross-sex Peer Playe |
SD |
4.83 |
5.78 |
5.57 |
|
|
|
|
|
|
N |
8 |
16 |
12 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Playmate and Playstyle Preferences |
M |
8.75 |
7.00 |
6.67 |
2.55 |
.096 |
.15 |
|
|
Structured Interview: Cross-sex toy playf |
SD |
2.43 |
2.92 |
3.37 |
|
|
|
|
|
|
N |
8 |
16 |
12 |
|
|
|
|
|
|
||||||||
|
Parent-report measures |
||||||||
|
Gender Identity Questionnaire for |
M |
2.40 |
2.88 |
2.87 |
|
|
|
|
|
Childreng |
SD |
.49 |
.58 |
.85 |
4.05 |
.021 |
|
|
|
|
N |
10 |
53 |
22 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Temperament: Activity Levelh |
M |
2.95 |
3.08 |
3.03 |
.593 |
ns |
- |
|
|
|
SD |
.41 |
.49 |
.59 |
|
|
|
|
|
|
N |
15 |
65 |
41 |
|
|
|
|
|
aFor diagnosis, GID means that the patient met complete DSM-III, DSM-IIIR, or DSM-IV criteria for GID. bDifference between cross-sex and same-sex play during a free-play task. Positive score indicates more cross-sex play. cDifference between number of same-sex and cross-sex responses. Positive score indicates more cross-sex responses. dAbsolute range, 0-24. A higher score reflects more gender identity confusion. eAbsolute range, 0-14. A higher score indicates more cross-sex playmate/peer choices. fAbsolute range, 0-14. A higher score indicates more cross-sex toy choices. gAbsolute range, 1-5. A lower score indicates more cross-gender behavior. hAbsolute range, 1-5. A higher score indicates higher activity level. |
||||||||
for Children). The ANCOVA for the cross-sex toy preference on the Playmate and Play Style Preferences Structured Interview approached significance (p = .096). The significant one-way ANCOVAs were followed up with post hoc analyses using lmatrix commands and the significant chi-square was followed-up with pair-wise chi-square comparisons.
On the Draw-a-Person, there was one significant post-hoc contrast. The bisexual/ homosexual persisters were, on average, significantly more likely to draw a female first compared to the heterosexual desisters (p = .04). The comparison between the bisexual/ homosexual desisters and heterosexual desisters approached significance (p = .09), with the bisexual/homosexual desisters showing a greater tendency to draw a female first. The comparison between the bisexual/homosexual persisters and bisexual/homosexual desisters was not significant (p > .05). On the free play measure, all post-hoc contrasts were significant. The bisexual/homosexual persisters displayed, on average, more cross-sex play than did the bisexual/homosexual desisters and the heterosexual desisters. The latter two groups differed significantly from each other; the bisexual/homosexual desisters displayed, on average, significantly more cross-sex play than did the heterosexual desisters. On the Gender Identity Interview, a semi-structured interview that assesses gender identity, feelings of gender confusion, and gender dysphoria, the bisexual/homosexual persisters reported, on average, significantly more gender confusion than did the bisexual/homosexual desisters. The post-hoc comparison between the bisexual/homosexual persisters and the heterosexual desisters approached significance (p = .054), with the bisexual/homosexual persisters reporting more gender confusion than the heterosexual desisters. The comparison between the bisexual/homosexual desisters and heterosexual desisters was not significant. There was also significant group difference on the peer preference domain of the Playmate and Play Style Preferences Structured Interview. The bisexual/homosexual persisters had, on average, significantly more cross-sex peer preference compared to the bisexual/homosexual desisters and the heterosexual desisters, who did not differ significantly from each other. On the Gender Identity Questionnaire for Children, a parent-report measure of cross-gender interest and identification, the bisexual/homosexual persisters were reported as significantly more cross-gendered than the bisexual/homosexual desisters and the heterosexual desisters. The latter two groups did not differ significantly from each other.
As can be seen from Table 15, the childhood sex-typed behavior measures on which the groups differed were significantly correlated.[24] From these six measures (first drawn
|
Table 15 |
||||||
|
Correlation Matrix of Childhood Sex-Typed Measures on which the Groups Differed |
||||||
|
Measures |
1 |
2 |
3 |
4 |
5 |
6 |
|
1. Draw-a-Person |
- |
.46*** |
.36** |
.58*** |
.42* |
-.30** |
|
2. Free Play Task |
|
- |
.43*** |
.68*** |
.55** |
-.42*** |
|
3. Gender Identity Interview |
|
|
- |
.56*** |
.47** |
-.35** |
|
4. Playmate and Playstyle Preferences Structured Interview: Cross-sex peer play |
|
|
|
- |
.76*** |
-.47** |
|
5. Playmate and Playstyle Preferences Structured Interview: Cross-sex toy play |
|
|
|
|
- |
-.46** |
|
6. Gender Identity Questionnaire for Children |
|
|
|
|
|
- |
|
Note. The n values vary for each variable. *p < .05, **p < .01, ***p < .001 |
||||||
person on the Draw-a-Person, free play, Gender Identity Interview, cross-sex peer preference on the Playmate and Play Style Preferences Structured Interview,21 cross-sex toy preference on the Playmate and Play Style Preferences Structured Interview, and the Gender Identity Questionnaire for Children), a composite score of childhood sex-typed behavior was derived for each participant by taking the average of the six variables[25] (each expressed as z-scores). Thus, the composite score was expressed as a z-score. A higher composite z-score indicates more cross-gender behavior at assessment (Fig. 2).
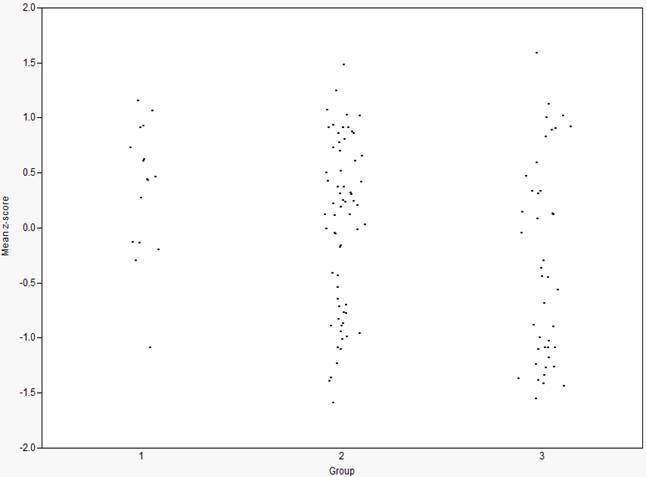
Figure 2. Distribution of the mean composite z-score for the outcome groups at follow-up.
1 = Bisexual/homosexual persisters (n = 16; M = .36, SD = .60)
2 = Bisexual/homosexual desisters (n = 66; M = .03, SD = .77)
3 = Heterosexual desisters (n = 42; M = -.32, SD = .90)
To evaluate the influence of childhood sex-typed behavior and demographic variables on group outcome at follow-up, a multinomial logistic regression was performed using the composite score and the demographic variables on which the groups differed[26]–age at assessment, IQ, and social class–as predictor variables. It can be seen from Table 16 that both social class and the composite score of childhood sex-typed behavior were significant predictors of group outcome at follow-up in the first model which compared the bisexual/ homosexual persisters to the bisexual/homosexual desisters.
|
Table 16 |
||||||||||
|
Multinomial Logistic Regression Predicting Group Outcome at Follow-up |
||||||||||
|
|
Bisexual/Homosexual Persisters |
Heterosexual Desisters |
||||||||
|
Predictor |
B |
SE |
Wald |
p |
eB |
B |
SE |
Wald |
p |
eB |
|
Age at Assessment |
.26 |
.16 |
2.90 |
.09 |
1.30 |
-.14 |
.11 |
1.55 |
.21 |
.87 |
|
IQ |
.02 |
.03 |
.58 |
.45 |
1.02 |
-.03 |
.01 |
2.77 |
.10 |
.97 |
|
Social Class |
-.12 |
.03 |
12.28 |
<.001 |
.89 |
-.01 |
.01 |
.51 |
.47 |
.99 |
|
Composite Z-score |
1.32 |
.55 |
5.82 |
.02 |
3.74 |
-.66 |
.31 |
4.38 |
.04 |
.52 |
|
Note. Reference group is the Bisexual/homosexual Desisters. This group was chosen as the reference because it represents the largest group size. Desistence of GID with a bisexual/ homosexual sexual orientation is also the most common long-term outcome for children with GID. |
||||||||||
The bisexual/homosexual persisters had a 274% increase in odds of having a higher composite score (i.e., more childhood cross-gender behavior) and 11% increase in odds of coming from a lower social class compared to the bisexual/homosexual desisters. Age at childhood assessment and IQ did not have a significant effect on group outcome (both ps > .05). In the second model, which compared the heterosexual desisters to the bisexual/ homosexual desisters, the only significant predictor of group outcome was the composite measures of sex-typed behavior. The bisexual/homosexual desisters had a 48% increase in odds of having a higher composite score compared to the heterosexual desisters.
3.6.2 Childhood Sex-Typed Behavior and Year of Assessment
The childhood assessment data were collected over the course of three decades, 1975-2004. Using correlation analysis, I assessed whether a relationship existed between year of assessment and scores on measures of sex-typed behavior. Across the entire sample, there was no significant correlation between year of assessment and any of the nine measures of childhood sex-typed behavior, all ps > .05. However, three correlations approached significance: free play (p = .05), the Gender Identity Questionnaire for Children (p = .08), and the cross-sex peer preference on Playmate and Play Style Preferences Structured Interview (p = .08). Across all three measures, there was a trend for participants with a later year of assessment (i.e., assessed more recently) to have had, on average, more childhood cross-gender behaviors compared to participants assessed earlier in the data collection period.
3.7 Peer Relations in Childhood
In the present study, we examined the quality of participants’ childhood peer relations by computing the Peer Relations Scale (Zucker, Bradley, & Sanikhani, 1997). In an effort to identify the relationship between peer relations and age across the entire sample of boys, participants’ age at childhood assessment and score on the Peer Relations Scale was correlated. The correlation was significant, r(121) = .58, p < .001, with older boys having poorer peer relations than younger boys. To examine the relationship between peer relations and behavior problems in childhood, participants Peer Relations Score was correlated with the sum of items rated as 1 or 2 on the CBCL, with the three items contributing to the Peer Relations Scale removed to prevent artificial inflation of the sum score.[27] The correlation was significant, r(121) = .43, p < .001.
A one-way ANCOVA (with age at assessment, IQ in childhood, social class, and marital status co-varied) was conducted to examine whether the three outcome groups at follow-up differed in the quality of their peer relations in childhood. The ANCOVA was not significant, F(2, 120) < 1.
3.8 Childhood Behavior Problems as a Function of Gender Identity and Sexual Orientation at Follow-up
Table 17 shows the maternal ratings on the Child Behavior Checklist (CBCL) as a function of group. ANCOVAs (with age at assessment, IQ, social class, and marital status[28] co-varied) were used to examine whether the groups differed on any of the reported childhood variables. The corresponding F values are also reported.
One-way ANCOVAs for Group revealed that there were no significant differences between the three groups on Internalizing T score, Externalizing T score or Total Problems T score at the childhood assessment (ps > .05). Table 17 also shows the percentage of participants in each group who fell within the clinical range (T score > 90th percentile) according to their Internalizing, Externalizing, and Total Problems T scores. For the bisexual/homosexual persisters, 62.5%-68.8% fell within the clinical range depending on whether they were classified according to their Internalizing T score, Externalizing T Score or Total T score. For the bisexual/homosexual desisters, 40.9%-42.4% were within the
|
Table 17 |
|||||||||||||||
|
Behavior Problems in Childhood and Follow-up as a Function of Group |
|||||||||||||||
|
|
Group |
|
|
|
|||||||||||
|
|
Persisters Bisexual/Homosexual |
Desisters Bisexual/Homosexual |
Desisters Heterosexual |
|
|
|
|||||||||
|
Variable |
M |
SD |
Clinical Range (%)a |
N |
M |
SD |
Clinical Range (%)a |
N |
M |
SD |
Clinical Range (%)a |
N |
F |
p |
η2 |
|
Childhood |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Internalizing T |
64.69 |
9.26 |
68.8b |
16 |
60.39 |
8.90 |
42.4b |
66 |
64.45 |
10.03 |
54.8b |
42 |
1.14 |
ns |
- |
|
Externalizing T |
65.88 |
9.43 |
62.5c |
16 |
59.39 |
10.98 |
42.4c |
66 |
61.67 |
11.21 |
42.9c |
42 |
<1 |
ns |
- |
|
Total T |
66.75 |
10.76 |
62.5d |
16 |
61.05 |
10.83 |
40.9d |
66 |
64.48 |
11.57 |
50.0d |
42 |
<1 |
ns |
- |
|
Follow-up Parent Report |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Internalizing T |
59.23 |
8.60 |
23.1e |
13 |
57.91 |
11.93 |
36.4e |
44 |
55.44 |
12.19 |
24.2e |
32 |
1.47 |
ns |
- |
|
Externalizing T |
61.92 |
8.18 |
23.1f |
13 |
55.73 |
11.40 |
22.7f |
44 |
53.94 |
10.39 |
15.2f |
32 |
1.10 |
ns |
- |
|
Total T |
62.54 |
8.21 |
38.5g |
13 |
55.95 |
12.11 |
20.5g |
44 |
55.31 |
13.10 |
27.3g |
32 |
<1 |
ns |
- |
|
Follow-up Self Report |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Internalizing T |
62.87 |
13.83 |
46.7h |
15 |
55.77 |
9.95 |
20.0h |
48 |
48.44 |
10.87 |
11.1h |
36 |
5.05 |
.008 |
.10 |
|
Externalizing T |
59.00 |
13.34 |
53.3i |
15 |
55.73 |
11.09 |
24.0i |
48 |
51.28 |
9.38 |
5.6i |
36 |
<1 |
ns |
- |
|
Total T |
61.53 |
13.88 |
46.7j |
15 |
54.90 |
10.64 |
18.0j |
48 |
49.39 |
10.52 |
11.1j |
36 |
2.60 |
.08 |
- |
|
aT score > 90th percentile. bχ2(2) = 4.15, ns. cχ2(2) = 2.23, ns. dχ2(2) = 2.68, ns. eχ2(2) = 1.66, ns. fχ2(2) <1, ns. gχ2(2) = 1.79, ns. hχ2(2) = 8.17, p = .017. i χ2(2) = 14.47, p = .001. j χ2(2) = 8.63, p = .013. |
|||||||||||||||
clinical range and, for the heterosexual desisters, 42.9%-54.8% were within the clinical range. These percentages did not differ significantly (see chi-square results in Table 17, footnotes b, c, and d).
3.9 Psychosexual Measures as a Function of Group
Table 18 summarizes six psychosexual variables obtained at follow-up as a function of group: (1) Gender Dysphoria, (2) the Recalled Childhood Gender Identity/Gender Role Questionnaire, (3) Erotic Response and Orientation Scale, Homoerotic Score, (4) Erotic Response and Orientation Scale, Heteroerotic Score, (5) Sexual History Questionnaire, Homoerotic Scale, and (6) Sexual History Questionnaire, Heteroerotic Scale. Table 18 also summarizes the results of a parent-report measure of gender role behavior at follow-up.
A series of ANCOVAs with age at assessment, IQ in childhood, social class, age at follow-up, IQ at follow-up, and marital status co-varied were conducted to evaluate whether the three groups differed significantly on any of the self-report measures. There was a significant main effect for group on all ANCOVAs. The significant ANCOVAs were followed up with post-hoc analyses using lmatrix commands, the results of which are reported below. For the Erotic Response and Orientation Scale (EROS), significant Group x EROS (homoerotic vs. heteroerotic) interaction was decomposed with between-and within-group pair-wise comparisons. Similarly, for the Sexual History Questionnaire (SHQ), significant Group x SHQ (homoerotic vs. heteroerotic) interaction was decomposed with between-and within-group pair-wise comparisons.
3.9.1 Gender Dysphoria
On the gender dysphoria measure,[29] there was a significant main effect for Group,
|
Table 18 |
|||||||
|
Psychosexual Measures as a Function of Group |
|||||||
|
|
|
Group |
|
|
|
||
|
Variable |
|
Persisters Bisexual/ Homosexual |
Desisters Bisexual/ Homosexual |
Desisters Heterosexual |
F |
p |
η2 |
|
|
|
|
|
|
|
|
|
|
Self-Report |
|||||||
|
Gender Dysphoriaa |
M |
.66 |
.03 |
.01 |
259.85 |
<.001 |
.85 |
|
|
SD |
.22 |
.05 |
.02 |
|
|
|
|
|
N |
15 |
49 |
36 |
|
|
|
|
|
|
|
|
|
|
|
|
|
RCGIb |
M |
1.96 |
3.01 |
3.75 |
30.20 |
<.001 |
.51 |
|
|
SD |
.44 |
.51 |
.68 |
|
|
|
|
|
N |
11 |
42 |
15 |
|
|
|
|
|
|
|
|
|
|
|
|
|
EROS |
|
|
|
|
64.30 |
<.001 |
.58 |
|
|
|
|
|
|
|
|
|
|
EROS: Homoeroticc |
M |
3.53 |
3.39 |
1.04 |
|
|
|
|
|
SD |
1.25 |
.96 |
.14 |
|
|
|
|
|
N |
15 |
49 |
37 |
|
|
|
|
|
|
|
|
|
|
|
|
|
EROS: Heteroeroticc |
M |
1.23 |
1.83 |
2.93 |
|
|
|
|
|
SD |
.42 |
1.00 |
1.08 |
|
|
|
|
|
N |
15 |
49 |
37 |
|
|
|
|
|
|
|
|
|
|
|
|
|
SHQ |
|
|
|
|
26.40 |
.001 |
.37 |
|
|
|
|
|
|
|
|
|
|
SHQ: Homoeroticd |
M |
3.38 |
2.46 |
1.00 |
|
|
|
|
|
SD |
1.25 |
1.19 |
.00 |
|
|
|
|
|
N |
15 |
49 |
36 |
|
|
|
|
|
|
|
|
|
|
|
|
|
SHQ: Heteroeroticd |
M |
1.37 |
1.80 |
2.02 |
|
|
|
|
|
SD |
.56 |
.95 |
.88 |
|
|
|
|
|
N |
15 |
49 |
36 |
|
|
|
|
|
|||||||
|
Parent-Report |
|||||||
|
|
|
|
|
|
|
|
|
|
GIDRQ-Ade |
M |
2.30 |
3.28 |
3.85 |
23.28 |
<.001 |
.37 |
|
|
SD |
1.09 |
.58 |
.52 |
|
|
|
|
|
N |
12 |
44 |
31 |
|
|
|
|
Note. RCGI = Recalled Childhood Gender Identity/Gender Role Questionnaire; EROS = Erotic Response and Orientation Questionnaire; SHQ = Sexual History Questionnaire; GIGRQ-Ad = Gender Identity/Gender Role Questionnaire for Adolescents. aAbsolute range, .00-1.00. A higher score indicates more gender dysphoria. This is a proportion score which represents participants’ scores on the Gender Identity/Gender Role Questionnaire for Adolescents and Adults or Gender Dysphoria Questionnaire, depending on which measure was administered. bAbsolute range, 1-5. A lower score indicates more recalled childhood cross-gender behavior. cAbsolute range, 1.5. A higher score indicates more frequent sexual fantasies. dAbsolute range, 1.5. A higher score indicates more frequent sexual behavior. eFor this measure, there was no absolute range, because one item did not have a scale–it asked parents to report on the number of male and/or female peers their child has. In this study, the actual range, across all three groups, was .78-4.80, with higher score reflecting more gender-typical behavior. |
|||||||
F(2, 99) = 259.85, p < .001. The strength of the relationship between Group and the gender
dysphoria score, as assessed by partial η2, was strong, with Group accounting for 85.1% of
the variance in gender dysphoria scores. Post-hoc analyses using lmatrix commands showed that the bisexual/homosexual persisters reported, on average, significantly more concurrent gender dysphoria than did the bisexual/homosexual desisters and the heterosexual desisters (both ps < .001).
3. 9.1.1 “Caseness” of Gender Dysphoria on the Gender Identity Questionnaire for Adolescents and Adults
Deogracias et al. (2007) suggested that a mean score of ≤ 3 on the Gender Identity
Questionnaire for Adolescents and Adults[30] can be used to determine whether a participant was gender dysphoric. In subsequent studies examining the psychometric properties of the Gender Identity Questionnaire for Adolescents and Adults (Singh et al., 2010; Singh, McMain, & Zucker, 2011), this criterion for “caseness” of gender dysphoria was also applied. In the present study, the Gender Identity Questionnaire for Adolescents and Adults data were available for 64 participants (12 persisters, 52 desisters).
As shown in Fig. 3, for the 12 persisters who completed the Gender Identity
Questionnaire for Adolescents and Adults, all but 2 participants[31] had scores lower than 3.00 (M = 2.50, SD = .78; range, 1.78-4.30), whereas all of the participants classified as desisters (and for whom data were available) had a mean score greater than 3.00 (M = 4.86, SD = .18; range, 4.19-5.00). Therefore, using the above-stated criterion for caseness, 83.3% of the bisexual/homosexual persisters (for whom data were available) met the criterion compared to 0% of the bisexual/homosexual desisters and 0% of the heterosexual desisters.
The group differences on mean scores on the Gender Identity Questionnaire for Adolescents and Adults were significant. A one-way ANCOVA (with age at assessment, IQ in childhood, social class, age at follow-up, IQ at follow-up, and marital status co-varied) for Group was significant, F(2, 61) = 206.103, p < .001, partial η2 = .89. Post hoc analyses using lmatrix commands revealed two significant contrasts. The bisexual/homosexual persisters, on average, reported significantly more concurrent gender dysphoria than did the bisexual/ homosexual desisters and the heterosexual desisters (both ps < .001).
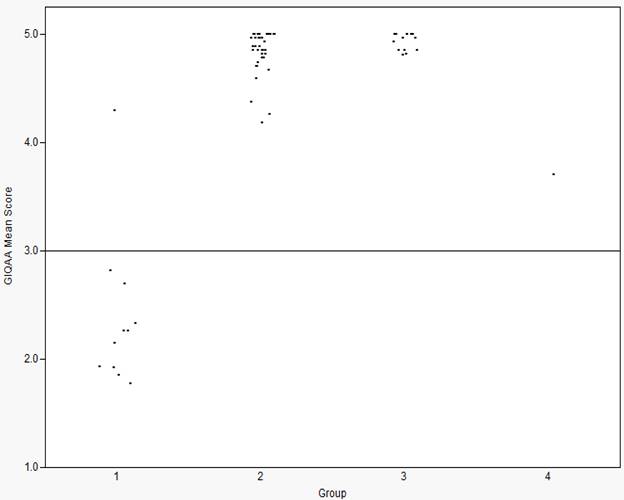
Figure 3. Distribution of the mean scores on the Gender Identity Questionnaire for Adolescents and Adults for the outcome groups at follow-up.
1 = Bisexual/homosexual persisters (n = 16)
2 = Bisexual/homosexual desisters (n = 66)
3 = Heterosexual desisters (n = 42)
4 = Heterosexual persisters (n = 1)
3.9.2 Recalled Childhood Sex-Typed Behavior
Table 19 shows the mean Recalled Childhood Gender Identity/Gender Role Questionnaire (RCGI) Factor 1 score for the entire sample, which pertained to the participants’ recollections of their sex-typed behaviors in childhood. A lower score on the RCGI indicates more recalled cross-gender identity/gender role. This mean score can be
|
Table 19 |
|||
|
Mean Factor 1 Score on the Recalled Childhood Gender Identity/Gender Role Questionnaire |
|||
|
Group |
M |
SD |
db |
|
Total follow-up samplea (n = 71) |
3.03 |
.77 |
|
|
Childhood Diagnosis |
|
|
|
|
Threshold for GID (n = 51) |
2.94 |
.75 |
.42c |
|
Subthreshold for GID (n = 20) |
3.27 |
.78 |
|
|
|
|
|
|
|
(Clinical Control adolescent males (n = 40))d |
(4.31) |
(.36) |
|
|
(Clinical Control adult males (n = 37))d |
(4.09) |
(.68) |
|
|
(GID adolescent males (n = 19))d |
(2.64) |
(.93) |
|
|
(GID adult males (n = 33))d |
(2.74) |
(.84) |
|
|
Note. Absolute range, 1.00-5.00. A lower score indicates more recalled cross-gender identity/gender role. aSome participants did not complete the RCGI because its development succeeded the beginning of data collection. bCalculated as M1-M2/SDcomparison group. cReference group was the participants who were subthreshold for the GID diagnosis in childhood. dSingh et al. (2010). |
|||
compared with a sample of clinical control males (i.e., males with mental health concerns other than GID) unselected for their gender identity or sexual orientation reported on in Singh et al. (2010) and also shown in Table 19. These clinical control males were collected as part of a research study which examined the psychometric studies of the Gender Identity/ Gender Role Questionnaire for Adolescents and Adults and which was conducted in our Gender Identity Service (see Singh et al., 2010). Thus, the RCGI data from these clinical control males were available for comparison to the males in the present follow-up study. It can be seen that, as a group, the males in the present study recalled relatively more childhood cross-gender behavior (M = 3.03, SD = .77) compared to clinical control adult males (M = 4.09, SD = .68) and clinical control adolescent males (M = 4.31, SD = .36). With age covaried[32], the mean RCGI score across these three groups was significantly different, F(2, 148) = 59.71, p < .001, partial η2 = .45. Post hoc analyses using lmatrix commands revealed two significant contrasts. The males in the present study recalled, on average, significantly more childhood cross-gender behavior compared to clinical control adult males and adolescent males (both ps < .001). The two clinical control groups of males did not differ significantly from each other (p > .05). The recollections of childhood sex-typed behavior by the males in this sample was similar to the childhood recollections of other biological males with GID assessed for the first time in adolescence or adulthood (Table 19) and reported on in Singh et al. (2010), F(2, 123) = 2.21, p > .05.
Table 19 also shows the mean Recalled Childhood Gender Identity/Gender Role Questionnaire Factor 1 score of the participants as a function of DSM diagnostic status for GID in childhood. With age and social class covaried, the threshold participants recalled, on average, more cross-gender behavior in childhood than the participants who were subthreshold for a diagnosis of GID. However, the difference only approached significance F(1, 70) = 3.53, p = .06.
3.9.2.1 Recalled Childhood Sex-Typed Behavior as a Function of Group
On the Recalled Childhood Gender Identity/Gender Role Questionnaire (see Table 18), there was a significant main effect for Group, F(2, 67) = 30.20, p < .001, partial η2 = .51. Post-hoc analyses revealed that all three pair-wise group comparisons were significant (ps < .001). The bisexual/homosexual persisters recalled, on average, significantly more cross-gender behavior during childhood than both the bisexual/homosexual desisters and the heterosexual desisters. The bisexual/homosexual desisters, in turn, recalled significantly more cross-gender behavior in childhood than did the heterosexual desisters.
Across the entire group of 139 participants, there were 71 cases where both the gender dysphoria score and the Recalled Childhood Gender Identity/Gender Role Questionnaire score was available. Based on these cases, the correlation between the gender dysphoria score and the Recalled Childhood Gender Identity/Gender Role Questionnaire was significant, r(71) = -.65, p < .001.
3.9.2.2 Recalled Childhood Sex-Typed Behavior and Childhood-Sex-Typed Behavior
Across the entire sample, the relationship between recalled childhood sex-typed behavior (assessed at follow-up) and childhood sex-typed behavior at the original assessment was examined. Participants’ score on the Recalled Childhood Gender Identity/Gender Role Questionnaire was correlated with their score on seven measures of childhood sex-typed behaviors (see Table 14 for a listing of these measures). There were four significant correlations. Participants’ recollections of their sex-typed behaviors was significantly correlated with parent report of their childhood cross-gender behaviors on the Gender Identity Questionnaire for Children, r(65) = .35, p < .01. The Recalled Childhood Gender Identity/Gender Role Questionnaire also correlated significantly with free play, r(65) = -.35, p < .01, cross-sex peer choice on the Playmate and Play Style Preferences Structured Interview, r(33) = -.39, p < .05, and cross-sex toy choice on the Playmate and Play Style Preferences Structured Interview, r(33) = -.44, p < .01. There was no significant correlation between the Recalled Childhood Gender Identity/Gender Role Questionnaire and the Gender Identity Interview, temperament/activity level, and difference between cross-sex and same-sex responses on the Rorschach (ps > .05).[33]
3.9.3 Sexual Orientation
The results for sexual orientation in fantasy are presented first, followed by sexual orientation in behavior.
3.9.3.1 Sexual Orientation in Fantasy
For the Erotic Response and Orientation Scale (EROS), a concurrent measure of sexual orientation in fantasy, a mean homoerotic fantasy score was computed for the 8 items pertaining to attraction to men and a mean heteroerotic fantasy score was computed for the 8 items pertaining to attraction to women. A 3 (group) x 2 (EROS: homoerotic vs. heteroerotic) repeated measures ANCOVA revealed a significant interaction, Wilks’ Lambda = .42, F(2, 92) = 64.30, p < .001, partial η2 = .58, which was decomposed with post hoc contrasts. Across the groups, the heterosexual desisters reported, on average, significantly more heteroerotic fantasy than both the bisexual/homosexual persisters (p < .001) and the bisexual/ homosexual desisters (p < .001). Furthermore, the bisexual/homosexual desisters reported, on average, significantly more heteroerotic fantasy than the bisexual/homosexual persisters (p = .036). In contrast, the heterosexual desisters reported, on average, significantly less homoerotic fantasy than both the bisexual/homosexual persisters and the bisexual/ homosexual desisters (both ps < .001). The bisexual/homosexual persisters and bisexual/ homosexual desisters did not differ significantly from each other on mean homoerotic fantasy (p > .05). Within groups, the bisexual/homosexual persisters reported, on average, significantly more homoerotic than heteroerotic fantasy (p < .001); the bisexual/homosexual desisters also reported, on average, significantly more homoerotic than heteroerotic fantasy (p < .001). In contrast, the heterosexual desisters reported, on average, significantly more heteroerotic than homoerotic fantasy (p < .001).
I also classified patients dichotomously as either “homosexual” or “non-homosexual” based on an EROS difference score (Homoerotic – Heteroerotic). If the difference score was > 0, the participant was classified as homosexual in relation to their birth sex. If the difference score was ≤ 0, then the patient was classified as non-homosexual (i.e., heterosexual, bisexual, or asexual). Based on this criterion (Table 20), 93.3% of the bisexual/
homosexual persisters and 80.0% of the bisexual/homosexual desisters were classified as homosexual; in contrast, none of the heterosexual desisters were classified as homosexual.
3.9.3.2 Sexual Orientation in Behavior
For the Sexual History Questionnaire, a measure of concurrent sexual orientation in behavior, a mean homoerotic behavior score was computed for the 10 items pertaining to attraction to men and a mean heteroerotic behavior score was also computed for
the 10 items pertaining to attraction to women. A 3 (group) x 2 (Sexual History Questionnaire: homoerotic vs. heteroerotic) repeated measure ANCOVA revealed a
|
Table 20 |
||||
|
Sexual Orientation in Fantasy and Behavior on EROS and SHQ |
||||
|
Variable
|
|
Persisters Bisexual/ Homosexual (n = 15) |
Desisters Bisexual/ Homosexual (n = 50) |
Desisters Heterosexual
(n = 37) |
|
EROS |
% Homosexuala |
93.3 |
80.0 |
0 |
|
|
N |
14 |
40 |
0 |
|
SHQ |
% Homosexualb |
93.3 |
64.0 |
0 |
|
|
N |
14 |
32 |
0 |
|
Note. EROS = Erotic Response and Orientation Scale; SHQ = Sexual History Questionnaire. aEROS difference score (Homoerotic – Heteroerotic) > 0. bSHQ difference score (Homoerotic – Heteroerotic) > 0. |
||||
significant interaction, Wilks’ lambda = .63, F(2, 91) = 26.40, p < .001, partial η2 = .37, which was decomposed with post hoc contrasts.
Across groups, there was no significant difference on heterosexual behavior (all ps > .05). However, the post hoc contrast between the bisexual/homosexual persisters and the heterosexual desisters approached significance (p = .08), with the latter group reporting more heterosexual behavior. In contrast, all three post hoc comparisons on homosexual behavior were significant. The heterosexual desisters reported, on average, significantly less homoerotic behavior than both the bisexual/homosexual persisters and the bisexual/ homosexual desisters (both ps < .001). The bisexual/homosexual persisters reported, on average, significantly more homoerotic behavior than the bisexual/homosexual desisters (p < .01). Within groups, the bisexual/homosexual persisters reported, on average, significantly more homoerotic than heteroerotic behavior (p < .001); the bisexual/homosexual desisters also reported, on average, significantly more homoerotic than heteroerotic behavior (p = .001). In contrast, the heterosexual desisters reported, on average, significantly more heteroerotic than homoerotic behavior (p < .001).
I also classified patients dichotomously as either “homosexual” or “non-homosexual” based on the Sexual History Questionnaire difference score (Homoerotic – Heteroerotic). If the difference score was > 0, the participant was classified as homosexual in relation to their birth sex. If the difference score was ≤ 0, then the patient was classified as non-homosexual (i.e., heterosexual, bisexual, or asexual). Based on this criterion (Table 20), 93.3% of the bisexual/homosexual persisters and 64.0% of bisexual/homosexual desisters were classified as homosexual; in contrast, none of the heterosexual desisters were classified as homosexual.
3.9.4 Parent Report of Concurrent Gender Role
On the parent report Gender Identity/Gender Role Questionnaire for Adolescents, a measure of concurrent gender role behaviors, there was a significant main effect for Group, F(2, 86) = 23.28, p < .001, partial η2 = .37 (Table 18). Post-hoc analyses revealed that all three pair-wise group comparisons were significant (all ps < .001). The bisexual/homosexual persisters had, on average, more cross-gender behavior than both the bisexual/homosexual desisters and the heterosexual desisters. The bisexual/homosexual desisters had, on average, significantly more cross-gender compared to the heterosexual desisters.
Across the entire sample, the relationship between parent report of concurrent gender role behaviors and childhood sex-typed behaviors was examined. Participants’ score on the Gender Identity/Gender Role Questionnaire for Adolescents was correlated with their score on nine measures of sex-typed behaviors (see Table 16 for a listing of these measures). There was only one significant correlation. Participants’ parent report of concurrent gender role behavior was significantly correlated with parent-report of their child’s cross-gender behavior on the Gender Identity Questionnaire for Children, r(46) = -.39, p < .01.
3.10 Behavior Problems at Follow-up
Table 21 shows the correlation coefficients on the behavior measures in childhood and at follow-up. Cohen’s (1988) criteria were used to evaluate the magnitude of the correlations: small (r = .10-.29), medium (r = .30-.49) or large (r ≥ .50).
Maternal ratings in childhood was significantly correlated with maternal ratings at follow-up for Internalizing problems (r[90] = .36, p < .001), Externalizing problems (r[90] = .36, p < .001), and Total problems (r[90] = .43, p < .001). Maternal ratings at follow-up was significantly correlated with participant self-report at follow-up for Internalizing problems (r[87] = .37, p < .001), Externalizing problems (r[87] = .49, p < .001), and Total problems (r[87] = .47, p < .001). None of correlations between maternal ratings in childhood and participant self-report at follow-up were significant (ps > .05).
3.10.1 Behavior Problems at Follow-up as a Function of Gender Identity and Sexual Orientation: Maternal-Report
Table 17 shows the maternal ratings on the CBCL/ABCL at follow-up as a function of group. ANCOVAs (with age at assessment, IQ in childhood, social class, age at follow-up, IQ at follow-up, and marital status[34] co-varied) were used to examine whether the groups differed on any of the reported follow-up variables (Internalizing T score, Externalizing T score, Total T score). One-way ANCOVAs for Group revealed no significant group differences on maternal ratings of Internalizing, Externalizing, and Total Problems at follow-up. Table 17 also shows the percentage of participants in each group who fell within the clinical range (T score > 90th percentile) according to their Internalizing, Externalizing, and
Table 21 |
||||||||||
|
Correlations between Behavior Problems in Childhood (CBCL) and Follow-up (YSR/ASR, CBCL/ABCL) |
||||||||||
|
|
Measure |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
|
1 |
CBCL Internalizing T
|
- |
.79*** |
.82*** |
.04 |
.03 |
.08 |
.36*** |
.27** |
.39*** |
|
2 |
CBCL Externalizing T
|
|
- |
.89*** |
.03 |
.09 |
.11 |
.30** |
.36*** |
.40*** |
|
3 |
CBCL Total T
|
|
|
- |
.02 |
.07 |
.10 |
.34** |
.35** |
.43*** |
|
4 |
Follow-up Self-Report Internalizing T |
|
|
|
- |
.69*** |
.89*** |
.37** |
.35** |
.37** |
|
5 |
Follow-up Self-Report Externalizing T |
|
|
|
|
- |
.90*** |
.35** |
.49*** |
.41*** |
|
6 |
Follow-up Self-Report Total T |
|
|
|
|
|
- |
.40*** |
.49*** |
.47*** |
|
7 |
Follow-up Parent- Report Internalizing T |
|
|
|
|
|
|
- |
.71*** |
.89*** |
|
8 |
Follow-up Parent- Report Externalizing T |
|
|
|
|
|
|
|
- |
.90*** |
|
9 |
Follow-up Parent- Report Total T |
|
|
|
|
|
|
|
|
- |
|
Note. CBCL at childhood assessment, n = 124. YSR/ASR self report at follow-up, n = 100. CBCL/ABCL parent-report at follow-up, n = 90. *p < .05, **p < .01, ***p < .001. |
||||||||||
Total T scores obtained from maternal ratings. For the bisexual/homosexual persisters, 23.1%-38.5% fell within the clinical range depending on the specific variable used in classification (i.e., Internalizing T, Externalizing T, or Total T); for the bisexual/homosexual desisters, 20.5%-36.4% fell in the clinical range; for the heterosexual desisters, 15.2%-27.3% fell in the clinical range. These percentages did not differ significantly (see Table 17, footnotes e, f, and g).
3.10.2 Behavior Problems at Follow-up as a Function of Gender Identity and Sexual Orientation: Self-Report
ANCOVAs (with age at assessment, IQ in childhood, social class, age at follow-up, IQ at follow-up, and marital status[35] co-varied) were conducted to examine whether the groups differed on participant self-report of their behavior problems on the YSR/ASR at follow-up. Table 17 shows participants’ self-report ratings on the YSR/ASR as a function of group. There was a significant main effect for Group on Internalizing T score, F(2, 99) = 5.05, p = .008, but not for Externalizing T score, F(2, 99) < 1. The ANCOVA for Total T score approached significance, F(2, 99) = 2.60, p = .08. For Internalizing T score, post hoc analyses using lmatrix commands revealed two significant pairwise comparisons. The heterosexual desisters had, on average, a lower Internalizing T score than both the bisexual/ homosexual persisters and the bisexual/homosexual desisters (both ps < .05), who did not differ from each other (p > .05).
Table 17 also shows the percentage of participants in each group who fell within the clinical range (T score > 90th percentile) according to their self-report of Internalizing, Externalizing, and Total Problems. For the bisexual/homosexual persisters, 46.7%-53.3% fell within the clinical range depending on whether they were classified according to their Internalizing T score, Externalizing T Score, or Total T score; for the bisexual/homosexual desisters, 18.0%-24.0% fell in the clinical range; for the heterosexual desisters, 5.6%-11.1% fell within the clinical range. These percentages were significantly different (ps ranged from .001-.017, refer to Table 17 footnotes h, i, and j.). For Internalizing T score, post hoc analyses showed that a greater proportion of the bisexual/homosexual persisters fell within the clinical range compared to the heterosexual desisters, χ2(1, N = 51) = 5.95, p = .015. The pairwise comparisons between the heterosexual desisters and bisexual/homosexual desisters and between the bisexual/homosexual persisters and bisexual/homosexual desisters were not significant (both ps > .05). For Externalizing T score, there were two significant pairwise comparisons: a smaller proportion of the heterosexual desisters fell within the clinical range compared to the bisexual/homosexual desisters, χ2(1, N = 86) = 3.96, p = .047, and to the bisexual/homosexual persisters, χ2(1, N = 51) = 12.45, p < .001. For the Total T score, only one comparison was significant: a greater proportion of the bisexual/homosexual persisters fell within the clinical range compared to the heterosexual desisters, χ2(1, N = 51) = 5.95, p = .015.
For comparative purposes, the percentage of participants from each group who fell within the clinical range based on Total T score can be compared to data on referred and nonreferred boys from the YSR standardization samples. In the YSR standardization sample, 30% and 9% of referred and nonreferred boys, respectively, fell within the clinical range based on Total T score. Chi-square analyses revealed that the group differences on the YSR were significant, χ2(4) = 34.53, p < .001. Pair-wise comparisons revealed that the percentage of bisexual/homosexual persisters whose total score fell within the clinical range was considerably higher than that in nonreferred boys (both p < .001) but comparable to referred boys (p > .05). The percentage of bisexual/homosexual desisters whose total score was in the clinical range was comparable to that in referred and nonreferred youth (both ps > .05). The percentage of heterosexual desisters whose total score was within the clinical range was lower than that in referred boys (p = .01) but comparable to that in nonreferred boys (p > .05).
3.11 Psychiatric Functioning at Follow-up
Table 22 shows the number of participants with no diagnosis, 1 diagnosis, 2 diagnoses, and 3 or more diagnoses on the Diagnostic Interview Schedule or Diagnostic Interview for Children and Adolescents.
|
Table 22 |
||
|
Number of Psychiatric Diagnoses at Follow-up on the DIS or DICA |
||
|
Number of Diagnoses |
N |
% |
|
0 |
40 |
37.0 |
|
1 |
25 |
23.1 |
|
2 |
18 |
16.7 |
|
3–9 |
25 |
23.2 |
|
Note. Data were only available for participants who completed the face-to-face interview. Of these, data were missing for 2 participants. The number of participants who received 3 or more diagnoses was low so these categories were collapsed. DIS = Diagnostic Interview Schedule (Administered to participants ≥ 18 years of age). DICA = Diagnostic Interview for Children and Adolescents (administered to participants < 18 years of age). |
||
Of the 108 participants for whom data were available, 40 (37%) did not meet criteria for any diagnoses. The remaining 68 (63%) met criteria for at least 1 diagnosis. Of these, 25 (23.1%) met criteria for 1 diagnosis, 18 (16.7%) met criteria for 2 diagnoses, and the remaining 25 participants (23.2%) met criteria for 3 or more diagnoses (range, 3-9 diagnoses). Appendix L provides additional details on the number of diagnoses (and type, where applicable) for each participant.
3.11.1 Psychiatric Functioning at Follow-up as a Function of Gender Identity and Sexual Orientation
Of the 16 bisexual/homosexual persisters, data were available for 15 participants. Of these, 13 (86.6%) met criteria for one or more psychiatric diagnoses at follow-up (other than GID). Of the 66 bisexual/homosexual desisters, data were available for 51 participants. Of these, 41 (80.3%) met criteria for one or more diagnoses. Of the 42 heterosexual desisters, data were available for 37 participants. Of these, 13 (35.1%) met criteria for one or more diagnoses.
Across the three groups, the number of participants administered the Diagnostic Interview Schedule versus the Diagnostic Interview for Children and Adolescents was not evenly distributed. As such, this rendered the total number of diagnoses for each participant potentially misleading. As an alternative to comparing the groups on the mean number of total diagnoses, a proportion score was calculated for each participant and this was used in group analyses. This score reflected the proportion of total possible diagnoses (17 for the Diagnostic Interview Schedule, 13 for the Diagnostic Interview for Children and Adolescents) that the participant obtained. Table 23 shows the means and SD for the proportion score for each group. For descriptive purposes only, Table 23 also shows the mean number of total diagnoses (and SD) according to gender identity and sexual orientation in fantasy.
A one-way ANCOVA (with age at assessment, IQ in childhood, social class, age at follow-up, IQ at follow-up, and marital status[36] co-varied) for Group was significant, F(2, 101) = 6.97, p = .002, partial η2 = .13. Post hoc analyses using lmatrix commands revealed two significant contrasts. The heterosexual desisters, on average, met criteria for fewer diagnoses compared to the bisexual/homosexual desisters (p = .001) and to the bisexual/ homosexual persisters (p = .006). The two bisexual/homosexual groups (i.e., the bisexual/ homosexual persisters and the bisexual/homosexual desisters) did not differ significantly from each other.
|
Table 23 |
|||||||
|
Psychiatric Functioning at Follow-up as a Function of Group |
|||||||
|
|
|
Group |
|
|
|
||
|
Variable |
|
Persisters Bisexual/ Homosexual |
Desisters Bisexual/ Homosexual |
Desisters Heterosexual |
F |
p |
η2 |
|
Number of Diagnoses (Proportion Score)a |
M |
.18 |
.17 |
.03 |
6.97 |
.002 |
.13 |
|
|
SD |
.13 |
.16 |
.05 |
|
|
|
|
|
N |
14 |
51 |
37 |
|
|
|
|
Total Number of Diagnoses |
M |
2.71 |
2.61 |
.49 |
- |
- |
- |
|
|
SD |
2.27 |
2.41 |
.73 |
|
|
|
|
|
N |
14 |
51 |
37 |
|
|
|
|
Note. Dash (-) indicates that an ANCOVA was not conducted on this measure. aAbsolute range, .00-1.00. |
|||||||
3.12.1 Suicidality Questionnaire
Participants’ experience of suicidality was assessed using the Suicidality Questionnaire. The Suicidality Questionnaire was added to the assessment protocol during the third (final) wave of data collection and, therefore, these data were missing for many participants. On this measure, participants reported suicidal thoughts and behaviors since the age of 13 years and in the 12 months preceding the follow-up assessment. Data were available for 48 participants (7 bisexual/homosexual persisters, 31 bisexual/homosexual desisters, and 10 heterosexual desisters). There was no significant difference between participants who completed the suicidality questionnaire and those who did not on any demographic variables (all ps > .05).
Regarding lifetime suicidal thinking/ideation, 8 (16.8%) participants reported that they had sometimes or often thought about suicide; 16 (33.3%) rarely thought about it. The remaining 24 (50%) had not thought about suicide since the age of 13 years. When asked about suicidal thinking in the 12 months preceding the follow-up assessment, 4 (8.3%) participants reported that they had sometimes thought of suicide; 3 (6.3%) rarely thought about it; and 41 (85.4%) never thought about it.
Of the 48 participants who completed the Suicidality Questionnaire, 15 (31.2%) reported that they attempted suicide since the age of 13 years. Of these 15 participants, 3 were bisexual/homosexual persisters, 11 were bisexual/homosexual desisters, and 1 was a heterosexual desister. Of the participants who attempted suicide, 9 reported that the suicide attempt was not related to their gender identity while the remaining 6 reported that it was related to their unhappiness about being a biological male. A one-way ANCOVA for Group was conducted to determine whether the three outcome groups differed significantly on number of suicide attempts since the age of 13.[37] The ANCOVA was significant, F(2, 46) = 4.61, p = .016, partial η2 = .20. Post-hoc analyses using lmatrix command revealed one significant contrast. The bisexual/homosexual desisters reported, on average, a greater number of past suicide attempts compared to the heterosexual desisters (p < .01). There was no significant difference between the bisexual/homosexual persisters and the two desister groups (both ps > .05). The majority (95.8%) of participants had not attempted suicide over the past 12 months; however, 2 (4.2%) participants, both of whom were bisexual/homosexual desisters, reported that they attempted suicide once. Both participants reported that their suicide attempt was not at all related to their gender identity as male.
3.12.2 Self-Report of Suicidality on the Youth Self-Report (YSR)/Adult Self-Report (ASR)
As many of the participants had not completed the Suicidality Questionnaire, suicidality was also measured by examining participants’ responses on two relevant items on the YSR/ASR. These data were only available for participants who completed the face-to-face assessment.
Suicidal ideation was measured by examining participants’ self-report on Item 91 of the YSR/ASR: “I think about killing myself.” Items on the YSR and ASR are rated as 0 (“not true”), 1 (“somewhat or sometimes true”) or 2 (“very true or often true), based on the 6 months preceding the follow-up assessment. Participants’ response on this item was recoded dichotomously,[38] 0 = 0 and 1 or 2 = 1. As shown in Table 24, 46.7% of the bisexual/ homosexual persisters, 19.1% of the bisexual/homosexual desisters, and 11.4% of the heterosexual desisters endorsed that they experienced suicidal ideation in the six months preceding the follow-up assessment. A chi-square analysis revealed that the three groups differed significantly on suicidal ideation, χ2(2, N = 97) = 8.09, p = .018. Pair-wise chi-square revealed one significant comparison: the heterosexual desisters were less likely to endorse this item than the bisexual/homosexual persisters (p < .05). The comparison between the bisexual/homosexual desisters and the bisexual/homosexual persisters approached significance (p = .07).
These results can be compared to standardization data for referred and nonreferred boys in the YSR and ASR standardization samples. In the YSR standardization sample[39], 20% and 7% of referred and nonreferred boys, respectively, endorsed Item 91. In the ASR
|
Table 24 |
||||||||||||||
|
Suicidal Ideation and Behavior at Follow-up as a Function of Group |
||||||||||||||
|
|
Group |
|
|
|||||||||||
|
|
Persisters Bisexual/Homosexual |
Desisters Bisexual/Homosexual |
Desisters Heterosexual |
|
|
|||||||||
|
Variable |
0 |
1 or 2 |
0 |
1 or 2 |
0 |
1 or 2 |
χ2 |
p |
||||||
|
|
N |
% |
N |
% |
N |
% |
N |
% |
N |
% |
N |
% |
|
|
|
YSR Suicidal Ideation |
8 |
53.3 |
7 |
46.7 |
38 |
80.9 |
9 |
19.1 |
31 |
88.6 |
4 |
11.4 |
8.09 |
.018 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
YSR Suicidal Behavior |
9 |
60.0 |
6 |
40.0 |
45 |
95.7 |
2 |
4.3 |
32 |
91.4 |
3 |
8.6 |
14.87 |
.001 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CBCL Suicidal Ideation |
10 |
76.9 |
3 |
23.1 |
42 |
93.3 |
3 |
6.7 |
28 |
84.8 |
5 |
15.2 |
3.01 |
ns |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CBCL Suicidal Behavior |
11 |
84.6 |
2 |
15.4 |
44 |
97.8 |
1 |
2.2 |
30 |
90.9 |
3 |
9.1 |
3.36 |
ns |
|
Note. Suicidal ideation and behavior were assessed using Item 91 and Item18 of the YSR/ASR and CBCL/ABCL, respectively. |
||||||||||||||
standardization sample[40], 28% and 3% of referred and nonreferred boys, respectively, endorsed item 91. Chi-square analyses revealed that the group differences on the YSR and ASR were significant, χ2(4) = 25.46, p < .001 and χ2(4) = 59.83, p < .001, respectively. Pair-wise comparisons revealed that, the bisexual/homosexual persisters were significantly more likely to endorse Item 91 compared to the referred and nonreferred boys in the YSR standardization sample (p = .01 and p < .001, respectively). The bisexual/homosexual persisters were significantly more likely to endorse Item 91 compared to the nonreferred boys in the ASR standardization sample (p < .001) but were comparable to the referred boys. The bisexual/homosexual desisters were more likely to endorse Item 91 compared to the nonreferred boys and in the YSR standardization sample (p = .01) and the ASR standardization sample (p < .001). The bisexual/homosexual desisters were comparable to the referred boys in both the YSR and ASR standardization samples (both ps > .05). The heterosexual desisters were significantly more likely than the nonreferred boys in the ASR standardization sample to endorse Item 91 (p = .01), but less likely than the referred boys (p = .03). However, the heterosexual desisters were comparable to the referred and nonreferred boys in the YSR standardization sample (both ps > .05).
Suicidal behavior was measured by examining participants’ self-report on Item 18 of the YSR/ASR: “I deliberately try to hurt or kill myself.” Similar to the analysis on Item 91 of the YSR/ASR, participants’ responses were recoded dichotomously, 0 = 0 and 1 or 2 = 1. As summarized in Table 24, 40% of the bisexual/homosexual persisters, 4.3% of the bisexual/ homosexual desisters, and 8.6% of the heterosexual desisters reported that they engaged in suicidal behavior in the six months preceding the follow-up assessment. A chi-square analysis revealed that these group differences were significant, χ2(2, N = 97) = 14.87, p =
.001. Pair-wise chi-square analyses revealed two significant comparisons. The bisexual/ homosexual persisters were more likely to endorse this item that the bisexual/homosexual desisters and the heterosexual desisters (both ps < .05).
These results can be compared to standardization data for referred and nonreferred boys in the YSR and ASR standardization samples. In the YSR standardization sample[41], 11% and 2% of referred and nonreferred boys, respectively, endorsed Item 18. In the ASR standardization sample[42], 20% and 7% of referred and nonreferred boys, respectively, endorsed Item 18. Chi-square analyses revealed that the group differences on the ASR and YSR were significant, χ2(4) = 40.93, p < .001 and χ2(4) = 28.62, p < .001, respectively. The results of comparisons varied depending on the standardization sample used in the comparison. The bisexual/homosexual persisters were significantly more likely to endorse this item compared to the referred and nonreferred boys in the YSR standardization sample (both ps < .001) and the ASR standardization sample (p = .006 and p < .001, respectively). The bisexual/homosexual desisters were comparable to the referred and nonreferred boys in the YSR standardization sample (both ps > .05). The bisexual/homosexual desisters were less likely to endorse Item 18 compared to referred boys in the ASR standardization sample (p = .01) but were comparable to the nonreferred boys. The heterosexual desisters were more likely to endorse this item compared to the nonreferred boys in the YSR (p = .005), but were comparable to the referred boys (p > .05). The heterosexual desisters were comparable to the referred and nonreferred boys in the ASR standardization sample (both ps > .05).
Participants’ responses on Item 18 and Item 91 were significantly corrected, r(97) = .68, p < .001.
3.12.3 Parent-Report of Suicidality on the Child Behavioral Checklist (CBCL)/Adult Behavior Checklist (ABCL)
Maternal report of participants’ suicidality was also examined using the CBCL/ABCL. Maternal report of suicidal ideation was measured on Item 91 (“Talking about killing self”) and suicidal behavior was measured on Item 18 (“Deliberately harms self or attempts suicide”). Similar to the coding system utilized for YSR/ASR suicidality items, maternal responses on Items 18 and 91 were recoded dichotomously as 0 = 0 and 1 or 2 = 1. A chi-square analysis revealed that the three groups did not differ significantly on maternal reports of suicidal ideation or suicidal behavior, ps > .05 (Table 24). Across all participants, the correlation between Item 18 and Item 91 on the CBCL/ABCL was significant, r(91) = .53, p < .001.
The extent of agreement between self-report and parent-report of suicidality was examined. For suicidal behavior, the correlation was not significant, p > .05. In contrast, the correlation between self and maternal report of suicidal ideation was significant, r(89) = .38, p < .001.
3.13 Victimization Experiences
The purpose of the victimization questionnaire was to gain a greater understanding of participants’ experiences of victimization related to their gender identity and gender role. The Victimization Survey was added to the assessment protocol during the third (final) wave of data collection and, therefore, these data were missing for participants who were assessed prior to 2008. On this measure, participants rated the frequency with which they experienced three types of verbal victimization and four types of physical victimization since the age of 13 years (also referred to as lifetime victimization) and in the 12 months preceding the follow-up assessment. Data were available for 48 participants (7 bisexual/homosexual persisters, 31 bisexual/homosexual desisters, and 10 heterosexual desisters). There was no significant difference between participants for whom victimization data were available and those where data were not available on any demographic variables (all ps > .05).
3.13.1 Descriptive Victimization Experiences for the Entire Sample
Of the 48 participants for whom data were available, 30 (62.5%) had experienced some type of victimization since the age of 13-years-old/in their lifetime related to their gender identity.[43]
Of the 48 participants, 29 (60.4%) had experienced some type of verbal victimization (e.g., verbal insults, threats to tell others about gender identity, threat of violence) in their lifetime (Table 25). Verbal insults were experienced more often than both threats to tell others about their gender identity and threat of a physical attack; 29 (60.4%) participants had experienced a verbal insult related to their gender identity at least once in their life, 16 (33.3%) experienced a threat of violence, and 10 (20.8%) were threatened by others to have their gender identity disclosed.
As shown in Table 25, for all types of verbal victimization (insults and threats), it was more common for participants to have experienced 3 or more episodes of victimization than a single episode. Based on the 12 months prior to the follow-up assessment, 19 (39.6%) participants had experienced at least one type of verbal victimization. Of the 48 participants, 19 (39.6%) had experienced verbal insults in the past 12 months, 8 (16.7%) experience a threat of violence, and 5 (10.5%) were threatened by others to have their gender identity disclosed.
|
Table 25 |
||||||||||||||||
|
Gender Identity-Related Victimization |
||||||||||||||||
|
|
Frequency of Victimization |
|||||||||||||||
|
|
Past 12 months |
Since the age of 13 years/lifetime |
||||||||||||||
|
|
0 |
1 |
2 |
≥3 |
0 |
1 |
2 |
≥3 |
||||||||
|
Type of victimization |
N |
% |
N |
% |
N |
% |
N |
% |
N |
% |
N |
% |
N |
% |
N |
% |
|
Verbal victimization |
||||||||||||||||
|
Verbal insults |
29 |
60.4 |
0 |
0 |
7 |
14.6 |
12 |
25.0 |
19 |
39.6 |
3 |
6.3 |
2 |
4.2 |
24 |
50.0 |
|
Threats of violence |
43 |
89.6 |
3 |
6.3 |
2 |
4.2 |
0 |
0 |
38 |
79.2 |
2 |
4.2 |
3 |
6.3 |
5 |
10.4 |
|
Threat of disclosure |
40 |
83.3 |
3 |
6.3 |
4 |
8.3 |
1 |
2.1 |
32 |
66.7 |
5 |
10.4 |
1 |
2.1 |
10 |
20.8 |
|
Physical victimization |
||||||||||||||||
|
Object thrown |
38 |
79.2 |
8 |
16.7 |
1 |
2.1 |
1 |
2.1 |
28 |
59.3 |
6 |
12.5 |
3 |
6.3 |
11 |
22.9 |
|
Physical assault |
44 |
91.7 |
4 |
8.3 |
0 |
0 |
0 |
0 |
36 |
75.0 |
6 |
12.5 |
2 |
4.2 |
4 |
8.3 |
|
Threat with a weapon |
47 |
97.9 |
0 |
0 |
0 |
0 |
1 |
2.1 |
42 |
87.5 |
4 |
8.3 |
1 |
2.1 |
1 |
2.1 |
|
Sexual assault |
47 |
97.9 |
1 |
2.1 |
0 |
0 |
0 |
0 |
44 |
91.7 |
3 |
6.3 |
1 |
2.1 |
0 |
0 |
|
Note. Data were available for 48 participants (7 bisexual/homosexual persisters, 31 bisexual/homosexual desisters, and 10 heterosexual desisters). For frequency of Victimization: 0 = Never, 1 = Once, 2 = Twice, ≥3 = 3 or more times |
||||||||||||||||
Of the 48 participants who completed the Victimization Survey, 22 (45.8%) had experienced at least one type of physical victimization (objects thrown at them, being punched/ kicked/beaten, threatened with a weapon, sexually attacked) since the age of 13-years-old (Table 25). The most commonly experienced type of physical victimization was having an object thrown at them; 20 (41.7%) participants had an object thrown at them at least once, 12 (25%) had been physically attacked (punched, beaten, kicked), 6 (22.5%) were threatened with weapons, and 4 (8.4%) were sexually assaulted. Across the four types of
physical victimization reported on, a report of one episode of physical victimization was generally more common than a report of multiple episodes. Based on the 12 months prior to the follow-up assessment, 11 (22.9%) participants had experienced at least one type of physical victimization. Of the 48 participants, 10 (20.8%) had an object thrown at them, 4 (8.3%) were physically attacked, 1 (2.1%) was threatened with weapons, and 1 (2.1%) was sexually attacked.
Visual inspection of the data with regard to the location of the victimization incidents revealed that they most commonly occurred at school or in the neighborhood. The most common assailants were strangers and peers.
3.13.2 Victimization Experiences as a Function of Sexual Orientation in Fantasy
For each participant, a mean score was calculated for verbal victimization, physical
victimization, and overall victimization (verbal and physical combined) based on the frequency of occurrence of victimization experiences in the past 12 months. Mean scores were also calculated for frequency of victimization since the age of 13 years. In total, six mean scores were calculated for each participant (Table 26).
|
Table 26 |
|||||||
|
Mean Frequency of Victimization as a Function of Gender Identity and Sexual Orientation in Fantasy |
|||||||
|
|
|
Group |
|
|
|
||
|
Variable |
|
Persisters Bisexual/ Homosexual (n = 7) |
Desisters Bisexual/ Homosexual (n = 30) |
Desisters Heterosexual
(n = 10) |
F |
p |
η2 |
|
Since the age of 13 years |
|||||||
|
Verbal Victimizationa |
M |
1.76 |
.92 |
.47 |
3.46 |
.042 |
.15 |
|
|
SD |
1.07 |
1.05 |
.61 |
|
|
|
|
Physical Victimizationb |
M |
1.07 |
.37 |
.18 |
4.60 |
.016 |
.20 |
|
|
SD |
.83 |
.57 |
.33 |
|
|
|
|
Overall Victimizationc |
M |
1.37 |
.60 |
.30 |
4.25 |
.022 |
.18 |
|
|
SD |
.87 |
.75 |
.42 |
|
|
|
|
Past 12 months |
|||||||
|
Verbal Victimizationa |
M |
1.38 |
.39 |
.23 |
6.38 |
.004 |
.25 |
|
|
SD |
.91 |
.58 |
.50 |
|
|
|
|
Physical Victimizationb |
M |
.50 |
.06 |
.00 |
7.21 |
.002 |
.27 |
|
|
SD |
.72 |
.11 |
.00 |
|
|
|
|
Overall Victimizationc |
M |
.88 |
.20 |
.10 |
8.89 |
.001 |
.31 |
|
|
SD |
.76 |
.27 |
.21 |
|
|
|
|
Note. Absolute range for mean frequency scores, 0-4. aCalculated as: (sum of frequency of each type of verbal victimization)/3 bCalculated as: (sum of frequency of each type of physical victimization)/4 cCalculated as: (sum of frequency of all type of verbal victimization)/7 |
|||||||
A series of one-way ANCOVAs (with age at assessment, age at follow-up, IQ in childhood, IQ at follow-up, social class, and marital status covaried) were conducted to determine whether the three outcome groups differed on mean frequency for verbal, physical and total victimization experiences since the age of 13 years. There was a significant main effect for Group on all three variables. The significant ANCOVAs were followed up with post-hoc analyses using lmatrix commands. For mean verbal victimization since the age of 13 years, there was one significant post hoc contrast: the bisexual/homosexual persisters had experienced, on average, significantly more victimization than the heterosexual desisters (p < .05). For mean physical victimization since the age of 13 years, the bisexual/homosexual persisters had experienced, on average, significantly more physical victimization than both the bisexual/homosexual desisters and the heterosexual desisters (both ps > .05). Not surprisingly, the groups also differed on their mean overall victimization scores for which two contrasts were significant: the bisexual/homosexual persisters reported, on average, significantly more victimization than both the bisexual/homosexual desisters (p = .05) and the heterosexual desisters (p = .006).
The above-described ANCOVAs were repeated to examine whether the groups differed in their victimization experiences (verbal, physical, and total) based on the 12 months preceding the follow-up interview. There was a significant main effect for Group on all three measures. The significant ANCOVAs were followed up with post-hoc analyses using lmatrix commands. For mean verbal victimization, mean physical victimization, and mean overall victimization in the 12 months preceding the follow-up assessment, bisexual/ homosexual persisters reported, on average, significantly more victimization than both the bisexual/homosexual desisters and the heterosexual desisters (all ps < .01). The bisexual/ homosexual desisters and heterosexual desisters did not significantly differ on any of the measures.
3.13.3 Victimization and Mental Health
Although not a focus of the follow-up study, the relationship between participants’ overall mean score on the victimization survey and their mental health functioning was examined. Participants’ Internalizing T score, Externalizing T score, and Total Problems T score on the Youth Self Report (YSR) or Adult Self Report (ASR) at follow-up was correlated with their mean overall victimization score for the past 12 months.[44] Participants’ overall victimization score was significantly correlated with their Externalizing T score, r(46) = .34, p < .05, and their Total Problems T Score, r(46) = .33, p < .05. The correlation between overall victimization score and Internalizing T score was not significant (p > .05).
The relationship between participants’ mean overall victimization score and psychiatric diagnosis on the DIS/DICA, using the proportion score, was also examined. The correlation was not statistically significant, r(47) = .20, p > .05.
3.13.4 Victimization and Childhood Sex-Typed Behavior
Using the overall mean victimization scores, the relationship between participants’ victimization experience and their childhood cross-gender behaviors was examined. Two sets of correlation analyses were conducted. First, participants’ overall mean overall victimization score since the age of 13 years old (i.e., lifetime victimization) was correlated with their scores on the nine measures of childhood sex-typed behavior (see Table 16, for example, for a list of these measures). None of the correlations were significant (all ps > .05). Second, participants overall mean victimization score for the 12 months preceding the follow-up assessment was correlated with their scores on the nine measures of childhood sex-typed behavior. There was only one significant correlation. Participants’ victimization experiences were significantly correlated with parent-report of their childhood cross-gender behavior on the Gender Identity Questionnaire for Children, r(46) = -.39, p < .01.
3.13.5 Victimization and Parent-Report of Concurrent Gender Role Behavior
Participants overall mean victimization scores, for both lifetime (since the age of 13 years old) and the 12 months preceding the follow-up assessment was correlated with their score on the parent report Gender Identity/Gender Role Questionnaire for Adolescents, a measure of concurrent gender role behaviors. Participants’ overall victimization score since the age of 13 years old was significantly correlated with their parents’ report of their concurrent cross-gender behaviors, r(42) = -.43, p < .01. Similar results were obtained when the relationship between victimization in the 12 months preceding the follow-up assessment and parent-report of concurrent gender role was examined, r(42) = -.59, p < .001.
3.14 Comparisons with Other Follow-up Studies of boys with Gender Identity Disorder
3.14.1Persistence Rates across Follow-up Studies of Boys with Gender Identity Disorder
Appendix M summarizes the persistence rate obtained in follow-up studies of boys with GID. Chi-square analysis revealed that the rates of persistent gender dysphoria across this study, Green (1987), and Wallien and Cohen-Kettenis (2008)[45] differed significantly, χ2(2) = 14.30, p = .001. Pair-wise comparisons showed a significant difference in persistence rates between the Green and Wallien and Cohen-Kettenis studies, χ2(1) = 12.31, p < .001, and between the present study and Wallien and Cohen-Kettenis, χ2(1) = 7.22, p < .01. The comparison between the present study and Green approached significance, χ2(1) = 3.73, p = .05.
In Drummond et al.’s (2008) follow-up study of females with GID, 3 of the 25 participants were classified as persisters and the remaining 22 were desisters. When combined with the boys from the present study, there was a total of 20 persisters and 144 desisters and a persistence rate of 12.1% for the Toronto sample of boys and girls. Wallien and Cohen-Kettenis reported a persistence rate of 27% for their entire sample of males and females (21 persisters, 56 desisters). However, this calculation included 23 participants who could not be traced/contacted at follow-up but were assumed to be desisters. If a more conservative rate was calculated by excluding these 23 individuals, the persistence rate was 38.8%.
Chi-square analyses were used to compare the results of the combined Toronto sample with that of the combined males and females in the study by Wallien and Cohen-Kettenis (2008). Regardless of whether one used the conservative or liberal persistence rates from Wallien and Cohen-Kettenis’ (2008) study, the rates of persistent gender dysphoria across the two clinics varied significantly, χ2(1) = 18.96, p < .001 and χ2(1) = 8.43, p = .004, respectively.
3.14.2 Threshold vs. Sub-threshold for Gender Identity Disorder in Childhood
In the present study, 88 (63.3%) of the 139 participants met diagnostic criteria for GID in childhood and the remaining 51 (36.7%) were subthreshold for the diagnosis. In the follow-up study by Wallien and Cohen-Kettenis (2008), 44 (74.5%) of the 59 boys met the full criteria for GID in childhood and the remaining 15 (25.5%) were sub-threshold for the diagnosis. There was no significant difference in the percentage of boys who met full criteria for GID across the two studies, χ2(1) = 2.36, p > .05.
Chapter 4
Discussion
The present study represents the largest sample to date of clinic-referred boys with Gender Identity Disorder (GID) followed into adolescence and adulthood. The goals of the study were to examine gender identity, sexual orientation, and general psychiatric outcomes at follow-up. The findings related to gender identity and sexual orientation outcomes are discussed first followed by behavioral and psychiatric functioning. The key findings of the study were as follows: (1) the most common long-term outcome for boys with GID was desistence of gender dysphoria a with co-occurring homosexual sexual orientation, (2) the percentage of boys with persistent gender dysphoria was modest but significantly higher than the base rate of GID in the general population of biological males, (3) the percentage of boys who developed a bisexual/homosexual sexual orientation was much higher than the base rates of bisexual/homosexual sexual orientation in adult males in the general population, (4) social class and severity of cross-gender behavior in childhood were significant predictors of gender identity outcome at follow-up, (5) severity of childhood cross-gender behavior was a significant predictor of sexual orientation at follow-up, and (6) the heterosexual desisters reported significantly less behavioral and psychiatric difficulties compared to the bisexual/ homosexual persisters and, to a lesser extent, the bisexual/homosexual desisters.
4.1 Representativeness of Sample and Participation Rate
Before providing an analysis of the findings, a comment on the representativeness of the sample should be made since differences between participants and non-participants can threaten the internal validity of a study (Campbell & Stanley, 1963). More than half of the patients who were identified as eligible to participate in the study were not recruited due to time and financial constraints. Comparisons between the participants and these non-participants on demographic variables, behavior problems, and sex-typed behavior yielded minimal group differences: only 1 of the 17 comparisons was significant. At least based on these measures, the boys who participated in the study did not appear to differ substantially from those who were eligible to participate but were not recruited. The study participants were also compared to the cases where the families could not be traced and to the cases where either the parent or potential participant himself refused. The group differences were modest: one comparison (IQ) approached significance and a second comparison (marital status) was significant. Regarding the latter, participants were more likely to originate in a two-parent family while the cases that could not be traced were more likely to come from a family composition other than two parent (e.g., divorced, living with relatives). This finding is not surprising in the context of research which shows that single-parent families move considerably more often than two-parent families (e.g., McLanahan & Sandefur, 1994). Based on these comparisons, the 139 participants who agreed to participate appeared to be representative of the total pool of available patients and did not constitute a biased sample at follow-up.
The participation rate in this study was 95.9% of those who could be traced,[46] which is extremely high especially given that the mean duration between childhood assessment and follow-up was 12.88 years. This participation rate was higher than Drummond et al.’s (2008) follow-up study of girls (83.3%) but lower than Wallien and Cohen-Kettenis’ (2008) follow-up study of boys and girls (100% of those who could be traced).
4.2 Recollection of Childhood Cross-Gender Behaviors
In using a prospective design, this study was not reliant on participants’ retrospective reporting of their childhood sex-typed behavior; however, the methodology did include a measure of recalled childhood cross-gender behaviors. While most of the participants in the present study no longer met criteria for GID, their recollections of sex-typed behavior in childhood was similar to the childhood recollections of biological males with GID assessed for the first time in adolescence and adulthood. Further, the participants recalled more cross-gender behaviors than adolescent and adult males referred for clinical reasons other than gender identity concerns (Singh et al., 2010).
Retrospective analysis of childhood sex-typed behaviors has been criticized on numerous grounds. In studies that examine the childhoods of adults with GID who present to specialized gender identity clinics, there may be a selection bias because they may not represent all individuals with GID (Drummond et al., 2008). For example, individuals who meet criteria for GID in childhood but show a desistence of their gender dysphoria in adolescence or adulthood would not be seen in a gender clinic because they no longer seek gender change. Thus, adults with GID seen in specialized gender clinics may be more representative of persisters rather than desisters. Beyond the potential for general distortion in memory than can occur with the passage of time (Hardt & Rutter, 2004), studies that have retrospectively examined the childhoods of heterosexual and homosexual adults have faced a more specific criticism related to selective retention/construction of experiences. It has been argued that the greater recollection of childhood cross-gender behaviors by homosexual compared to heterosexual adults reflects an attempt by these individuals to reconstruct a childhood that fits with current Western culture’s belief that the childhoods of homosexual adults is gender nonconforming (e.g., Gottschalk, 2003; Hoult, 1983/1984). In other words, they recall a childhood pattern of sex-typed behaviors that is aligned with beliefs about homosexual individuals so as to appear similar to them. Using this reasoning, one can also assert that children with GID who develop a heterosexual sexual orientation in adulthood might provide a narrative of their childhood sex-typed behaviors that is consistent with a masculine childhood, especially if their cross-gender behaviors caused them embarrassment or peer rejection.
Results of the present study did not support a retrospective distortion hypothesis. Participants’ adult recollections of their childhood cross-gender behavior correlated significantly with four of seven measures of sex-typed behaviors in childhood, including one parent report and three self-report. Their recollections of how cross-gendered they were as children were comparable to their actual extent of cross-gendered behaviors in childhood. Thus, in contrast to the criticism of retrospective designs, the participants in this study, which included homosexual and heterosexual men, were generally not biased or selective in their recall. That participants recalled a cross-gendered childhood is consistent with a large body of research that has retrospectively examined childhood sex-typed behaviors of heterosexual and homosexual men (for a meta-analysis, see Bailey & Zucker, 1995), including studies that have utilized home videos (e.g., Rieger et al., 2008) and parent report (e.g., Bailey, Miller, & Willerman, 1993; Bailey, Nothnagel, & Wolfe, 1995; Bailey, Willerman, & Parks, 1991) in an attempt to reduce bias in recall. Given the findings across these studies, it is unlikely that inaccurate recollection of their childhood (i.e., retrospective distortion) accounts for the large and consistent differences in the childhood sex-typed behaviors between homosexual and heterosexual men.
4.3 GID Diagnosis in Childhood
The majority (63.3%) of boys in this study met complete diagnostic criteria for GID in childhood. The boys who did not meet the complete criteria showed some characteristics of cross-gender identification and some, based on the history provided by their parents, would have met full criteria had they been assessed earlier in development. Therefore, it is not likely that the subthreshold cases represented grossly false positives or inappropriate referrals. As an example, one participant who was assessed when he was 11-years-old and was subthreshold for GID exhibited a fair amount of cross-gender behavior (e.g., always chose female roles in role-play and usually used girls’ clothing in dress-up play). He also showed some signs of cross-gender identification on psychological testing (e.g., his first drawn person on the Draw-a-Person task was a female, when asked if it would be better to be a boy or a girl he said “I don’t know, in the middle I guess,” and said he “sometimes” thinks he would like to be a girl). At the same time, he also had a moderate degree of same-gender role behavior, had not made explicit remarks of wanting to be a girl (according to parents), preferred boys and girls equally as peers, and played with male-typical and female-typical dolls with equal frequency. On psychological testing, this youngster indicated that there were some good things about being a boy but could not list any of them.
In the Toronto clinic, false positives almost never occur and about 70% of the children evaluated meet the full criteria for GID, which is similar to the percentage of threshold cases in the present follow-up sample (Zucker, 2010a). There appears to be variance in the cross-gender presentation of children referred to the Toronto clinic, with some meeting full criteria and some not, and this may be reflective of the apparent gender variance spectrum that is witnessed in this population of children. A number of adolescents who present to the Toronto clinic seem to have only met the full diagnostic criteria for GID sometime in adolescence and, based on historical information provided, might have been subthreshold for GID in childhood.
Comparative analysis of the threshold and subthreshold cases revealed a number of significant differences between the groups. There was a relationship between age and diagnostic status in childhood. The boys who met full criteria for GID in childhood were significantly younger at the time of the childhood assessment than those who were subthreshold for the diagnosis. This finding could not be directly compared with other follow-up studies of boys with GID because requisite data from those studies were not available. However, there are clues that this finding represents a pattern in children with GID. Research using the DSM-III and DSM-III-R criteria found that younger children (under 7 years of age) were more likely to receive the diagnosis than were older children (Zucker, 1992). This appeared to be related to the fact that older children were less likely than younger children to verbalize their desire to be of the opposite gender, which was required for the diagnosis to be made. Fear of stigma and social desirability pressures may have been operating on these children. Clinical impression from assessing and treating older children with GID suggests that some children also attempt to conceal some of their cross-gender behaviors.
It is not surprising that, even with age at childhood assessment controlled for, the boys who met criteria for GID in childhood also showed more severe cross-gender behavior (or less same-gender behavior) on parent and self-report measures of sex-typed behavior than those who were subthreshold for the diagnosis. Similar differences were found between threshold and subthreshold cases of gender-referred children in the Netherlands: the threshold cases were reported by parents as more severe in their cross-gendered behaviors compared to the subthreshold cases (Cohen-Kettenis et al., 2006). This difference between threshold and subthreshold cases may be reflecting a natural history of GID for some children whereby cross-gender identification and behaviors lessen over time. This is plausible given that some of the subthreshold cases would have met criteria for GID had they been assessed earlier in development. On the other hand, the subthreshold cases were, on average, older than the threshold cases; thus, differences in severity may be an artifact of social desirability, as discussed above. There are other factors that may also contribute to the relationship between age, diagnostic status, and symptom severity. For example, parental efforts to treat the condition even prior to the clinical assessment might have affected their child’s gender identity development and resulted in a decrease in cross-gender behaviors and identification.
The subthreshold participants had more externalizing difficulties than the threshold participants. This may be related to the observed relationship between age and behavior problems in children with GID with older children showing more behavioral problems than younger children (Cohen-Kettenis et al., 2003). One hypothesis for this is that poorer peer relations in older children may be mediating the relationship between age and behavior problems (Zucker, 2005c).
4.4 Gender Identity and Sexual Orientation
4.4.1 Gender identity outcome
4.4.1.1 Rate of persistent gender dysphoria
The present study found that the majority of boys with GID showed desistence of their gender dysphoria when followed into adolescence and adulthood: 87.8% of the boys did not report any distress about their gender identity at follow-up and were happy living as males. When persistence rate was examined as a function of GID diagnostic status (i.e., threshold vs. subthreshold) in childhood, there was no significant difference in the rates obtained for the two diagnostic groups. The two childhood diagnostic subgroups did not show significant differences in their developmental trajectories, at least in regard to persistence of gender dysphoria. In this study, the categorical diagnosis of GID itself was, therefore, not a good prognosticator of persistence/desistence of GID over time. This is in contrast to the follow-up study by Wallien and Cohen-Kettenis (2008) where all of the persisters met full criteria for GID in childhood compared to approximately half of the desisters; thus, persistence rate of gender dysphoria would have varied significantly for the threshold and sub-threshold groups.
Although across the present study and those by Green (1987) and Wallien and Cohen-Kettenis (2008) the majority of boys with GID no longer had GID in adolescence or adulthood, there was significant variability in the persistence rates obtained across the studies with a range of 2.3%-30%. The persistence rate of 12.2%[47] in the present study fell in between that obtained by Green and Wallien and Cohen-Kettenis, but was closer to the rate of 9.1% calculated by Zucker and Bradley (1995) in their summary of six follow-up studies of boys with GID. Possible explanations for this variability are discussed later.
4.4.2 Sexual orientation outcome.
4.4.2.1 Rate of Bisexual/Homosexual Sexual Orientation
Information on sexual fantasy and behaviors in the 12-month period preceding the follow-up assessment was obtained during a face-to-face semi-structured interview, from which Kinsey ratings were assigned. The correlation between these two metrics of sexual orientation was very strong. One has to be cautious about the possibility that participants may have underreported a minority sexual orientation due to social desirability pressures; however, there was no significant relationship between sexual orientation and the propensity to give socially desirable responses on the measure of social desirability. It is recognized that these results do not directly confirm whether there was an underreporting of bisexual/ homosexual fantasies and can only speak to group differences in social desirability.
Regarding sexual orientation in fantasy,[48] 63.6% of participants were classified as bisexual/homosexual at follow-up. The rate of a bisexual/homosexual outcome obtained in the present sample was similar to that obtained by Green (1987) and Wallien and Cohen-Kettenis (2008), 75% and 81%, respectively. Across these follow-up studies, the percentage of males with a bisexual/homosexual outcome was, therefore, greater than the percentage of males with a heterosexual outcome. These results were also similar to that obtained by Zucker and Bradley (1995) in their summary of six follow-up studies of boys with gender dysphoria: In the combined sample, 61.9% of males reported a bisexual/homosexual orientation at follow-up; however, it is unclear whether this was based on sexual fantasy or sexual behavior. In contrast to these results for biological males with gender dysphoria, all of the control boys in Green’s (1987) study were classified as heterosexual at follow-up.
In contrast to the low rate of persistent GID in this study, the rate of bisexuality/ homosexuality was very high and it represented the most common sexual orientation outcome for boys with GID. The percentage of participants in the present study who reported a bisexual/homosexual sexual orientation (63.6%) was substantially higher than the currently accepted base rate of a homosexual sexual orientation in males of 3.1% (Laumann, Gagnon, Michael, & Michaels, 1994).
4.4.2.2 Sexual Orientation of Persisters
All but one of the persisters in the present study reported a bisexual/homosexual sexual orientation at follow-up. Only one persister reported a heterosexual sexual orientation. Similarly, in the follow-up studies summarized by Zucker and Bradley (1995) and in Green’s (1987) study, all persisters reported a homosexual sexual orientation. In contrast, Wallien and Cohen-Kettenis (2008) reported that 83% of the male persisters in their sample were bisexual/homosexual. Wallien and Cohen-Kettenis hypothesized that some of the participants who reported a heterosexual sexual orientation may move toward a bisexual/homosexual sexual orientation later on. This was based on the observation that some participants reported different sexual orientations across the metrics of fantasy, behavior, and attraction. Thus, it may be possible that these individuals had not yet developed a consolidated sexual identity and may have been experimenting with their sexual identity. As well, Wallien and Cohen-Kettenis did not measure participants’ propensity to give socially desirable responses; therefore, it remains unknown whether there was also an underreporting of bisexual/ homosexual sexual orientation in their sample, a limitation that they noted.
4.4.2.3 Age and Sexual Orientation
Approximately one-third of the present sample reported a heterosexual sexual orientation and these males were significantly younger than the bisexual/homosexual participants at follow-up. The age difference between the desisting bisexual/homosexual participants and the desisting heterosexual participants may be related to the timing of “coming out.”[49] Decades of research on “coming out” as gay or homosexual have shown that the period of first disclosure can range from mid-adolescence, around 16 or 17 years of age (e.g., D’Augelli, Hershberger, & Pilkington, 1998; Grov, Bimbi, Nanin, & Parson, 2006; Newman & Muzzonigro, 1993), to late adolescence and early 20s (e.g., Barber, 2000; Herek, Cogan, Gillis, & Glunt, 1998; McDonald, 1982; Savin-Williams, 1998; Savin-Williams & Ream, 2003). It is possible that some of the heterosexual males, if followed up later in their adult life, will continue to identify as heterosexual while others may disclose a bisexual or homosexual identity. Indeed, the literature on sexual identity development of gay and bisexual youth has shown that there can be change in identity over time and this may be related to the stages of the “coming out” process (e.g., Lever, 1994; Rosario, Schrimshaw, & Hunter, 2008; Rosario, Schrimshaw, Hunter, & Braun, 2006; Stokes, Damon, & McKirnan, 1997). In Green’s (1987) study, which included multiple follow-up assessments between childhood and adulthood, there was a shifting in sexual identity over the course of follow-up for some participants (e.g., one male identified as heterosexual at age 15, bisexual at age 16, and homosexual at age 20). We do not know, however, what factors contributed to the change in reported sexual identity. It is unclear, for example, if this shift represented a bona fide change in the participants’ sexual identity or whether there may have been other factors, such as social desirability, which rendered the participant unwilling to disclose their homosexual sexual identity as the earlier assessment conducted when he was 15-years-old.
4.4.3 Multiple Long-term Psychosexual Outcomes for Boys with GID
With gender identity and sexual orientation outcomes combined, there were diverse developmental outcomes for boys with GID, three of which were primary: (1) persistence of GID with a bisexual/homosexual sexual orientation, (2) desistence of GID with a bisexual/ homosexual sexual orientation, and (3) desistence of GID with a heterosexual sexual orientation. The fourth outcome, persistence of GID with heterosexual sexual orientation, was least common and seen in only one participant. Most of the boys in this study no longer experienced gender dysphoria when followed into adolescence and adulthood, which is consistent with findings from previous follow-up studies. Thus, GID in childhood appears to be more strongly associated with a desisting homosexual outcome rather than a transsexual outcome. The observed variation in the long-term psychosexual outcome of boys with GID suggests that biological reductionist accounts of psychosexual development are too simplistic. These results did not support the view that GID in childhood is isomorphic with homosexuality in adulthood. Predictors of this observed variability are subsequently discussed.
4.5 Predictors of Gender Identity Outcome
The long-term psychosexual outcome for boys with GID can be encapsulated by the principle of multifinality from the developmental psychopathology literature (i.e., multiple long-term outcomes from a common starting point in childhood–gender dysphoria). That there are multiple long-term outcomes for boys with GID raises a number of questions, one of which is whether there are childhood features that distinguish between the boys who will persist in their gender dysphoria from those who will desist. In the present study, the sample size was large enough to examine whether demographic variables, sex-typed behavior, or behavior problems in childhood could predict group outcome at follow-up.
4.5.1 Demographic Predictors of Gender Identity Outcome
Of the childhood demographic variables collected, the outcome groups[50] differed on age at childhood assessment, IQ, social class, and marital status. The persisters were older at the childhood assessment, had a lower IQ, and were more likely to come from a lower social class, single parent-household compared to both desister groups. In a regression model,[51] however, social class was the only significant demographic predictor of group outcome at follow-up and, thus, is the focus of the current discussion.
4.5.1.1 Social Class
The persisters were at increased odds of coming from a lower social class background compared to the desisters. However, within the two groups of desisters, social class did not predict outcome at follow-up. Thus, in this sample of boys with GID, social class was a predictor of gender identity outcome, but not of sexual orientation outcome per se. These results cannot be compared to previous follow-up studies as social class data were not published. There are a number of potential explanations for the relationship between social class and persistence of gender dysphoria such that social class may be a proxy for a number of factors, including familial stress, parental psychopathology, peer relations, attitudes towards effeminate gay men, and attitudes towards homosexuality, each of which is subsequently discussed.
In the literature on adult homosexual and non-homosexual male-to-female transsexuals, there has been a long-standing observation that these individuals, on average, seem to grow up within families of low socioeconomic status (e.g., Hoenig, Kenna, & Youd, 1970; MacFarlane, 1984). The association between male-to-female transsexualism and sexwork (a correlate of socioeconomic status) has also been examined. A recent study of 573 self-identified adult transsexuals, for example, found that more than 50% had done some type of sexwork in the preceding 6 months (Nemoto, Bödeker, & Iwamoto, 2011). From these data, it is unclear whether low socioeconomic status was implicated in the etiology and development of transsexualism or whether it was secondary to possible social struggles and economic discrimination experienced by these individuals.
4.5.1.1.1 Familial Stress and Parental Psychopathology
Socioeconomic status (SES) or social class has a long-standing history in the child development literature as a risk factor for negative outcomes, with numerous studies demonstrating the association between poverty, for example, and increased risk for mental health problems in children (for a summary, see Jenkins, 2008). In the child development literature, social class has been conceptualized as a proxy or marker for access to resources and experiences that may be related to or associated with socioeconomic status (Bradley & Corwyn, 2002). For example, numerous studies have shown that low SES families experience, on average, significantly more stress compared to high SES families due to more destabilizing events, such as family dissolution and moves (e.g., Gad & Johnson, 1980).
Though speculative, it may be that low social class is a risk factor for persistent gender dysphoria due to the associated stress in these families. Parents who are experiencing significant stressors may be overwhelmed by these difficulties, feel depleted themselves, and, thus, are unable to work on interventions aimed at resolving their child’s gender identity issues (Zucker et al., 2012b). One can imagine that, if a family is burdened with economic hardship, there may be less financial resources to dedicate to addressing the child’s gender identity issues. A consistent finding in psychiatric research has been the negative relationship between SES and mental disorder–the lower the SES of an individual, the higher is his or her risk for developing a mental disorder (e.g., Hollingshead & Redlich, 1958; Hudson, 1988, 2005). It may be that the parents of persisters were also struggling with significant psychopathology that interfered with their parenting role and this contributed to the perpetuation of their child’s gender dysphoria. Data on parental psychopathology at the time of the childhood assessment were not analyzed as they were not the focus of the present study. Therefore, it remains unknown whether parents of persisters had more psychopathology compared to parents of the desisters. Zucker and Bradley (1995) reported that mothers of boys with GID were more impaired in their emotional functioning compared to mothers of normal control boys but were generally as impaired as mothers of clinical control boys.
4.5.1.1.2 Quality of Peer Relationships
Social class may also be operating on the quality of peer relations in the study participants. Peer relations are an important aspect of children’s well-being in general (for a review, see Parker, Rubin, Price, & DeRosier, 1995) and, more specifically, relations with same-sex peers play an important role in children’s gender identity development and consolidation (Maccoby, 1998). Thus, for children with GID, developing and expanding the breadth of same-sex peer relations with temperamentally compatible peers has been encouraged (e.g., Meyer-Bahlburg, 2002; Zucker et al., 2012b). Studies have shown that children with GID have more peer relationship difficulties than their siblings and non-GID peers (e.g., Cohen-Kettenis et al., 2003; Zucker, Bradley, & Sanikhani, 1997). There is some evidence that children from low SES families may be more isolated from peers and experience less peer companionship overall compared to their high SES counterparts (Patterson, Vaden, Griesler, & Kupersmidt, 1991). It is possible that boys with GID who were also from a low SES may have had even fewer opportunities for using their peers for gender identity consolidation and, therefore, were at an increased risk for persistence of cross-gender identification compared to boys with GID from a higher social class background. In the present, sample, however, there was no significant difference between the outcome groups on the quality of their childhood peer relations, measured using two items from the Child Behavior Checklist. It is possible that our crude measure of childhood peer relations was not sufficient to capture differences between the groups on quality of their relationships, if differences did exist.
4.5.1.1.3 Attitudes towards Homosexuality
The stereotypical gay man in Western culture is feminine in a number of respects, including his mannerisms, interests, and occupation; however, there is variation in the extent of femininity seen in homosexual men (Bailey & Pillard, 1991; Rieger, Linsenmeier, Gygax, Garcia, & Bailey, 2010). An inverse relationship between social class and effeminacy in adult gay men has been reported, such that more stereotypical/effeminate behaviors are seen in gay men from a lower social class background compared to gay men from a higher social class (e.g., Farrell & Morrione, 1974). Given that a large proportion of gay men engaged in cross-gendered behaviors in childhood, a process of defeminization (Whitam, 1977) occurred in some gay men between childhood and adulthood while, in others, cross-gender behaviors persisted. Harry (1985b) speculated that defeminization (i.e., discontinuation in cross-gender behaviors) may be related to social class such that it is more likely to occur among gay males from middle-class backgrounds than among males from working-class families, and found support for this hypothesis in a retrospective study of 686 male homosexuals. There was greater continuation of cross-gender behaviors among adult gay men raised in blue-collar households than those raised in middle-class/white-color households.
In the present study, the least amount of defeminization (i.e., persistence of cross-gender behaviors) did occur in boys from a lower social class while the most defeminization (i.e., desistence) occurred in boys from a higher social class. The relationship between social class and persistent gender dysphoria may be related to attitudes of gay men towards effeminacy in other gay men. Gay men, particularly those who view themselves as masculine, prefer men who describe themselves as masculine rather than feminine (Bailey, Kim, Hills, & Linsenmeier, 1997; Taywadietp, 2001). It is possible that males with persistent cross-gender behaviors who may or may not have yet desisted in their gender dysphoria would be experienced by homosexual men as effeminate and may, therefore, be rejected as sexual partners. Consistent rejection may predispose some of these individuals to consider transitioning to the female gender role as an alternative to living as a homosexual man. This hypothesized process may not occur in the lives of gay men who do not have a childhood history of gender dysphoria. However, in effeminate men with a homosexual sexual orientation and a history of gender dysphoria, it may increase the likelihood of a transsexual outcome. Future studies would need to systematically examine whether boys with persistent GID first attempt to live as homosexual men before transitioning to the female gender role and whether romantic rejection was experienced in the former. Consciously or unconsciously, there may be a weighing of pros and cons in the minds of adolescent boys with GID who continue to be effeminate regarding their likelihood of being accepted or passing as a gay male or as (trans) female. Thus, it is possible that effeminate gay men with a history of gender dysphoria who experience rejection from gay men may decide that they may be more likely to be accepted as a (trans) female and may, therefore, pursue transitioning rather than live as a gay male. It is understandable that such experience may result in significant socioemotional difficulties, which may further predispose these individuals to persistent GID.
With one exception, the persisters in the study were bisexual/homosexual in sexual orientation. The relationship between social class and persistence of gender dysphoria may be related to attitudes about homosexuality. Three decades ago, Hellman, Green, Gray, and Williams (1981) retrospectively explored a number of factors that were hypothesized to influence the development of transsexualism and sexual orientation, including childhood femininity, childhood religiosity (specifically in Catholics), and homophobia, among homosexual males, heterosexual males, and male-to-female transsexuals. Hellman et al.’s (1981) interest in exploring the relationship between religiosity and Catholicism stemmed from statements of some transsexuals that homosexuality is immoral and, therefore, transsexualism may resolve the conflict between same-sex sexual attraction and religious beliefs that do not support same-sex attractions. Hellman et al. did not find support for the view that transsexualism was simply motivated out of conflict between religious beliefs and sexual orientation. Rather, homophobia among transsexuals seemed to have stemmed from the need to maintain established social values (i.e., heterosexuality is the appropriate behavior). It was reassuring that all groups scored low on an index of homophobia; however, there were significant differences between the groups: the heterosexuals were the most homophobic and the homosexual men were the least homophobic. Not surprisingly, childhood femininity had the greatest influence on later transsexualism. However, when the level of femininity was not extreme, homophobia was significantly associated with a transsexual outcome. Hellman et al. speculated that childhood femininity in males and homophobia may interact to result in transsexualism in adulthood.
There is support for the idea that individuals who hold less favorable views of homosexuality may be less educated and belong to a lower social class compared to individuals who hold a more favorable view (e.g., Glenn & Weaver, 1979; Hill, 2002; Irwin & Thompson, 1977; Jensen, Gambles, & Olsen, 1988; Lemelle & Battle, 2004; Nyberg & Alston, 1976). There are a number of possible mechanisms through which social class may be related to attitudes about homosexuality. Higher education and, by extension, higher social class may foster more favorable attitudes towards homosexuality due to exposure to greater diversity (e.g., in people, ideas, philosophies) in higher education institutions (Herek & Capitanio, 1996; Herek & Glunt, 1993). Increased acceptance and approval of homosexuality may also reflect a larger set of changes in attitudes that takes place during higher education (Lottes & Kuriloff, 1994).
In the present study, the parents of persisters may have held less favorable views of homosexuality compared to the desisters. As a result, the persisters may have experienced more disapproval of homosexuality during development and were, therefore, more predisposed to a transsexual[52] outcome compared to boys with GID who grew up in an environment that was accepting of homosexuality. This is, of course, speculative as parental attitudes towards homosexuality were not measured in the study sample. None of the follow-up studies to date on boys with gender dysphoria have specifically examined attitudes towards homosexuality as a predictor of outcome. Given that negative attitudes towards homosexuality may also vary according to cultural background, it would be important to examine whether ethnicity, independent of social class, is predictive of gender identity outcome. In the present study, there was no significant difference in ethnicity between the persisters and desisters; however, this is not surprising given that the sample was predominantly of Caucasian background. As such, there may not have been sufficient variability in ethnicity to detect a difference if one does actually exist.
4.5.2 Childhood Sex-Typed Behavior as a Predictor of Gender Identity Outcome
Given Wallien and Cohen-Kettenis’ (2008) finding that the persisters in their study were more extreme in their childhood cross-gender behaviors than were the desisters, it was not surprising that, in the present study, childhood sex-typed behavior was predictive of group outcome at follow-up. Of the nine measures of sex-typed behavior used in the present study, the groups differed on four child (self) report measures (three of which were dimensional) and one dimensional parent report measure, with the persisters having more extreme scores (i.e., more childhood cross-gender behavior) than both desister groups. Similarly, in Wallien and Cohen-Kettenis’ study, the persisters had more extreme scores on two dimensional measures of cross-gender behavior and gender dysphoria,[53] both of which were used in the present study and on both the persisters were more extreme than were the desisters.
In a regression model,[54] both social class and childhood sex-typed behavior were predictors of gender identity outcome. Childhood sex-typed behavior was a predictor of gender identity above and beyond social class. The persisters were at substantially increased odds of having more extreme cross-gender behavior in childhood compared to the bisexual/ homosexual desisters. These findings suggest that the severity of childhood cross-gender behavior has an impact on the developmental trajectory of boys with GID: Boys with more extreme cross-gender identity and behavior are more likely to show persistence of their gender dysphoria into adolescence/adulthood while those with less extreme cross-gender identification are more likely to overcome their gender dysphoria by the time they reach adolescence/adulthood, if not before.
In the present study, the persisters were no more likely than the desisters to have met the complete categorical DSM criteria for GID in childhood. It is possible that the diagnostic criteria for GID, in its current form, are not sharp enough to distinguish children who are more likely to show persistence of the disorder from those who are not (Zucker & Cohen-Kettenis, 2008).
4.5.3 Behavior Problems in Childhood as a Predictor of Gender Identity Outcome
Using the CBCL as a measure of behavior problems in childhood, there was no significant difference between the outcome groups: the persisters did not differ from the desisters on internalizing and externalizing problems in childhood. There was also no significant difference between the three outcome groups on the percentage of each group that fell within the clinical range on internalizing, externalizing, and total problems. Thus, childhood behavior problems did not appear to impact the developmental trajectory of gender dysphoria. This finding cannot be compared to previous follow-up studies of boys with GID. In Green’s (1987) study, it was reported that the feminine group had few behavioral problems other than gender identity issues; however, Green did not systematically assess behavioral problems at the time of the childhood assessment. Wallien and Cohen-Kettenis (2008) did not provide data on associated behavior problems in their follow-up sample.
In recent years, a new line of research has suggested that some children with GID may have comorbid Pervasive Developmental Disorder (PDD) (e.g., de Vries et al., 2010). One explanation for a possible linkage between these two disorders is the intense focus on specific activities (e.g., Klin et al., 2007). This has led to some discussions about the relationship between PDD and GID and whether the presence of PDD would influence the trajectory of gender dysphoria. It is not clear if children with GID who also have PDD or traits of PDD will be more likely to persist in gender dysphoria compared to children with GID who do not have PDD or traits of PDD. It is plausible that the presence of a PDD may increase the likelihood of persistent gender dysphoria if the fixation on cross-gender interests in these children is more intense compared to children with GID without a PDD. On the other hand, for some children with PDD, the nature of the intense interest does change over time and, therefore, comorbid PDD may not place children with GID at a greater risk for persistent gender dysphoria. This is an empirical question that will require further exploration.[55]
In addition to social class and severity of cross-gender behavior in childhood as predictors of persistent gender dysphoria, there may well be additional factors that contributed to persistence and desistence of GID from childhood into adolescence, though it would be a matter of speculation as they were not measured in the study. It is possible that psychotherapy that aims to reduce gender dysphoria can alter the course of GID and make it less likely that the child will persist (e.g., Green, 1974; Cohen-Kettenis & Pfäfflin, 2003; Zucker, 2006c). Perhaps parents’ and clinicians’ attempts to modify children’s cross-gender behaviors result in a reduction of the behaviors, thereby enabling children to socialize as members of their birth sex and preventing the need for a sex change (Green, 2008). However, treatment studies with long-term follow-up are required to support this explanation. None of the follow-up studies to date, including this study, have systematically examined treatment received between the childhood assessment and follow-up.
Persistence of gender dysphoria may reflect a continuation of the psychosocial risk factors that contributed to its genesis in the first place. As one example, Zucker et al. (2012b) suggested that parental response to cross-gender behavior as it emerges in development is an important parameter in the clinical case formulation of gender-referred children. In this model, parental neutrality and parental encouragement of cross-gender behavior are both viewed as perpetuating factors in the child’s cross-gender identification. There is some support for this idea. In Green’s (1987) follow-up study, the degree to which mothers of the feminine boys were rated as supportive of the boy’s early cross-gender behavior (i.e., did not make an attempt to interrupt the cross-gender behaviors) rather than masculine behavior was significantly correlated with a rating of childhood “femininity” that was derived from the combination of six variables of cross-gender behavior (e.g., doll play, cross-dressing). Clinical impression in the assessment of adolescents with GID (where the rate of persistent gender dysphoria seems to be much higher than seen in children) is that their parents display more tolerance towards cross-gender behavior than do parents who seek consultation when their children are younger (Bradley & Zucker, 1997). One can reasonably hypothesize, then, that continued parental neutrality or encouragement of cross-gender behaviors in children with GID after the disorder develops may increase the chances of persistent gender dysphoria in adolescence and adulthood.
4.6 Variation in Persistence Rates across Follow-up Studies of Boys with GID
As previously noted, the rates of persistent gender dysphoria obtained in the present
study and by Green (1987) and Wallien and Cohen-Kettenis (2008) were significantly different. The persistence rate obtained in the present study was significantly lower than that obtained by Wallien and Cohen-Kettenis in their sample of boys with GID. Similarly, when one compares the persistence rate of the females in Wallien and Cohen-Kettenis’ study to that obtained by Drummond et al. (2008) in their follow-up study of girls with GID, there was significant variability across the two studies, with the former reporting a significantly higher persistence rate than the latter.[56] When the results from the present study were combined with the persistence rate obtained by Drummond et al. (2008) and then subsequently compared to the persistence rate obtained by Wallien and Cohen-Kettenis for boys and girls combined, there was also a significant difference. This raises the issue of cross-clinic, cross-national factors that may be contributing to variability in persistence rates, including sample composition, socio-cultural influences, differences between referred and non-referred families, and treatment experience, each of which is discussed below.
4.6.1 Sample Differences
Sample differences in severity of cross-gender behavior, age at childhood assessment, social class, and treatment may have contributed to the variability across studies in the rate of persistent gender dysphoria.
Zucker and Seto (2008) speculated that some of the previously observed variability in persistence rates may be attributable to sample differences as Wallien and Cohen-Kettenis (2008) reported on a clinically referred sample while Green (1987) reported on a non-clinical (advertised) sample that may have contained less extreme participants with respect to severity of cross-gender identification. Thus, a referral bias may be at play and account for the variability in persistence rates obtained by Green and Wallien and Cohen-Kettenis. A direct comparison could not be made between the boys in the present study and those in Wallien and Cohen-Kettenis’ study with respect to scores on specific measures of sex-typed behaviors.[57] However, comparisons of the Amsterdam and Toronto clinics on severity in clinical presentation of the children assessed at each clinic have provided some evidence to suggest that, on average, children referred to the Amsterdam gender clinic may be more extreme in their cross-gender identification compared to children referred to the Toronto gender clinic.
Cross-clinic (i.e., Amsterdam vs. Toronto) severity in clinical presentation could be measured in two ways. One approach involves comparing clinic-referred children from Toronto and Amsterdam on validated dimensional measures of sex-typed behavior. Cross-national, cross-clinic studies comparing boys with GID seen at our clinic in Toronto to boys seen at the Amsterdam gender clinic[58] found that boys seen in Amsterdam were, on average, more extreme in their cross-gender behaviors. The finding was consistent across self-report on the Gender Identity Interview (Wallien et al., 2009) and parent-report on the Gender Identity Questionnaire for Children (Cohen-Kettenis et al., 2006).
A second approach to measuring severity involves a comparison of the percentage of children from each clinic who meet full diagnostic criteria for GID. Cohen-Kettenis et al. (2003) conducted a cross-clinic comparison of children seen in Amsterdam and Toronto and found that a greater percentage of children seen at the Amsterdam clinic met full criteria for the DSM diagnosis compared to children seen at the gender clinic in Toronto. In fact, there was a 227% increase in the odds of meeting the complete DSM criteria for GID in the Amsterdam clinic compared to the Toronto clinic. This finding added support to the possibility that boys seen in the Amsterdam clinic were, on average, more extreme than boys seen in the Toronto clinic. It is possible, then, that (by extension) the boys in Wallien and Cohen-Kettenis’ follow-up study were more extreme in their childhood cross-gender behaviors compared to the boys in the present study. However, there was no significant difference between the present follow-up study and follow-up study by Wallien and Cohen-Kettenis (2008) in the percentage of boys in the respective samples that were given the full DSM diagnosis of GID in childhood. Thus, while the results of cross-clinic comparisons of the children seen at the Toronto and Amsterdam clinics suggest that children assessed in Amsterdam may be more extreme than children assessed in Toronto, it remains unclear whether the boys in the present study were, in fact, less extreme compared to the boys in Wallien and Cohen-Kettenis’ follow-up study.
The boys in Wallien and Cohen-Kettenis’ study were, on average, older at the time of the childhood assessment compared to the boys in the present study. This fits with comparative data on age at referral for gender identity concerns, which show that children in Toronto are generally referred at a younger age compared to children in Amsterdam (Cohen-Kettenis et al., 2003). It is possible that sample differences in age at assessment and severity of cross-gender behavior in childhood contributed to the variation in the rates of persistent gender dysphoria in the two studies. Discussed later, differences in treatment approaches across the clinics might have also contributed to variation in persistence rates.
The participants in the present study may have also differed from those in Green’s and Wallien and Cohen-Kettenis’ studies along dimensions of other factors that may influence the developmental trajectory of gender dysphoria. In the present study, for example, social class was a predictor of gender identity outcome with persisters more likely to originate in families from lower social class background compared to desisters. One can speculate that perhaps the participants in the present study differed from those in Green’s and Wallien and Cohen-Kettenis’ study in social class background, which could have contributed to the variability in persistence rates across the three studies. This is speculative, however, as data on social class of their participants were not available in the publications by Green (1987) and Wallien and Cohen-Kettenis (2008).
Mentioned earlier, psychotherapy may alter the course of GID; however, this variable was not measured in the present study or by Wallien and Cohen-Kettenis, which makes it impossible to make comparisons. A possibility is that, not only could there have been sample differences in whether participants received therapy between the childhood assessment and follow-up, but there may have been differences in the treatment approaches to childhood gender dysphoria. In the Dutch approach to treatment of children with GID, therapy is not directed at the gender dysphoria itself and instead focuses on concomitant emotional or behavioral problems in the child and dysfunctional family dynamics (de Vries & Cohen-Kettenis, 2012). At the gender clinic in Toronto, the specific goals of therapy are guided by the clinical formulation. In some cases, the focus of therapy is solely on resolving the child’s gender dysphoria and in other cases therapy may focus on gender dysphoria in addition to other emotional/behavioral problems identified by the parents. In instances where parents are unclear of how to proceed vis-à-vis their child’s cross-gender identification, resolving the child’s gender dysphoria may not be the focus of therapy (Zucker et al., 2012b). It is an important empirical question whether these variations in treatment approaches across the Toronto and Dutch clinics have contributed to the variation seen in the percentage of children from each clinic who persist in their gender dysphoria. It is possible that a therapeutic approach that focuses on resolving a child’s gender dysphoria may result in a greater likelihood of desistence compared to an approach does not directly address the gender dysphoria. To address this issue, systematic treatment studies with long-term follow-up would be required.
Green (2008) suggested that a cohort effect may also explain why the more recent study by Wallien and Cohen-Kettenis (2008) found a higher persistence rate than his follow-up study conducted over two decades ago. Green (2008) hypothesized that, over the years, society’s increasing tolerance for cross-gender behavior in children might have raised the threshold for clinical referral. As such, children assessed three decades ago may have been less extreme in their cross-gender behavior because the threshold for referral was lower at that time. Thus, children referred more recently are more extreme in their cross-gender behavior and, therefore, more likely to show persistence of gender dysphoria. In the present study, childhood assessment data were collected over a 30-year period. The severity of sex-typed behavior did not vary as a function of year of assessment. Contrary to Green’s hypothesis, the boys seen 30 years ago were, on average, no less severe in their childhood cross-gender behaviors than boys seen in past 10 years.
4.6.2 Sociocultural Influences
There is some merit to Green’s stipulation that societal tolerance for cross-gender behavior may impact the threshold for becoming concerned about children’s cross-gender behavior and a subsequent referral to a gender clinic. In a cross-clinic comparison on the Gender Identity Interview, it was observed that children from the Toronto clinic were more guarded than their Dutch counterparts in acknowledging cross-gender feelings (Wallien et al., 2009). Moreover, older children in the Toronto sample were less likely to report cross-gender feelings whereas this was not seen in the Dutch sample. Wallien et al. (2009) hypothesized that perhaps the Dutch children were less inhibited and more candid about sharing cross-gender feelings because their culture, on average, is more tolerant of cross-gender behaviors compared to Toronto culture. At the same time, Dutch children with GID experience similarly poor peer relations as children with GID seen in Toronto (Cohen-Kettenis et al., 2003; Wallien et al., 2009). A similar sociocultural hypothesis was offered to explain the older age of referral seen among Dutch children with GID compared to children seen in Toronto (Cohen-Kettenis et al., 2003). Perhaps the parents of Dutch children with GID were relatively less concerned about their children’s early cross-gender behavior compared to their Toronto counterparts and, therefore, a greater period of time elapsed between onset of cross-gender behaviors and the clinical assessment.
Cross-cultural differences in attitudes towards children’s cross-gender behavior may also play a role in the variability in persistence rates seen across the Dutch and Toronto clinic. As noted previously, some clinicians (e.g., Green, 1987; Zucker et al., 2012b) have suggested that parental tolerance of children’s cross-gender behaviors may encourage/perpetuate the behaviors, which may increase the likelihood of persistence of the behaviors into adolescence. If Dutch parents are, on average, less concerned and more tolerant of their children’s cross-gender behaviors compared to Toronto parents, this may have contributed to the higher persistence rate of gender dysphoria obtained by Wallien and Cohen-Kettenis (2008). Of course, cross-clinic data on parental attitudes towards cross-gender behavior would be needed to evaluate this hypothesis.
The issue of sociocultural influences regarding GID raises a question about the influence of society’s attitudes about cross-gender behaviors on persistence and desistence rates. The fa’afafine is a clearly defined third gender in Samoa, a society in which there is considerable acceptance and support of boys who take on the social roles of females (Vasey & Bartlett, 2007). In a retrospective study, most fa’afafine recalled that they frequently engaged in cross-gender behaviors in childhood and some adopted a cross-gender identity, believing they were girls (Vasey & Bartlett, 2007). One can, therefore, conceptualize fa’afafine as biological males who show persistence of childhood cross-gender behavior into adulthood. An empirical question is raised about whether there would be a higher persistence rate of cross-gender behaviors and identification from childhood into adolescence and adulthood in Samoa, or societies in which gender is not a binary construct, compared to societies in which gender is conceptualized as a binary construct. Using the Samoan culture as an example, there have been no published data on whether boys who are identified as fa’afafine in childhood grow up to later identify as males and, therefore, desist in their fa’afafine identity.
4.6.3 Referred vs. Non-Referred Children
It is also important to consider that parents who bring their children to a gender identity clinic may differ in attitude towards cross-gender behavior from parents who choose not to have their child seen by a professional. This raises a larger issue of how representative clinically referred children with cross-gender behavior are of all children with similar behaviors. For the most part, the prospective studies of boys with GID reported on samples of clinically referred children. The notable exception was Green’s (1987) sample, which was recuited through advertisement. It is unclear if and how these children, and their families, differ from families who choose to not seek professional consultation. Perhaps parents of non-referred children are less concerned compared to parents who seek professional services for their child’s cross-gendered behaviors. However, some parents of extremely cross-gendered children who do not seek an assessment/treatment may be ambivalent about how to address the issue or may be avoiding it all together. Given the obvious difficulty of conducting a study of parents who do not seek professional help, we simply do not know how treatment-seeking families differ from non-treatment seeking families and whether these differences can affect the development trajectory of the child’s gender identity, and ultimately affect persistence/desistence of gender dysphoria. It is also possible that the assessment process itself, regardless of whether psychotherapy is subsequently received, alters the natural history of cross-gender identification in some referred children, thus reducing the risk for persistent GID.
4.6.4 Treatment Experience
There is another reason to speculate that the families seen at the clinic in Toronto may be different from families that do not seek professional help for their cross-gender identified child and also from families who seek help at other clinics. The clinic’s philosophy around treatment of gender dysphoria in children has been publicized in mainstream local media (e.g., Toronto Life magazine, The Agenda with Steve Paiken). Parents of cross-gender identified children who believe that their child is inherently transgendered and who do not view their child’s cross-gender identification as psychopathological may seek the support of clinicians who support transition rather than attend a clinic where the treatment philosophy does not include explicit support for gender transitioning in childhood. It is possible that the children referred to our clinic and, by extension, the participants in the study may represent a biased sample. One therefore wonders whether the persistent rate obtained is representative of the persistent rate within the overall population of children with GID.
4.7 Implications of High Desistence Rate
4.7.1 Theoretical Implications
In comparing the long-term outcome of children with GID obtained in prospective studies to retrospective studies of adolescents and adults with GID, a notable disjunction with regard to gender identity outcome is observed. While adolescent and adult males with GID, particularly those who are androphilic,[59] recall a pattern of childhood cross-gender behavior that is consistent with the phenomenology of GID, most children with GID do not continue to have GID in adulthood. How might this disjunction be understood? Children with GID have different developmental trajectories and this leads to diverse outcomes in adolescence and adulthood. Perhaps there is malleability or plasticity in gender identity differentiation early on in development; however, it becomes more fixed as development progresses into adolescence and adulthood (Coates & Wolfe, 1997; Meyer-Bahlburg, 2002; Zucker, 2006a; Zucker & Bradley, 1995).
Clinical observation and empirical evidence support this idea–persistence of gender dysphoria, including the desire for sex change, is higher among patients assessed for the first time during adolescence and then followed up than among patients first assessed in childhood and then followed prospectively (Zucker & Bradley, 1995). In Cohen-Kettenis and van Goozen’s (1997) follow-up study of Dutch adolescents with GID, the rate of persistent gender dysphoria was 66.6%. This is similar to the percentage of adolescents recommended for puberty blocking hormonal treatment at the Toronto clinic (Zucker et al., 2011). If we assume liberally that the adolescents recommended for puberty blockers would persist in their gender dysphoria, the persistence rates obtained by Cohen-Kettenis and van Goozen and Zucker et al. in their adolescent samples are substantially higher than that obtained in the follow-up studies of boys with GID first referred in childhood. That gender identity is relatively more malleable in childhood but becomes less plastic as development progresses may also explain why the persisters were significantly older at the time of the childhood assessment compared to the desisters.
Another explanation for the disjunction between rates of persistence of GID in children versus adolescents may pertain to the differences in the DSM criteria for these age groups (Drummond et al., 2008). The criteria for GID in children places relatively greater emphasis on surface behavior indictors of cross-gender identification, whereas the criteria in adolescence (and adulthood) relies more heavily on behaviors and feelings stemming from the conflict between subjective gender identity and somatic sex (i.e., anatomic dysphoria). Thus, the childhood criteria for GID may also be capturing children that are at relatively low-risk for persistent GID while the diagnostic criteria for GID in adolescents and adults, with its emphasis on somatic indicators (e.g., in males, distress about facial hair, deepening of voice), may be capturing primarily the high-risk for transsexualism/persistence group.
4.7.2 Clinical Implications
That most boys did not continue to experience gender dysphoria in adolescence and adulthood and reported feeling happy and comfortable living as males raises the issue of “best practice” in clinical management of GID. At present, there are three therapeutic approaches for GID, each informed by distinct conceptual and philosophical assumptions regarding gender identity development: one actively attempts to work with the children and their parents to lessen the child’s gender dysphoria; in a second approach, there is no active attempt to lessen the child’s gender dysphoria or cross-gender behaviors; and a third, more recent, approach actively encourages gender transitioning in childhood and puberty blocking hormones as puberty approaches (if the gender dysphoria persists). The third approach has recently been featured on popular TV shows such as the Oprah Winfrey Show, 20/20, and Anderson Cooper. Two important questions regarding therapeutics for children with GID are raised: (1) Should gender transition be encouraged in childhood given that most boys with GID will not continue to experience gender dysphoria later in life, and (2) Do the various treatment approaches for children with GID have different long-term gender identity outcomes?
4.7.2.1 Should Gender Transitioning be Encouraged in Childhood?
An early gender transitioning approach appears to stem from a theoretical standpoint that the persistence or desistence of gender dysphoria occurs in isolation and is not influenced by biological, psychological, or social factors. To some extent, there also seems to be the assumption that gender identity is fixed at an early age and is not malleable. While this may be true for the vast majority of children, there are some children whose gender identity does change. The high desistence rate obtained in follow-up studies suggested that, for some children, gender identity is not fixed at an early age and is, indeed, malleable. Thus, one needs to consider if they want to encourage early transition and, hence, a pathway of complex medical treatment (cross-sex hormonal treatment, sex-reassignment surgery) without first trying to understand the nature of a child’s gender identity and whether there is any room for helping the child develop a gender identity that is aligned with their biological sex.
Apart from case reports (e.g., Ehrensaft, 2011, 2012), there is little in the way of published data on the experience of children who transition in childhood. As there have been no follow-up studies of these children; at this time, one can only speculate about potential risks of this approach. There are reports that some children who engage in a social transition in childhood later on reverse their gender role transition and return to a gender role that is aligned with their biological sex (e.g., Edwards-Leeper & Spack, 2012; Menvielle, 2012). At the present time, however, it remains unknown what percentage of these children later reverse their transition. One has to consider the potential risk of harm to children who are encouraged to transition early but who later experience resolution of their gender dysphoria and want to reverse their transition.
In the qualitative study by Steensma et al. (2011) on 25 adolescents who had been diagnosed with GID in childhood, two girls who had lived as boys, and were treated as such but had not officially transitioned, during elementary school reported that they found it very difficult to return to the female gender role once they realized that they no longer wanted to live in the opposite gender role (presumably because their gender dysphoria resolved). Fear of teasing and shame to admit they were “wrong” about wanting to transition prolonged these children’s distress, though they did eventually return to their female gender role in high school. One can imagine how difficult it would be for children who had socially transitioned in childhood and who were living for years as the opposite sex to make a change back, particularly if only their immediately family were aware of their biological sex (de Vries & Cohen-Kettenis, 2012). Some children could conceivably feel “stuck” in the opposite gender role even if their gender dysphoria desisted as they had committed themselves, parents, and others in their life in supporting their transitioning. Some children may not disclose that they no longer want to live as the opposite gender and may, therefore, maintain a transgendered presentation even if it conflicts with their felt gender identity. Thus, the decision to support an early transition raises the concern that a child may not feel free to switch back to a gender role aligned with his or her biological sex if he or she desires to do so in the future, a concern that is acknowledged by some clinicians who are supportive of early gender transitioning (e.g., Edwards-Leeper & Spack, 2012).
de Vries and Cohen-Kettenis (2012), in their description of the Dutch approach to treatment of children and adolescents with GID, provided an additional rationale for not recommending early transition. There is concern that children who transition very early (e.g., in preschool) may not realize that they are of the other natal sex and develop a sense of reality that is different from their physical reality that makes acceptance of the multiple treatments they will later need an unnecessarily difficult process.
At the same time, one also has to consider the possible advantages of an early transitioning approach. At the present time, we do not know whether the various treatment approaches will differentially affect the long-term psychiatric functioning and overall adjustment of these children. If, for example, persisters showed a better psychosocial adjustment and adaptation than children who desist (e.g., become homosexual or heterosexual without gender dysphoria), then one can question whether treatment efforts to maximize the chances of desistence (and prevent persistence) should be the optimal treatment goal (Zucker et al., 2012b). The argument can also be made that, for children who will turn out to be persisters, an early gender transitioning may be beneficial as there may be drawbacks to having to wait until puberty or adolescence to begin gender transitioning (Steensma & Cohen-Kettenis, 2011). However, the problem remains in the difficulty in distinguishing the persisters from the desisters at a young age. If it were possible to know with certainty whether a child with GID will persist or desist, then the clinical approach can be modified to best match the child’s needs. In the absence of perfect science, combined with the high chances that gender dysphoria will desist and possible risk to those who transition in childhood but then want to reverse the transition, clinicians should be cautious in recommending gender transitioning in childhood. It is conceivable that the drawbacks of having to wait until early adolescence to begin transition may be less serious than having to make a social transition twice (Steensma & Cohen-Kettenis, 2011).
4.7.2.2 Effects of Treatment on Long-Term Gender Identity Outcome
A second important question is whether these various treatment approaches will result in different long-term gender identity outcomes for these children (Drescher & Byne, 2012). For example, will the rate of persistence be higher for children who are allowed to gender transition at a young age compared to children for whom there is some attempt to lessen their gender dysphoria and cross-gender behaviors? In the clinical management of adolescents with gender dysphoria, one of the rationales for recommending puberty blocking hormonal treatment is that suspension of the patient’s biological puberty will reduce their preoccupation with it and, therefore, afford the adolescent greater opportunity to explore his or her long-term gender identity options in psychotherapy in a less pressured manner (Edwards-Leeper & Spack, 2012; Zucker et al., 2011). In a review of current treatment approaches, Stein (2012) suggested the possibility that temporarily stopping puberty may have the effect of increasing persistence. Thus, instead of allowing adolescents more time to “wait-and-see” and evaluate their gender identity options, puberty blocking treatment may unintentionally push adolescents towards cross-sex hormonal treatment and sex-reassignment surgery.
Along the same lines, one can hypothesize that allowing children to socially transition in childhood may have the effect of increasing the chances of persistence into adolescence and adulthood. Without empirical comparative data on treatment approaches, one can only speculate on the effects of treatment on gender identity outcomes, if there are effects. At the follow-up assessment, participants in the present study were asked if they previously received treatment; however, a qualitative assessment of the interview data would be required to draw any substantial conclusions, which was beyond the scope of the present study. At the same time, it can be commented that some of the persisters in the study received treatment efforts aimed at helping them to resolve their gender dysphoria while in other cases much in the way of intervention was not attempted. The same can be said for the desisters.
4.7.3 Process of GID Desistence and Persistence Overtime
The present study advances our understanding of the long-term trajectories of boys with GID and the characteristics of the subgroup of the boys who persisted in their gender dysphoria into adolescence and adulthood. Gender identity appears to be relatively malleable in childhood, but becomes less plastic as development progresses. However, the factors that underlie this malleability are far from understood. We still do not know why most boys with GID “lose it” by adolescence or adulthood. We also do not understand the process of how desistence occurs and the possible interaction that occurs between biological and psychosocial variables to give rise to the observed trajectories in these children.
There have been no quantitative follow-up studies that have systematically examined the developmental process through which GID desists (e.g., how and at what age). Some authors suggest that desistence typically occurs sometime around puberty or early adolescence (de Vries & Cohen-Kettenis, 2008; Wallien & Cohen-Kettenis, 2008). However, one should be skeptical in viewing puberty as the transformative period in the lives of children with GID with regard to their gender identity. Some gender-referred children show changes in their gender identity before puberty and, in fact, desist in their dysphoria during childhood (for case examples, see Zucker, 2006c; Zucker & Bradley, 1995). In Steensma et al.’s (2011) qualitative study, persisters and desisters reported that the period from age 10 to 13 years of age was significant in the trajectory of their gender identity development. Whether gender dysphoria intensified or lessened appeared to have been influenced by psychosocial influences (e.g., peer relations), psychological factors (e.g., anticipation about puberty), and emerging sexual attraction. It is unclear how these factors interacted with other factors that have been hypothesized to influence the trajectory of GID, including therapy, family dynamics, and biological factors (e.g., temperament, a genetic predisposition to cross-gender behaviors).
It was beyond the scope of this study to systematically evaluate when and how the desisters stopped experiencing feelings of gender dysphoria. This type of question would be best evaluated using a prospective study that included multiple follow-up assessments around critical time points in children’s development (e.g., school entry, onset of somatic puberty). Notwithstanding, participants who reported desistence of gender dysphoria were asked about their thoughts on when and how it occurred. These data were not evaluated or coded in any systemic way and, therefore, can only be commented on qualitatively. Some participants stated that the gender dysphoria simply went away but could not offer any hypotheses on how nor could they remember when. Some desisters recalled feeling comfortable about their biological status as males long before puberty. Further, some desisters who were assessed early in childhood had no memory of earlier gender dysphoria and, in fact, were surprised to hear that they had, at one point, expressed a desire to be female. Clearly, desistence occurred during childhood for these males.
4.8 Variability in the Group of Persisters
On the Gender Identity Questionnaire for Adolescents and Adults, a dimensional measure of gender dysphoria, all but two persisters met criteria for caseness (of gender dysphoria), one of whom was the lone heterosexual persister, and the other was the youngest persister in the study. At the same time, based on interview data, there was notable variability in degree of gender transitioning within this subgroup. At the least extreme end of the spectrum were the participants who reported feelings of gender dysphoria but, at the same time, were not presenting socially as women, using a female name, or receiving any type of hormonal treatment (i.e., hormones to suppress masculinization, cross-sex hormones)–there were at least four such participants. At the most extreme end of the spectrum were the participants who were presenting socially as women (e.g., wearing female clothing and make-up), had legally changed their name, and were taking cross-sex hormones to feminize their bodies. Although none of the persisters had undergone any type of surgery at the time of follow-up, some expressed interest in pursuing this type of medical treatment.
Additional details regarding these gender change parameters would be needed from Wallien and Cohen-Kettenis (2008) regarding the persisting males in their sample to make comparisons.[60] However, it appears that there was relatively less variability in their groups as all of the persisters had applied for sex reassignment by the age of 16 years. Therefore, as a group, the male persisters in Wallien and Cohen-Kettenis’ study seemed more extreme in their gender dysphoria (at follow-up) compared to persisters in this study. There was no significant difference in the mean age at follow-up between the two groups; however, there was less variability in the age at follow-up in Wallien and Cohen-Kettenis’ sample (16-18 years) compared to the present sample (13-39 years). Additional follow-up assessments with the younger persisters in the present study, particularly with those who were experiencing gender dysphoria but had not initiated any form of gender transition, would clarify how many of these males continue to persist in their gender dysphoria and how many, if any, desist. Therefore, to better understand the long-term outcome of boys with GID, longer follow-up periods that extend into adulthood are necessary.
The variability in cross-gender identification among the persisters is not completely surprising. Individuals who present to gender identity clinics in adolescence are a heterogeneous group (e.g., Cohen-Kettenis & Pfäfflin, 2003, 2010; Meyer et al., 2001; Zucker et al., 2011). While most gender dysphoric adolescents who present to specialized gender identity clinics are seeking some form of biologic treatment (e.g., cross-sex hormones, sex-reassignment surgery), some gender dysphoric individuals do not request medical intervention and do not necessarily want to live in the opposite gender role (Cohen-Kettenis & Pfäfflin, 2003; Zucker et al., 2011). It is possible that the latter population may be representing individuals who are subthreshold for the DSM diagnosis of GID and, therefore, experience less gender dysphoria compared to individuals who desire sex reassignment surgery. Indeed, Cohen-Kettenis and Pfäfflin (2003) described the subthreshold adolescents seen in their clinic as a “heterogeneous group.” Some enter the clinic with a strong desire for sex-reassignment but later change their minds while others enter the clinic without a wish for sex reassignment but are confused about their gender identity and desire professional consultation. Some of these adolescents are ego-dystonic homosexual and, in others, the gender dysphoria is secondary to other psychopathology, such as a Pervasive Developmental Disorder. Interest in measuring gender dysphoria as a dimensional construct has been driven, in part, by the observed heterogeneity in adolescents and adults with GID (e.g., Deogracias et al., 2007; Singh et al., 2010).
4.9 Predictors of Sexual Orientation Outcome
As discussed above, the results of the present study were consistent with previous follow-up studies of effeminate boys and boys with GID that have shown that childhood cross-gender behavior and identification is associated with a high rate of bisexual/ homosexual outcome. These data also converge nicely with retrospective studies of homosexual men (Bailey & Zucker, 1995) and cross-cultural studies of men attracted to men (e.g., Bartlett & Vasey, 2006). At the same time, 33.3% of the participants reported a heterosexual outcome at follow-up. In follow-up studies by Green (1987) and Wallien and Cohen-Kettenis (2008), 25% and 19% of the participants, respectively, reported a heterosexual sexual orientation at follow-up. The relationship between age and “coming out” may, in part, account for this finding, as discussed earlier. However, that some males with GID develop a heterosexual outcome is not fully understood.
Wallien and Cohen-Kettenis (2008) hypothesized that perhaps degree of cross-gender identification in childhood may affect sexual orientation outcome, but they did not find support for this in their sample–differences in severity of childhood cross-gender behavior between the heterosexual and homosexual participants was obtained only for the persisters and not the desisters. In Green’s (1987) study, the results were mixed. On one hand, there was a significant correlation between childhood peer interest and doll play and adult sexual orientation in fantasy. However, within the group of feminine boys, there was no significant correlation between an overall femininity score and later sexual orientation.
In the present study, there were significant group differences between the bisexual/ homosexual persisters, bisexual/homosexual desisters, and heterosexual desisters on five of nine measures of childhood sex-typed behaviors. In each instance, the persisters were more extreme in cross-gender identity/behaviors than were the two desister groups. In addition, there was some support for the idea that perhaps severity of cross-gender behavior may not only predict gender identity outcome, as discussed earlier, but also sexual orientation outcome. On one of the nine measures of childhood sex-typed behavior (Free Play), the bisexual/homosexual desisters were less extreme than the bisexual/homosexual persisters but more extreme than the heterosexual desisters. Though speculative, it is possible that the bisexual/homosexual desisters and heterosexual desisters did not show more group differences because some of the males who identified as heterosexual may later identify as bisexual/homosexual. Of course, subsequent follow-up of the heterosexual group would be needed to evaluate this hypothesis. In a regression model,[61] a composite measure of childhood cross-gender behavior was the only predictor of outcome when the heterosexual desisters were compared to the bisexual/homosexual desisters. The bisexual/homosexual participants were at increased odds of having more extreme childhood cross-gender behaviors compared to the heterosexual desisters.
These results suggest that there is also an association between severity of childhood cross-gender behavior and sexual orientation outcome. Within the desistence group, the boys who were more cross-gender identified developed a bisexual/homosexual sexual orientation and the boys who were less extreme in their cross-gender identification developed a heterosexual sexual orientation. As discussed earlier, there was also a “dosage effect” in the relationship between childhood cross-gender behavior and gender identity outcome. However, the dosage effect appears to be stronger in separating the persisting from the desisting cases (the bisexual/homosexual persisters had a 274% increase in odds of having more extreme childhood cross-gender behavior compared to the bisexual/homosexual desisters) than in separating the bisexual/homosexual desisters from the heterosexual desisters (the bisexual/homosexual desisters had a 48% increase in odds of having more extreme childhood cross-gender behavior compared to the heterosexual desisters).
The relationship between variation in degree of childhood cross-gender behavior and later sexual orientation has been demonstrated in epidemiological samples drawn from non-clinical populations. In a 24-year follow-up of 406 boys taken from a population based study and who were, therefore, unselected for their gender identity, those who were considered gender variant on a parent-report measure of behavior problems were more likely to develop a minority sexual orientation outcome compared to those who were classified as non-gender-variant (Steensma et al., 2012). Depending on whether sexual orientation was classified according to fantasy or behavior, the prevalence of bisexuality/homosexuality within the gender variant group was 8.7-9.5 times higher than that in the non-gender-variant group.
4.10 Behavioral Problems and Psychiatric Functioning at Follow-up
4.10.1 Behavior Problems at Follow-up
There were significant correlations between maternal ratings of behavior problems in childhood and at follow-up on three indices of disturbance: internalizing, externalizing, and total problems. Thus, the participants who were rated by their mothers as more extreme in behavior problems in childhood were also rated as more extreme in behavior problems at follow-up. However, maternal ratings in childhood did not correlate significantly with self-report at follow-up. At follow-up, however, there were significant correlations between participants’ self-report and maternal report on internalizing, externalizing, and total problems. Thus, participants and their parents were generally in agreement on the extent of participants’ behavioral problems at follow-up.
Behavior problems as a function of gender identity and sexual orientation identity at follow-up were examined in two ways. The three (primary) outcome groups (bisexual/ homosexual persisters, bisexual/homosexual desisters, and heterosexual desisters) were compared on three indices of disturbance (internalizing T score, externalizing T score, and total T score) using self-report on the Youth Self Report (YSR) or Adult Self Report (ASR) and maternal report on the Child Behavior Checklist (CBCL) and Adult Behavior Checklist (ABCL). The outcome groups were also compared on the percentage in each group whose T score fell within the clinical range on these three indices of disturbance. Based on maternal report, there were no significant differences between the three groups on internalizing, externalizing, and total problem or on the percentage of each group who fell within the clinical range. Significant group differences emerged, however, when participants’ self-report of behavior problems were examined. Specifically, the three groups differed significantly on internalizing problems, but were comparable in externalizing and total behavior problems. The heterosexual desisters reported significantly lower internalizing problems compared to the bisexual/homosexual persisters and the bisexual/homosexual desisters. The two bisexual/homosexual groups were comparable on internalizing problems.
That the heterosexual desisters had, on average, less behavioral disturbance than the bisexual/homosexual persisters was also reflected in the percentage of participants in each group whose scores on internalizing, externalizing, and total problems fell within the clinical range. Across all three indices of disturbance, a greater proportion of the bisexual/ homosexual persisters fell within the clinical range compared to the heterosexual desisters. Differences between the heterosexual desisters and bisexual/homosexual desisters were significant only on externalizing problems, with a greater proportion of the latter group falling within the clinical range. Across all three indices, there was no significant difference between the bisexual/homosexual persisters and bisexual/homosexual desisters on the percentage who fell within the clinical range.
Thus, the most consistent group differences on behavioral problems emerged between the bisexual/homosexual persisters and the heterosexual desisters, with the latter group reporting significantly less behavioral disturbance than the former. Less consistent was the group differences between the heterosexual desisters and bisexual/homosexual desisters. When differences did emerge, the heterosexual desisters reported less behavioral disturbance compared to the bisexual/homosexual desisters. At least on self-report of behavioral problems, the bisexual/homosexual persisters and bisexual/homosexual desisters were comparable.
The bisexual/homosexual persisters showed, on average, higher behavioral disturbance than nonreferred boys in the standardization sample when compared on the percentage in each group who fell within the clinical range on total problems on the YSR/ASR, but were comparable to referred boys. The bisexual/homosexual persisters had, on average, 5.18 times as many behavior problems compared with nonreferred boys. The percentage of heterosexual desisters who fell within the clinical range was lower than the referred boys in the standardization sample but comparable to nonreferred boys. The bisexual/homosexual desisters were comparable to the referred and nonreferred boys in the standardization sample.
4.10.2 Psychiatric Functioning at Follow-up
At follow-up, 37% of the entire group of participants did not have any comorbid psychiatric disorders, 23.1% had at least one, 17.7% had two, and 23.2% had three or more. Thus, 63% of participants had at least one comorbid psychiatric diagnosis at follow-up. The three outcome groups differed on the extent of psychiatric comorbidity at follow-up. Similar to the results obtained on behavioral problems at follow-up, the heterosexual desisters had significantly fewer psychiatric diagnoses at follow-up compared to the bisexual/homosexual desisters and the bisexual/homosexual persisters. The bisexual/homosexual persisters and the bisexual/homosexual desisters were comparable on psychiatric comorbidity.
4.10.2.1 Implications of Psychiatric Outcomes
When group differences did emerge in behavioral problems and psychiatric functioning, the heterosexual desisters appeared less disturbed compared to the other groups. The bisexual/homosexual persisters and bisexual/homosexual desisters were generally comparable on behavioral problems and psychiatric functioning. Thus, there is evidence that behavioral and psychiatric problems at follow-up varied as a function of both gender identity and sexual orientation. As discussed below, a number of possible factors could account for these findings.
4.10.2.1.1 Distress of Gender Dysphoria
Applicants for sex reassignment often experience their gender dysphoria as unbearable (Cohen-Kettenis & Pfäfflin, 2010). It could be argued that gender dysphoria itself among the persisters was sufficiently distressing to these individuals and it caused secondary behavioral and psychiatric difficulties (Nuttbrock et al., 2010). Thus, the distress felt by adolescents with GID due to the incongruence between their gender identity and the physical characteristics of their biological sex (i.e., anatomic dysphoria) may itself have served as a vulnerability factor in the development of comorbid psychiatric issues (Zucker et al., 2012a). In some studies, however, transsexuals were not found to have had high rates of comorbid psychiatric diagnoses (e.g., Cole, O’Boyle, Emory, & Meyer, 1997; Gomez-Gil, Trilla, Salamero, Godas, & Valdes, 2009). In the clinical setting, some applicants for sex-reassignment surgery are employed, have relationships, and function socially without problems. These individuals express that they suffer from incongruence between their anatomy and gender identity, but it does not interfere with their ability to function satisfactorily (Cohen-Kettenis & Pfäfflin, 2010). Cohen-Kettenis & Pfäfflin have interpreted this to mean that gender dysphoria, per se, may not necessarily be associated with psychiatric difficulties in some transgendered individuals. In the present study the bisexual/homosexual persisters and the bisexual/homosexual desisters were generally comparable on behavioral and psychiatric functioning, but when there were differences the bisexual/homosexual persisters had more difficulties than did the bisexual/homosexual desisters. Based on the hypothesis that gender dysphoria is sufficiently distressing to cause secondary behavioral and psychiatric difficulties (e.g., Nuttbrock et al., 2010), one would have expected more substantial differences between the bisexual/homosexual persisters and bisexual/homosexual desisters.
4.10.2.1.2 Peer and Family Rejection
Social rejection is another possible factor that could have contributed to the group differences on behavioral and psychiatric difficulties. Poor peer relations appear to be a general risk factor for behavior problems in children and youth (Schneider, 2000). Gender referred boys with GID experience substantial difficulties with peers (e.g., Zucker et al., 1997) and this has been found to be a significant predictor of CBCL behavior problems (Cohen-Kettenis et al., 2003). Although the quality of peer relation at follow-up was not measured in the present study, the results of other studies of GID adolescents suggest that these youth have significant problems with their peers (Zucker et al., 2012a). Retrospective studies of gay men had demonstrated that childhood gender nonconformity was significantly associated with peer rejection (Landolt, Bartholomew, Saffrey, Oram, & Perlman, 2004).
Although we did not have data on parental attitudes towards their child’s gender dysphoria, it is possible that rejection from family members may have contributed to the elevated levels of behavioral and psychiatric disturbance among the bisexual/homosexual persisters compared to the heterosexual desisters. Transgendered adults, on average, may receive less social support from family members compared to their non-transgendered siblings (Factor & Rothblum, 2007) and among gay, lesbian, and bisexual youth, those who reported higher levels of familial rejection were at increased risk for psychological disturbance (suicide attempts, depression, substance use) compared to youth who reported no or low levels of family rejection (Ryan, Huebner, Diaz, & Sanchez, 2009). In future studies, it would be important to also measures levels of current support, at the peer and family level, in these individuals.
4.10.2.1.3 Minority Stress
Minority stress (i.e., social prejudice, victimization, and discrimination experienced by non-heterosexual individuals) appears to account, in part, for the strong association between homosexuality and mental health risk (Meyer, 1995; 2003). For example, within GLB populations, levels of mental health risk (e.g., suicidality, substance use) appear to be mediated by victimization (Almeida, Johnson, Corliss, Molnar, & Azrael, 2009; Bontempo & D’Augelli, 2002). In a study of 245 gay, lesbian, bisexual, and transgender youth (GLBT), victimization due to perceived or actual GLBT status fully mediated the association between gender nonconformity and psychosocial adjustment (Toomey, Ryan, Diaz, Card, & Russell, 2010). Thus, minority stress may be another factor that contributed to the higher rates of behavioral and psychiatric difficulties seen among the bisexual/homosexual persisters and bisexual/homosexual desisters. At the same time, studies of homosexual adults in countries known for their liberal and accepting attitudes towards homosexuality, such as the Netherlands, also show a relationship between sexual orientation and mental health, with homosexual individual reporting more mental health difficulties compared to their heterosexual counterparts (e.g., Sandfort et al., 2006). In the present study, 62.5% of participants for whom data were available reported lifetime experience of victimization. As a group, participants’ total victimization scores across their lifetime and in the 12 months preceding the follow-up assessment were significantly and positive correlated with a parent-report measure of concurrent cross-gender behavior. Thus, participants who were rated as more cross-gendered in behavior by their parents, had also self-reported higher levels of victimization compared to participants rated by their parents as having less cross-gendered behaviors. On an overall measure of victimization, the bisexual/homosexual persisters reported significantly more victimization in their lifetime and in the 12 months preceding the follow-up assessment compared to the bisexual/homosexual desisters and heterosexual desisters. Further, participants’ overall victimization scores for the 12 months preceding the follow-up assessment were significantly and positively associated with their self-report of externalizing, and total problems on the Youth Self-Report/Adult Self-Report. Thus, participants who experienced higher levels of victimizations were more likely to report higher levels of emotional and behavioral problems.
These results are not surprising. Even among youth unselected for their gender identity, the presence of gender atypical behavior appears to be associated with poorer well being (Rieger & Savin-Williams, 2012) and places these youth at higher risk for victimization compared to gender atypical youth. Thus, transgender youth are particularly vulnerable to victimization because of their atypical gender role presentation (for a discussion, see Stieglitz, 2010). Generally, the rates of victimization among transgender youth appear to be higher than the estimated rates for youth victimization in North American (e.g., Grossman, D’Augelli, & Salter, 2006; Nuttbrock et al., 2011).
Some sexual minority youth also struggle with felt stigma, defined as one’s subjective experience of stigma against his/her group and this may influence decisions regarding disclosure of sexual orientation (Burn, Kadlec, & Rexer, 2005), and possibly gender identity. Self-stigmatization, also referred to as internalized homophobia, may influence individuals to conceal their sexual orientation and this may intensify their experienced minority stress and contribute to mental health difficulties (Oswalt & Wyatt, 2011). Self-stigmatization may have been operating among participants in the present study; however, this is speculative as this construct was not measured.
Sexual minority and transgender youth, on average, have been found to experience higher levels of psychological difficulties compared to their heterosexual and non-transgender counterparts, which is also supported by the results of the present study. One hypothesis for shared risk among these two groups is that the presence of gender atypical behavior in GID adolescents and homosexual men, rather than cross-gender identity or sexual orientation per se, places sexual and gender minority youth at risk. Rieger and Savin-Williams (2012) found some support for this hypothesis. In a study of 475 high school seniors, childhood and adolescent gender nonconformity was negatively associated with a measure of psychological well-being. This relationship was not moderated by sexual orientation. Thus, Rieger and Savin-Williams concluded that the factors that caused gender nonconforming homosexual or bisexual individuals to suffer psychologically may also apply to heterosexual individuals who are gender nonconforming. Savin-Williams and Ream (2003) suggested that sexual orientation per se has little explanatory power for understanding the relatively consistent finding that homosexual individuals are at greater risk for mental health difficulties compared to their heterosexual counterparts; rather, the association exists within the social context in which gender atypical behavior and sexual orientation evoke negative reactions (e.g., victimization) that leads to psychological distress.
One can infer that the bisexual/homosexual persisters in the present study had more cross-gendered behavioral compared to the desisters by virtue of their persistent gender dysphoria. Parent-report of gender role behaviors at follow-up also supported this inference. The bisexual/homosexual persisters were rated as significantly more cross-gendered compared to both desister groups. The bisexual/homosexual desisters were, in turn, rated as more cross-gendered than the heterosexual desisters. Given the above discussions about the relationship between gender atypical behavior and mental health, this finding may, in part, account for the consistent finding that the heterosexual desisters in the present study were found to have had better behavioral and mental health outcomes at follow-up compared to the bisexual/homosexual persisters. One would have predicted that the bisexual/homosexual desisters would have had more behavioral and psychiatric difficulties than the heterosexual desisters but less than the bisexual/homosexual persisters but this was not consistently found.
4.10.2.1.4 Familial Psychiatric Vulnerability
The above summarized data are not to imply that victimization is the only factor that explains the increased risk for mental health problems in sexual minority individuals. There are likely other factors (Bailey, 1999). Mays and Cochran (2001) found that controlling for reported levels of discrimination among gay, lesbian, and bisexual adults reduced the relationship between sexual orientation and mental health but did not eliminate it. Similarly, in a recent population based survey of Swedish adults, rates of depression, anxiety, and alcohol use were increased among individuals with same-sex sexual partners (Frisell, Lichtenstein, Rahman, & Langstrom, 2010). When discrimination and hate crime victimization were controlled for, this risk was reduced. However, controlling for familial factors in within-pair comparisons reduced and, at times, eliminated it. This suggests that the psychiatric vulnerability observed in sexual minority youth may also be understood from the perspective of more general familial risk.
Further support for the hypothesis that sexual minority youth may be psychiatrically vulnerable comes from a recent study of 4942 adult twin pairs which found that genetic factors accounted for 60% of the correlation between sexual orientation and depression (Zietsch et al., 2012). It is possible that the bisexual/homosexual persisters originated within families with higher levels of psychiatric difficulties and, therefore, had higher risk for developing such problems, compared to the heterosexual desisters. This is, of course, speculative as family psychiatric history was not systematically assessed.
One controversial mental health issue pertaining to sexual minority youth concerns suicidality ideation and suicide attempts (Zucker, 2010b). Gay, lesbian, and bisexual youth, in addition to being at greater risk for mental health disorders (e.g., Cochran, 2001; Meyer, 2003), are also at greater risk for suicidal behaviors (Halpert, 2002; Kulkin, Chauvin, & Percle, 2000) compared to heterosexual counterparts. In a recent meta-analysis, King et al. (2008) concluded that sexual minorities were 2.47 times more likely to have attempted suicide in their lifetime. Further, high rates of suicide attempts among sexual minority individuals does not appear to simply be an artifact of high rates of mental disorder in this group, but, rather, occurs independent of psychiatric diagnosis at higher rates than heterosexual individuals (Bolton & Sareen, 2011). Although epidemiological studies have not been conducted, available data on transgendered youth using community samples suggest a greater risk for suicidal ideation and self harm (e.g., Almeida et al., 2009; Mathy, 2003) compared to non-transgendered youth. That there is elevated risk for suicidality among homosexual and transgendered youth was supported by results of the present study.
On the Suicidality Questionnaire, the three outcome groups differed significantly on number of lifetime suicide attempts. The bisexual/homosexual desisters reported, on average, a greater number of lifetime suicide attempts compared to the heterosexual desisters but were comparable to the bisexual/homosexual persisters.
Suicidal ideation in the 6 months preceding the follow-up assessment was measured using the Youth Self Report (YSR)/Adult Self Report (ASR). The bisexual/homosexual persisters were significantly more likely to endorse this item compared to the heterosexual desisters, but were comparable to the bisexual/homosexual desisters. The frequency of reported suicidal ideation among the bisexual/homosexual persisters was also significantly higher than that reported by referred and nonreferred boys in the YSR standardization sample and the nonreferred boys in the ASR standardization sample. The bisexual/homosexual desisters were more likely to endorse suicidal ideation compared to the nonreferred boys in the YSR and ASR standardization samples but were comparable to referred boys. The results for the heterosexual desisters varied according to the standardization sample used for comparison–group differences only emerged when compared to the ASR standardization sample. The heterosexual desisters were more likely to endorse suicidal ideation compared to the nonreferred boys but were less likely to when compared to the referred boys. Thus, the bisexual/homosexual persisters were the only group who reported greater suicidal ideation when compared to a group of clinically referred boys.
The three outcome groups also differed on suicidal and self-harm behavior[62] in the 6 months preceding the follow-up assessment. The bisexual/homosexual persisters were significantly more likely to endorse suicidal and self-harm behaviors compared to the bisexual/homosexual desisters, heterosexual desisters, referred boys in the standardization sample, and non-referred boys in the YSR and ASR standardization samples. The heterosexual desisters reported significantly more suicidal behavior compared to the nonreferred boys in the YSR standardization sample only, but were comparable to the bisexual/homosexual desisters and to referred boys in both standardization sample. The bisexual/homosexual desisters reported less suicidal behavior compared to the referred boys in the ASR standardization sample only, but were comparable to the nonreferred boys from both standardization samples. Thus, the most consistent finding from the YSR/ASR suicidality data was that the bisexual/homosexual persisters were significantly more likely to have experienced suicidal ideation and suicidal and self-harm behaviors compared to the other groups, including the standardization samples. However, in terms of lifetime risk of suicide attempts, the bisexual/homosexual desisters reported the highest number.
Studies of community samples of transgendered youth have suggested that they may be at even greater risk for suicide ideation and attempts than homosexual males (Mathy, 2003) and that cross-gender role behavior may be responsible for these findings (Maugen & Shipherd, 2010). Thus, while some homosexual men may engage in gender atypical behaviors that place them at risk, the pervasive and more extreme cross-gender behaviors of transgendered individuals may place them at even higher risk compared to homosexual individuals. In one study, cross-gender role accounted for more of the variance in suicidal ideation than sexual orientation (Fitzpatrick, Euton, Jones, & Schmidt, 2005) and in another study of gay, lesbian, and bisexual adults, the relationship between sexual orientation and suicidality decreased substantially after gender atypical behaviors were controlled for (Plöderl & Fartacek, 2009). The greater risk for suicidal ideation and attempts among transgendered youth compared to homosexual (and heterosexual) youth may be directly related to discrimination and victimization pertaining to their atypical gender role behaviors (Clements-Nolle et al., 2006; Nuttbrock, 2010). In a recent prospective study of 246 gay, lesbian, bisexual, and transgendered youth, victimization was associated with both suicidal ideation and self-harm, as was a history of completed suicide (Liu & Mustanski, 2012). In a study of 55 transgendered youth recruited from programs that provide services to this population, Grossman and D’Augelli (2007) attempted to clarify what differences might exist between those who attempted suicide and those who did not along the parameters of gender nonconformity, childhood parental abuse, body self esteem, and negative thoughts about transgendered identity. The suicide attempters reported greater parental abuse, more negative body self-esteem, and more negative thoughts about being transgendered compared to the non-attempters. Thus, it is possible that, in addition to minority stress and victimization, there are additional factors that contribute to the elevated risk for suicidality among transgendered youth, including factors discussed above that are deemed relevant to understanding elevated risk for mental health issues within this population, including gender dysphoria itself, and general familial risk.
It has been an assumption that gender dysphoria itself is one reason for the increased prevalence of suicidality among transgendered youth. However, follow-up data on psychiatric outcome of transgendered individuals who receive cross-sex hormonal therapy and sex-reassignment surgery suggest that, even among individuals who receive medical treatment for gender dysphoria, there may be an increased risk for suicidality compared to the general population (Asscheman et al., 2011; Dhejne et al., 2011; van Kesteren, Asscheman, Megens, & Gooren, 1997). These findings are surprising as one would expect that sex-reassignment surgery, which will serve to align the body of transgendered individuals with their gender identity, would substantially reduce the gender dysphoria, if not eliminate it, and, therefore, reduce the risk for suicide. Continued risk for suicidality suggests that there may be an underlying vulnerability for suicidality (and, perhaps, depression more generally) that contributes to its persistence even after medical treatment for gender dysphoria is received.
In a recent three-part video series called “The Sissy Boy Experiment,” CNN’s Anderson Cooper reported on Kirk Murphy, who committed suicide in 2003 when he was 38-years-old. Kirk was one of the “feminine” boys in Green’s (1987) follow-up study. Following Kirk’s childhood assessment, he was seen in therapy by George Rekers at the University of California, Los Angeles (UCLA). A published report of Kirk’s treatment[63] (Rekers & Lovaas, 1974) indicated that a behavioral approach had “normalized” Kirk’s sex-typed behaviors and “he looked and acted like any other boy.” At follow-up, when he was 18-years-old, Kirk identified as a male and was happy with his gender identity. He reported a bisexual sexual orientation.
In “The Sissy Boy Experiment,” the viewer finds out that Kirk later disclosed a homosexual sexual orientation. This case report and above summarized data on psychiatric functioning have three important implications. First, even after receiving treatment for gender dysphoria, transgendered individuals appear to be at risk for suicidality/psychiatric difficulties. Second, prospective studies should follow these individuals beyond adolescence and well into adulthood. On this point, a recent study of 571 male-to-female transgender individuals[64] recruited from the population found a prevalence rate of depression to be 54.3%. When examined according to age group, the highest levels of depression were found among those aged 19-39 years, and then decreased thereafter (Nuttbrock et al., 2010). Third, children with GID who later desist in their gender dysphoria may still be psychiatrically vulnerable. In the present study, the bisexual/homosexual desisters reported the highest rate of lifetime suicide attempts and the heterosexual desisters reported significantly more suicidal and self-harm behaviors compared to nonreferred boys in the standardization samples. A general implication of these findings is that, in practice, clinicians working with youth should ask about sexual orientation, given the strong relationship between minority orientation and psychiatric problems and suicidality.
4.12 Limitations of the Present Study and Future Directions
The most prominent limitation of the study is that concurrent control groups, either clinical (i.e., referred for reasons other than gender identity concerns) or community, were not employed. Accordingly, some of the comparative analyses relied on epidemiological or survey data. However, the exclusion of a control group is methodologically justified given the goal of the study was to examine outcomes within a specific group of children.
There are a number of prospective approaches that can be used study the relationship between cross-gender behavior in childhood and later gender identity and sexual orientation, and with each approach there are implications on the populations to which results can be generalized. This present study examined children referred to a specialized gender identity clinic because of concern around their cross-gender behavior and gender identity status. Therefore, generalizations about psychosexual development and psychiatric functioning in adolescence and adulthood are limited to clinic-referred boys with severe cross-gender behaviors. Generalizations to other populations should be done with caution.
There were a number of other factors which may affect the long-term psychosexual outcome of boys with GID which were not evaluated in the present study. A major such factor pertains to the role of psychotherapy on long-term psychosexual and psychiatric outcomes. Future studies which systematically evaluate treatment involvement and utilizing relevant comparison groups will provide much needed information regarding the differential effects of various treatment options, including no treatment, on long-term outcomes. These data are urgently needed given the lack of treatment consensus within the field.
Although this study has contributed substantially towards understanding childhood predictors of outcome within a group of boys with GID, as a field, we do not understand how and when desistence of gender dysphoria occurs. Systematic prospective studies, utilizing multiple follow-up assessments that extend well into early adulthood are needed.
Data on continued risk for suicidality in transgendered youth and among boys with GID who desist in their gender dysphoria as well as the empirical literature on the coming out process suggest that follow-up periods should ideally extend beyond adolescence and into adulthood.
Since Green and Money’s (1960) seminal article on boys with “incongruous gender role,” much progress has been made in understanding the phenomenology of GID. The long-term psychosexual outcome of boys with GID has also received some empiric attention, with studies having consistently found that most boys desisted in their gender dysphoria and had a homosexual sexual orientation. The present study extended previous follow-up studies of boys with GID and, in addition to examining rates of persistent gender dysphoria and sexual orientation outcome, attempted to identify within-group childhood factors that were predictive of long-term psychosexual outcomes. In the present follow-up study, the most common outcome at follow-up, consistent with the extant literature, was a desistence of GID with a co-occurring bisexual/homosexual sexual orientation. Childhood social economic status and severity of cross-gender behavior were identified as predictors of long-term gender identity outcome. Notwithstanding these empirical gains, a number of questions were still left unresolved. We still do not understand the process through which GID desists. We also do not understand how psychosocial factors interact with the very likely biological predisposition for cross-gender identity/behavior to influence long-term outcome. The role of therapeutics on outcome also remains unclear. It is hoped that future studies will examine the effects, if any, of different therapeutic approaches on persistence and desistence of GID. The present study was the first to systematically assess psychiatric functioning at follow-up. Future follow-up studies should incorporate longer follow-up periods that extend well into adulthood as adolescents and adults with GID appeared to be a psychiatrically vulnerable group, even if the gender dysphoria desists.
Achenbach, T. M. (1985). Assessment and taxonomy of child and adolescent psychopathology. Thousand Oaks, CA: Sage Publications.
Achenbach, T. M. (1991). Manual for the child behavior checklist/4-18 and 1991 profile. Burlington, VT: University of Vermont Department of Psychiatry.
Achenbach, T. M. (1997). Manual for the Young Adult Self Report and Young Adult Behavior Checklist. Burlington, VT: University of Vermont, Department of Psychiatry.
Achenbach, T. M., & Edelbrock, C. (1983). Manual for the child behavior checklist and revised child behavior profile. Burlington, VT: University of Vermont, Department of Psychiatry.
Achenback, T. M., & Edelbrock, C. (1986). Manual for the Youth Self-Report and Profile. Burlington, VT: University of Vermont, Department of Psychiatry.
Achenbach, T. M., Howell, C. T., McConaughy, S. H., & Stanger,C. (1995). Six year predictors of problems in a national sample III: Transitions to young adult syndromes. Journal of the American Academy of Child and Adolescent Psychiatry, 34, 658-669.
Achenbach, T. M., Krukowski, R. A., Dumenci, L., & Ivanova, M. Y. (2005). Assessment of adult psychopathology: Meta-analyses and implications of cross-informant correlations. Psychological Bulletin, 131, 361-382.
Achenbach, T. M., McConaughy, S. H., & Howell, C. T. (1987). Child/adolescent behavior and emotional problems: Implications of cross-informant correlations for situational specificity. Psychological Bulletin, 101, 213-232.
Achenbach, T. M., & Rescorla, L. A. (2003). Manual for ASEBA Adult Forms & Profiles. Burlington, VT: University of Vermont, Research Center for Children, Youth, & Families.
Alanko, K., Santtila, P., Harlaar, N., Witting, K., Varjonen, M., Jern, P., …, & Sandnabba, N. K. (2010). Common genetic effects of gender atypical behavior in childhood and sexual orientation in adulthood: A study of Finnish twins. Archives of Sexual Behavior, 39, 81-92.
Alexander, G. M., & Hines, M. (1994). Gender labels and play styles: Their relative contribution to children’s selections of playmates. Child Development, 65, 869-879.
Almeida, J., Johnson, R. M., Corliss, H. L., Molnar, B. E., & Azrael, D. (2009). Emotional distress among LGBT Youth: The influence of perceived discrimination based on sexual orientation. Journal of Youth and Adolescence, 38, 1001-1014.
American Psychiatric Association. (1980). Diagnostic and statistical manual of mental disorders (3rd ed.). Washington, DC: Author.
American Psychiatric Association. (1987). Diagnostic and statistical manual of mental disorders (3rd ed., rev.). Washington, DC: Author.
American Psychiatric Association. (1994). Diagnostic and statistical manual of mental disorders (4th ed.). Washington, DC: Author.
American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders (4th ed., text rev.). Washington, DC: Author.
Asscheman, H., Giltay, E. J., Megens, J. A. J., de Ronde, W. P., van Trotsenburg, A. A., & Gooren, L. J. G. (2011). A long-term follow-up study of mortality in transsexuals receiving treatment with cross-sex hormones. European Journal of Endocrinology, 164, 635-642.
Anduaga, J. C., Forteza, C. G., & Lira, L. R. (1991). Concurrent validity of the DIS: Experience with psychiatric patients in Mexico City. Hispanic Journal of Behavioral Sciences, 13, 63-77.
Ault, A., & Brzuzy, S. (2009). Commentary: Removing gender identity disorder from the Diagnostic and Statistical Manual of Mental Disorders: A call for action. Social Work, 54, 187-189.
Bailey, J. M. (1999). Homosexuality and mental illness. Archives of General Psychiatry, 56, 883-884.
Bailey, J. M. (2009). What is sexual orientation and do women have one? In: Hope, D. A. (Series Ed.), Nebraska symposium on motivation: Vol. 54. Contemporary perspectives on lesbian, gay, and bisexual identities (pp. 43-64). New York: Springer.
Bailey, J. M., & Bell, A. P. (1993). Familiality of female and male homosexuality. Behavior Genetics, 23, 313-322.
Bailey, J. M., Bobrow, D., Wolfe, M., & Mikach, S. (1995). Sexual orientation of adult sons of gay fathers. Developmental Psychology, 31, 124-129.
Bailey, J. M., Dunne, M. P., & Martin, N. G. (2000). Genetic and environmental influences on sexual orientation and its correlates in an Australian twin sample. Journal of Personality and Social Psychology, 78, 524-536.
Bailey, J. M., Kim., P. Y., Hills, A., & Linsenmeier, J. A. (1997). Butch, femme, or straight acting? Partner preferences of gay men and lesbians. Journal of Personality and Social Psychology, 73, 960-973.
Bailey, J. M., Miller, J. S., & Willerman, L. (1993). Maternally rated gender nonconformity in homosexuals and heterosexuals. Archives of Sexual Behavior, 22, 461-469.
Bailey, J. M., Nothnagel, J., & Wolfe, M. (1995). Retrospectively measured individual differences in childhood sex-typed behaviour among gay men: Correspondence between self- and maternal reports. Archives of Sexual Behavior, 24, 613-622.
Bailey, J. M., & Oberschneider, M. (1997). Sexual orientation and professional dance. Archives of Sexual Behavior, 26, 433-444.
Bailey, J. M, & Pillard, R. C. (1991). A genetic study of male sexual orientation. Archives of General Psychiatry, 48, 1089-1096.
Bailey, J. M, & Pillard, R. C. (1995). Genetics of human sexual orientation. Annual Review of Sex Research, 6, 126-150.
Bailey, J. M., Pillard, R. C., Dawood, K., Miller, M. B., Farrer, L. A., Trivedi, S., & Murphy, R. L. (1999). A family history of male sexual orientation. Behavior Genetics, 29, 79-86.
Bailey, J. M., Willerman, L., & Parks, C. (1991). A test of the maternal stress theory of human male homosexuality. Archives of Sexual Behavior, 20, 277-293.
Bailey, J. M., & Zucker, K. J. (1995). Childhood sex-typed behaviour and sexual orientation: A conceptual analysis and quantitative review. Developmental Psychology, 1, 43-55.
Bakker, A., van Kesteren, P. J. M., Gooren, L. J. G., & Bezemer, P. D. (1993). The prevalence of transsexualism in the Netherlands. Acta Psychiatrica Scandinavica, 87, 237-238.
Bakwin, H. (1968). Deviant gender-role behavior in children: Relation to homosexuality. Pediatrics, 41, 620-629.
Barber, M. E. (2000). Examining differences in sexual expression and coming out between lesbians and gay men. Journal of the Gay and Lesbian Medical Association, 4, 167-174.
Bartlett, N. H., & Vasey, P. L. (2006). A retrospective study of childhood gender-atypical behavior in Samoan fa’afafine. Archives of Sexual Behavior, 35, 559-566.
Bartlett, N. H., Vasey, P. L., & Bukowksi, W. M. (2000). Is gender identity disorder in children a mental disorder? Sex Roles, 43, 753-785.
Bates, J. E., Skilbeck, W. M., Smith, K. V. R., & Bentler, P. M. (1974). Gender role abnormalities in boys: An analysis of clinical ratings. Journal of Abnormal Child Psychology, 2, 1-16.
Beaty, L. A. (1999). Identity development of homosexual youth and parental and family influences on the coming out process. Adolescence, 34, 597-601.
Beautrais, A. L. (2003). Suicide and serious suicide attempts in youth: A multiple-group comparison study. American Journal of Psychiatry, 160, 1093-1099.
Bem, D. J. (1996). Exotic becomes erotic: A developmental theory of sexual orientation. Psychological Review, 103, 320-335.
Bem, D. J. (2008). The exotic becomes erotic: A review of theory and research. Journal of Gay & Lesbian Mental Health, 12, 61-79.
Berenbaum, S. A. (1999). Effects of early androgens on sex-typed activities and interests in adolescents with congenital adrenal hyperplasia. Hormones and Behavior, 35, 102-110.
Berenbaum, S. A., & Hines, M. (1992). Early androgens are related to childhood sex-typed toy preferences. Psychological Science, 2, 203-206.
Berenbaum, S. A., & Snyder, E. (1995). Early hormonal influences on childhood sex-typed activity and playmate preferences: Implications for the development of sexual orientation. Developmental Psychology, 1, 31-42.
Berrill, K. (1990). Anti-gay violence and victimization in the United States: An overview. Journal of Interpersonal Violence, 5, 274-294.
Blakemore, J. E. O. (2003). Children’s beliefs about violating gender norms: Boys should look like girls, and girls shouldn’t act like boys. Sex Roles, 48, 411-419.
Bockting, W. O. (1997). The assessment and treatment of gender dysphoria. Directions in Clinical and Counselling Psychology, 7, 1-22.
Bockting, W. O. (2009). Are gender identity disorders mental disorders? Recommendations for revision of the World Professional Association for Transgender Health’s Standards of Care. International Journal of Transgenderism, 11, 53-62.
Bockting, W. O., & Ehrbar, R. D. (2005). Commentary: Gender variance, dissonance, or identity disorder? Journal of Psychology & Human Sexuality, 17, 125-134.
Bodlund, O., & Armelius, K. (1994). Self-image and personality traits in gender identity disorders: An empirical study. Journal of Sex & Marital Therapy, 20, 303-317.
Boegart, A. F. (2003). Interaction of older brothers and sex-typing in the prediction of sexual orientation in men. Archives of Sexual Behavior, 32, 129-134.
Bolton, S.-L., & Sareen, J. (2011). Sexual orientation and its relation to mental disorders and suicide attempts: Findings from a nationally representative sample. The Canadian Journal of Psychiatry, 56, 35-43.
Bontempo, D. E., & D’Augelli, A. R. (2002). Effects of at-school victimization and sexual orientation on lesbian, gay, or bisexual youths’ health risk behaviour. Society for Adolescent Medicine, 30, 364-374.
Bower, H. (2001). The gender identity disorders in the DSM-IV classification: A critical evaluation. Australian and New Zealand Journal of Psychiatry, 35, 1-8.
Bradley, R. H., & Corwyn, R. F. (2002). Socioeconomic status and child development. Annual Review of Psychology, 53, 371-399.
Bradley, S. J. (1998). Assessment of sexual and gender development in adolescents. In S. I. Harrison & S. Eth (Eds.), Handbook of child and adolescent psychiatry (pp. 252-258). New York: John Wiley & Sons.
Bradley, S. J. (1999). Gender dysphorias of childhood and adolescence. In B. D. Garfinkel, G. A. Carlson, & E. B. Weller (Eds.), Psychiatric disorders in children and adolescents (pp. 121-134). Philadelphia: Saunders
Bradley, S. J., Blanchard, R., Coates, S., Green, R., Levine, S. B., Meyer-Bahlburg, H. F. L.,…Zucker, K. J. (1991). Interim report of the DSM-IV Subcommittee on Gender Identity Disorders. Archives of Sexual Behavior, 20, 333-343.
Bradley, S. J., & Zucker, K. J. (1997). Gender identity disorder: A review of the past 10 years. Journal of the American Academy of Child and Adolescent Psychiatry, 36, 872-880.
Bradley, S. J., & Zucker, K. J. (1998). Gender identity disorder [Letter to the Editor].
Journal of the American Academy of Child and Adolescent Psychiatry, 37, 244-246.
Bradley, S. J., & Zucker, K. J. (2003). Children with gender nonconformity [Letter to the Editor]. Journal of the American Academy of Child and Adolescent Psychiatry, 42, 266-268.
Brender, N. C., Kann, L., McManus, T., Kinchen, S. A., Sundberg, E. C., & Ross, J. G. (2002). Reliability of the 1999 Youth Risk Behavior Survey Questionnaire. Journal of Adolescent Health, 31, 336-342.
Brill, S., & Pepper, R. (2008). The transgender child: A handbook for families and professionals. San Francisco, CA: Cleis Press.
Brown, P. L. (2006, December 2). Supporting boys or girls when the line isn’t clear. New York Times, pp. A1, A11.
Bryant, K. (2006). Making gender identity disorder of childhood: Historical lessons for contemporary debates. Sexuality Research and Social Policy, 3, 23-39.
Burn, S. M., Kadlec, K., & Rexer, R. (2005). Effects of subtle heterosexism on gays, lesbians, and bisexuals. Journal of Homosexuality, 49, 23-38.
Campbell, D. T., & Stanley, J. C. (1963). Experimental and quasi-experimental designs for research. Chicago: Rand McNally & Company.
Cardoso, F. L. (2009). Recalled sex-typed behavior in childhood and sports’ preferences in adulthood of heterosexual, bisexual, and homosexual men from Brazil, Turkey, and Thailand. Archives of Sexual Behavior, 38, 726-736.
Carlson, G. A., Kashani, J. H., Thomas, M. D. F., Vaidya, A., & Daniel, A. E. (1987). Comparison of the DISC and the K-SADS interviews in an epidemiological sample of children. Journal of the American Academy of Child and Adolescent Psychiatry, 26, 645-648.
Caron, C., & Rutter, M. (1991). Comorbidity in child psychopathology: Concepts, issues, and research strategies. Journal of Child Psychology and Psychiatry, 32, 1063-1080.
Carrier, J. M. (1986). Childhood cross-gender behavior and adult homosexuality [Letter to the Editor]. Archives of Sexual Behavior, 15, 89-93.
Carver, P. R., Yunger, J. L., & Perry, D. G. (2003). Gender identity and adjustment in middle school. Sex Roles, 49, 95-109.
Centers for Disease Control. (2002). Trends in sexual risk behaviors among high school students-United States, 1991-2001. Mortality of Morbidity Weekly Reviews, 51, 856-859.
Chivers, M. L., Rieger, G., Latty, E., & Bailey, J. M. (2004). A sex difference in the specificity of sexual arousal. Psychological Science, 15, 736-744.
Cicchetti, D., & Rogosch, F. A. (1996). Equifinality and multifinality in developmental psychopathology. Development and Psychopathology, 8, 597-600.
Clements-Nolle, K., Marx, R., & Katz, M. (2006). Attempted suicide among transgender persons: The influence of gender-based discrimination and victimization. Journal of Homosexuality, 51, 53-69.
Coates, S., & Person, E. S. (1985). Extreme boyhood femininity: Isolated behavior or pervasive disorder? Journal of the American Academy of Child Psychiatry, 24, 702-709.
Coates, S., & Wolfe, S. (1997). Gender identity disorders of childhood. In J. D. Noshpitz (Ed.) and S. Greenspan, S. Wieder, & J. Osofsky (Vol. eds.), Handbook of child and adolescent psychiatry: Vol. I. Infants and preschoolers: Development and syndromes (pp. 453-472). New York: Wiley.
Cochran, S. D. (2001). Emerging issues in research on lesbians’ and gay men’s mental health: Does sexual orientation really matter? American Psychologist, 56, 931-947.
Cochran, S. D., & Mays, V. M. (2000). Lifetime prevalence of suicide symptoms and affective disorders among men reporting same-sex sexual partners: Results from NHANES III; American Journal of Public Health, 90, 573-578.
Cochran, S. D., Sullivan, J. G., & Mays, V. M. (2003). Prevalence of mental disorders, psychological distress, and mental health services use among lesbian, gay and bisexual adults in the United States. Journal of Consulting and Clinical Psychology, 71, 53-61.
Cohen, J. (1988). Statistical power analysis for the behavioral sciences (2nd ed.) Hillsdale, NJ: Erlbaum.
Cohen, K. M. (2002). Relationships among childhood sex-atypical behavior, spatial ability, handedness, and sexual orientation in men. Archives of Sexual Behavior, 31, 129-143.
Cohen-Kettenis, P. T. (2001). Gender identity disorder in DSM? [Letter to the Editor]. Journal of the American Academy of Child and Adolescent Psychiatry, 40, 391.
Cohen-Kettenis, P. T., Delemarre-van de Waal, H. A., & Gooren, L. J. G. (2008). The treatment of adolescent transsexuals: Changing insights. Journal of Sexual Medicine, 5, 1892-1897.
Cohen-Kettenis, P. T., & Gooren, L. J. G. (1999). Transsexualism: A review of etiology, diagnosis, and treatment. Journal of Psychosomatic Research, 46, 315-333.
Cohen-Kettenis, P. T., Owen, A., Kaijser, V. G., Bradley, S. J., & Zucker, K. J. (2003). Demographic characteristics, social competence, and behavior problems in children with gender identity disorder: A cross-national, cross-clinic comparative analysis. Journal of Abnormal Psychology, 31, 41-53.
Cohen-Kettenis, P. T., & Pfäfflin, F. (2003). Transegenderism and intersexuality in childhood and adolescence: Making choices. Thousand Oaks, CA: Sage.
Cohen-Kettenis, P. T., & Pfäfflin, F. (2010). The DSM diagnostic criteria for gender identity disorder in adolescents and adults. Archives of Sexual Behavior, 39, 499-513.
Cohen-Kettenis, P. T., & van Goozen, S. H. M. (1997). Sex reassignment of adolescent transsexuals: A follow-up study. Journal of the American Academy of Child and Adolescent Psychiatry, 36, 263-271.
Cohen-Kettenis, P. T., Wallien, M., Johnson, L. L., Owen-Anderson, A. F. H., Bradley, S. J., & Zucker, K. J. (2006). A parent-report Gender Identity Questionnaire for children: A cross-national, cross-clinic comparative analysis. Clinical Child Psychology and Psychiatry, 7, 433-456.
Cole, C. M., O'Boyle, M., Emory, L. E., & Meyer, W. J. (1997). Comorbidity of gender dysphoria and other major psychiatric diagnoses. Archives of Sexual Behavior, 26, 13-26.
Compton, W. M., & Cottler, L. B. (2004). The Diagnostic Interview Schedule (DIS). In M. Hersen (Ed.) and M. Hilsenroth, & D. L. Segal (Vol. eds.), Personality assessment, Vol. 2: Comprehensive handbook of psychological assessment (pp. 153-162). Hokoken, NJ: Wiley.
Corbett, K. (1998). Cross-gendered identifications and homosexual boyhood: Toward a more complex theory of gender. American Journal of Orthopsychiatry, 68, 352–360.
Clements-Nolle, K., Marx, R. & Katz, M. (2006). Attempted suicide among transgendered persons: The influence of gender based discrimination and victimization. Journal of Homosexuality, 51, 53-69.
Crowne, D. P., & Marlowe, D. (1960). A new scale of social desirability independent of psychopathology. Journal of Consulting Psychology, 24, 349-354.
Dalsgaard, S., Mortensen, P. B., Frydenberg, M., & Thomsen, P. H. (2002). Conduct problems, gender, and adult psychiatric outcome of children with attention-deficit hyperactivity disorder. British Journal of Psychiatry, 181, 416-421.
Dascalu, M., Compton, W.M., Horton, J. C., & Cottler, L. B. (2001). Validity of DIS-IV in diagnosing depression and other psychiatric disorders among substance users. Drug and Alcohol Dependence, 63(S), 37.
D’Augelli, A. R. (2002). Mental health problems among lesbian, gay, and bisexual youths ages 14-21. Clinical Child Psychology and Psychiatry, 7, 433-456.
D’Augelli, A. R. (2006). Developmental and contextual factors and mental health among lesbian, gay, and bisexual youths. In A. M. Omoto & H. S. Kurtzman (Eds.), Sexual orientation and mental health: Examining identity and development in lesbian, gay, and bisexual people (pp. 37-54). Washington, DC: American Psychological Association.
D'Augelli, A. R., & Grossman, A. H. (2001). Disclosure of sexual orientation, victimization, and mental health among lesbian, gay, and bisexual older adults. Journal of Interpersonal Violence, 16, 1008-1027.
D’Augelli, A. R., & Hershberger, S. L. (1993). Lesbian, gay, and bisexual youth in community settings: Personal challenges and mental health problems. American Journal of Community Psychology, 21, 421-448.
D’Augelli, A. R., Hershberger, S. L., & Pilkington, N. W. (1998). Lesbian, gay, and bisexual youth and their families: Disclosure of sexual orientation and its consequences. American Journal of Orthopsychiatry, 68, 361-371.
D’Augelli, A. R., Hershberger, S. L., & Pilkington, N. W. (2001). Suicidality patterns and sexual orientation-relate factors among lesbian, gay, and bisexual youths. Suicide and Life-Threatening Behavior, 31, 250-264.
D'Augelli, A. R., Pilkington, N. W., & Hershberger, S. L. (2002). Incidence and mental health impact of sexual orientation victimization of lesbian, gay, and bisexual youths in high school. School Psychology Quarterly, 17, 148-167.
Davenport, C. W. (1986). A follow-up study of 10 feminine boys. Archives of Sexual Behavior, 15, 511-517.
De Cuypere, G., Jannes, C., & Rubens, R. (1995). Psychosocial functioning of transsexuals in Belgium. Acta Psychiatrica Scandinavica, 91, 180-184.
De Cuypere, G. T., T’Sjoen, G., Beerten, R., Selvaggi, G., De Sutter, P., Hoebeke, P.,…Rubens, R. (2007). Sexual and physical health after sex reassignment surgery, Archives of Sexual Behavior, 34, 679-690.
De Cuypere, G. T., Van Hemelrijck, M., Michel, A., Carael, B., Heylens, G., Rubens, R.,…Monstrey, S. (2007). Prevalence and demography of transsexualism in Belgium. European Psychiatry, 22, 137-141.
Dessens, A. B., Slijper, F. M. E., & Drop, S. L. S. (2005). Gender dysphoria and gender change in chromosomal females with congenital adrenal hyperplasia. Archives of Sexual Behavior, 34, 389-397.
de Vries, A. L. C., & Cohen-Kettenis, P. T. (2012). Clinical management of gender dysphoria in children and adolescents: The Dutch approach. Journal of Homosexuality, 59, 301-320.
de Vries, A. L. C., Doreleijers, T. A., Steensma, T. D., & Cohen-Kettenis, P. T. (2011b). Psychiatric comorbidity in gender dysphoric adolescents. Journal of Child Psychology and Psychiatry, 52, 1195-1202.
de Vries, A. L. C., Noens, I. L., Cohen-Kettenis, P. T., van Berckelaer-Onnes, I. A., & Doreleijers, T. A. H. (2010). Autism spectrum disorders in gender dysphoric children and adolescents. Journal of Autism and Developmental Disorders, 40, 930-936.
de Vries, A. L. C., Steensma, T. D., Doreleijers, T. A., & Cohen-Kettenis, P. T. (2011a). Puberty suppression in adolescents with gender identity disorder: A prospective follow-up study. Journal of Sexual Medicine, 8, 2276-2283.
Deogracias, J. J., Johnson, L. L., Meyer-Bahlburg, H. F. L., Kessler, S. J., Schober, J. M., & Zucker, K. J. (2007). The Gender Identity/Gender Dysphoria Questionnaire for Adolescents and Adults. Journal of Sex Research, 44, 370-379.
Dhejne, C., Lichtenstein, P., Boman, M., Johansson, A. L. V., Långström, N., & Lande, N. (2011). Long-term follow-up of transsexual persons undergoing sex reassignment surgery: Cohort study in Sweden. PLoS One, 6, e16885.
Diamond, M. (1993). Homosexuality and bisexuality in different populations. Archives of Sexual Behavior, 22, 291-310.
Diamond, L. M. (2000). Sexual identity, attractions, and behavior among young sexual-minority women over a 2-year period. Developmental Psychology, 36, 241-250.
Diamond, M. (2002). Sex and gender are different: Sexual identity and gender identity are different. Clinical Child Psychology and Psychiatry, 7, 320-334.
Dreger, A. (2009). Gender identity disorder in children: Inconclusive advice to parents. Hastings Center Report, 39, 26-29.
Drescher, J. (2010a). Queer diagnoses: Parallels and contrasts in the history of homosexuality, gender variance, and the Diagnostic and Statistical Manual. Archives of Sexual Behavior, 39, 427-460.
Drescher, J. (2010b). Transsexualism, gender identity disorder and the DSM. Journal of Gay & Lesbian Mental Health, 14, 109-122.
Drescher, J., & Byne, W. (2012). Gender dysphoric/gender variant (GD/DV) children and adolescents: Summarizing what we know and what we have yet to learn. Journal of Homosexuality, 59, 501-510.
Drummond, K. D. (2006). A follow-up study of girls with gender identity disorder. Unpublished master’s thesis, Ontario Institute for Studies in Education of the University of Toronto, Toronto, Ontario, Canada.
Drummond, K. D., Bradley, S. J., Peterson-Badali, M., & Zucker, K. J. (2008). A follow-up study of girls with gender identity disorder. Developmental Psychology, 44, 34-45.
Edwards-Leeper, L., & Spack, N. P. (2012). Psychological evaluation and medical treatment of transgender youth in an interdisciplinary “Gender Management Service” (GeMS) in a major pediatric center. Journal of Homosexuality, 59, 321-336.
Egan, S. K., & Perry, D. G. (2001). Gender identity: A multidimensional analysis with implications for psychosocial adjustment. Developmental Psychology, 37, 451-463.
Ehrensaft, D. (2011). “I’m a Prius”: A child case of a gender/ethnic hybrid. Journal of Gay & Lesbian Mental Health, 15, 46-57.
Ehrensaft, D. (2012). From gender identity disorder to gender identity creativity: True gender self child therapy. Journal of Homosexuality, 59, 337-356.
English, B. (2011, December). Led by the child who simply knew. The Boston Globe. Retrieved January 07, 2012 from www.bostonglobe.com.
Erlenmeyer-Kimling, L., Adamo, U. H., Rock, D., Roberts, S. A., Bassett, A. S., Squires-Wheeler, E.,…Gottesman, I. I. (1997). The New York High-Risk Project: Prevalence and comorbidity of Axis I disorders in offspring of schizophrenic parents at 25 year follow-up. Archives of General Psychiatry, 54, 1096-1102.
Ezpeleta, L., Osa, N., Domenech, J. M., Navarro, J. B., Losilla, J. M., & Judez, J. (1997). Diagnostic agreement between clinicians and the Diagnostic Interview for Children and Adolescents-DICA-R-in an outpatient sample. Journal of Child Psychology and Psychiatry, 38, 431-440.
Factor, R. J., & Rothblum, E. D. (2007). A study of transgender adults and their non-transgender siblings on demographic characteristics, social support, and experiences of violence. Journal of Lesbian, Gay, Bisexual and Transgender Research, 3, 11-30.
Fagot, B. I. (1977). Consequences of moderate cross-gender behaviour in preschool children. Child Development, 48, 902-907.
Fagot, B. I. (1985). Changes in thinking about early sex role development. Developmental Review, 5, 83-98.
Fagot, B. I., & Leinbach, M. D. (1985). Gender identity: Some thoughts on an old concept. Journal of the American Academy of Child Psychiatry, 24, 6894-688.
Fagot, B. I., Leinbach, M. D., & Hagan, R., (1986). Gender labelling and adoption of sex-typed behaviors. Developmental Psychology, 22, 440-443.
Farrell, R., & Morrione, T. (1974). Social interaction and stereotypic responses to homosexuals. Archives of Sexual Behavior, 3, 425-442.
Faulkner, A. H., & Cranston, K. (1998). Correlates of same-sex sexual behaviour in a random sample of Massachusetts high school students. American Journal of Public Health, 88, 262-266.
Ferdinand, R. F., & Verhulst, F. C. (1995). Psychopathology from adolescence into young adulthood: an 8-year follow-up study. American Journal of Psychiatry, 152, 1586-1594.
Ferdinand, R. F., Verhulst, F. C., & Wiznitzer, M. (1995). Continuity and change of self-reported problem behaviors from adolescence into young adulthood. Journal of the American Academy of Child and Adolescent Psychiatry, 34, 680-690.
Fergusson, D. M., Horwood, J., & Beautrais, A. L. (1999). Is sexual orientation related to mental health problems and suicidality in young people? Archives of General Psychiatry, 56, 876-880.
Fisk, N. (1973). Gender dysphoria syndrome (the how, why, and what of a disease). In D. Laub & P. Gandy (Eds.), Proceedings of the second interdisciplinary symposium on gender dysphoria syndrome (pp. 7-14). Stanford, CA: Stanford University Press.
Fitzpatrick, K. K., Euton, S. J., Jones, J. N., & Schmidt, N. B. (2005). Gender role, sexual orientation, and suicide risk. Journal of Affective Disorders, 87, 35-42.
Floyd, F. J., & Bakeman, R. (2006). Coming-out across the life-course: Implications of age and historical context. Archives of Sexual Behavior, 35, 287-296.
Fridell, S. R. (2001). Sex-typed play behaviour and peer relationships of boys with gender identity disorder. Unpublished doctoral dissertation, University of Toronto, Ontario, Canada.
Fridell, S. R., Owen-Anderson, A., Johnson, L. L., Bradley, S. J., & Zucker, K. J. (2006). The Playmate and Play Style Preferences Structured Interview: A comparison of children with gender identity disorder and controls. Archives of Sexual Behavior, 35, 729-737.
Fridell, S. R., Zucker, K. J., Bradley, S. J., & Maing, D. M. (1996). Physical attractiveness of girls with gender identity disorder. Archives of Sexual Behavior, 25, 17-31.
Frisell, T., Lichtenstein, P., Rahman, Q., & Långström, N. (2010). Psychiatric morbidity associated with same-sex sexual behaviour: influence of minority stress and familial factors. Psychological Medicine, 40, 315-324.
Gad, M., & Johnson, J. (1980). Correlates of adolescent life stresses related to race, SES, and levels of perceived support. Journal of Clinical Child Psychology, 9, 13-16.
Geller, B., Fox, L. W., & Clark, K. A. (1994). Rate and predictors of prepubertal bipolarity during follow-up of 6- to 12-year-old depressed children. Journal of the American Academy of Child and Adolescent Psychiatry, 33, 461-468.
Gilman, S. E., Cochran, S. D., Mays, V. M., Hughes, M., Ostrow, D., & Kessler, R. C. (2001). Risk of psychiatric disorders among individuals reporting same-sex sexual partners in the National Comorbidity Survey. American Journal of Public Health, 91, 933-939.
Glenn, C. R., & Klonsky, E. D. (2010). A multimethod analysis of impulsivity in nonsuicidal self-injury. Personality Disorders, 1, 67-75.
Glenn, N. D., & Weaver, C. N. (1979). Attitudes towards premarital, extramarital, and homosexual relations in the U.S. in the 1970’s. Journal of Sex Research, 15, 108-118.
Gómez-Gil, E., Trilla, A., Salamero, M., Godás, T., & Valdéa, M. (2009). Sociodemographic, clinical, and psychiatric characteristics of transsexuals from Spain. Archives of Sexual Behavior, 38, 378-392.
Gottschalk, L. (2003). Same-sex sexuality and childhood gender non-conformity: A spurious connection. Journal of Gender Studies, 12, 35-50.
Goy, R. W., Bercovitch, F. B., & McBriar, M. C. (1988). Behavioral masculinisation is independent of genital masculinisation in prenatally androgenised female rhesus macaques. Hormones and Behavior, 22, 552-571.
Green, R. (1970). Sex reassignment: A research strategy. International Journal of Psychiatry, 9, 269-273.
Green, R. (1974). Sexual identity conflict in children and adults. New York: Basic Books.
Green, R. (1976). One-hundred ten feminine and masculine boys: Behavioral contrasts and demographic similarities. Archives of Sexual Behavior, 5, 425-446.
Green, R. (1987). The “sissy boy syndrome” and the development of homosexuality. New Haven, CT: Yale University Press.
Green, R. (2008). Childhood cross-gender behavior and adult homosexuality: Why the link? Journal of Gay & Lesbian Mental Health, 12, 17-28.
Green, R. (2011). The introduction of gender identity disorder of childhood into DSM-III: An historical note. Journal of Gay & Lesbian Mental Health, 15, 8-11.
Green, R., & Money, J. (1960). Incongruous gender role. Nongenital manifestations in prepubertal boys. Journal of Nervous and Mental Disease, 131, 160-168.
Green, R., Roberts, C. W., Williams, K., Goodman, M., & Mixon, A. (1987). Specific cross-gender behavior in boyhood and later homosexual orientation. British Journal of Psychiatry, 151, 84-88.
Grossman, A. H., & D’Augelli, A. R. (2007). Transgender youth and life-threatening behaviors. Suicide and Life-Threatening Behavior, 37, 527-537.
Grossman, A. H., D’Augelli, A. R., & Salter, N. P. (2006). Male-to-female transgender youth: Gender expression milestones, gender atypicality, victimization, and parents’ responses. Journal of GLBT Family Studies, 2, 71-92.
Grov, C., Bimbi, D. S., Nanin, J. E., & Parsons, J. T. (2006). Race, ethnicity, gender, and generational factors associated with the coming out process among gay, lesbian, and bisexual individuals. Journal of Sex Research, 43, 115-212.
Haas, A. P., Eliason, M., Mays, V. M., Mathy, R. M., Cochran, S. D., D’Augelli, A. R.,…Clayton, P. J. (2011). Suicide and suicide risk in lesbian, gay, bisexual, and transgender populations: Review and recommendations. Journal of Homosexuality, 58, 10-51.
Halpert, S. C. (2002). Suicidal behavior among gay male youth. Journal of Gay and Lesbian Psychotherapy, 6, 53-79.
Haraldsen, I. R., & Dahl, A. A. (2000). Symptom profiles of gender dysphoric patients of transsexual type compared to patients with personality disorders and healthy adults. Acta Psychiatrica Scandinavica, 102, 276-281.
Hardt, J., & Rutter, M. (2004). Validity of adult retrospective reports of adverse childhood experiences: review of the evidence. Journal of Child Psychology and Psychiatry, 45, 260-273.
Harry, J. (1985a). Sexual orientation as destiny. Journal of Homosexuality, 10, 111-124.
Harry, J. (1985b). Defeminization and social class. Archives of Sexual Behavior, 14, 1-12.
Heatherington, L., & Lavner, J. A. (2008). Coming to terms with coming out: Review and Recommendations for Family Systems-Focused Research. Journal of Family Psychology, 22, 329-343.
Hellman, R. E., Green, R., Gray, J. L., & Williams, K. (1981). Childhood sexual identity, childhood religiosity, and ‘homophobia’ as influences in the development of transsexualism, homosexuality, and heterosexuality. Archives of General Psychiatry, 38, 910-915.
Helzer, J. E., Robins, L. N., McEnvoy, L. T., Spitznagel, E. L., Stoltzman, R. K., Farmer, A., & Brockington, I. F. (1985). A comparison of clinical and Diagnostic Interview Schedule diagnoses. Archives of General Psychiatry, 42, 657-666.
Hepp, U., Kraemer, B., Schnyder, U., Miller, N., & Delsignore, A. (2005). Psychiatric comorbidity in gender identity disorder. Journal of Psychosomatic Research, 58, 259-261.
Herek, G. M., & Capitanio, J. P. (1996). ‘‘Some of my best friends’’: Intergroup contact, concealable stigma, and heterosexuals’ attitudes toward gay men and lesbians. Personality and Social Psychology Bulletin, 22, 412-424.
Herek, G. M., Cogan, J. C., Gillis, J. R., & Glunt, E. K. (1998). Correlates of internalized homophobia in a community sample of lesbians and gay men. Journal of the Gay and Lesbian Medical Association, 2, 17-25.
Herek, G. M., Gillis, J. R., Cogan, J. C., & Glunt, E. K. (1997). Hate crime victimization among lesbian, gay and bisexual youth. Journal of Interpersonal Violence, 12, 195-215.
Herek, G. M., & Glunt, E. K. (1993). Interpersonal contact and heterosexuals’ attitudes toward gay men: Results from a national survey. Journal of Sex Research, 30, 239-244.
Herjanic, B., & Reich, W. (1982). Development of a structured psychiatric interview for children: Agreement between child and parent on individual symptoms. Journal of Abnormal Child Psychology, 10, 307-324.
Herjanic, B., & Reich, W. (1983). Diagnostic Interview for Children and Adolescents (DICA-C): Child version. St. Louis, MO: Washington University School of Medicine.
Hershberger, S. L. (1997). A twin registry study of male and female sexual orientation. Science, 261, 321-327.
Hesselbrock, V., Stabenau, J., Hesslebrock, M., Mirkin, P., & Meyer, R. (1982). A comparison of two interview schedules: The Schedule for Affective Disorders and Schizophrenia-Lifetime and the National Institute of Mental Health Diagnostic Interview Schedule. Archives of General Psychiatry, 39, 674-677.
Hill, S. A. (2002). Teaching and doing gender in African American families. Sex Roles, 47, 493-506.
Hill, D. B., Rozanski, C., Carfagnini, J., & Willoughby, B. (2005). Gender identity disorders in childhood and adolescence: A critical inquiry. Journal of Psychology & Human Sexuality, 17, 7-34.
Hines, M. (2002). Sexual differentiation of human brain and behaviour. In D. W. Plaff, A. P. Arnold, A. M. Etgen, S. E. Fahrbach, & R. T. Rubin (Eds.), Hormones, brain, and behaviour (Vol. 4, pp. 425-262). San Diego, CA: Academic Press.
Hines, M. (2010). Gendered behavior across the lifespan. In R. M. Lerner (Ed.), The handbook of life-span development (Vol. 2, pp. 341-378). New York: Wiley.
Hines, M. (2011). Gender development and the human brain. Annual Review of Neuroscience, 34, 69-88.
Hines, M., Brook, C., & Conway, G. S. (2004). Androgen and psychosexual development: core gender identity, sexual orientation and recalled childhood gender role behavior in women and men with congenital adrenal hyperplasia (CAH). Journal of Sex Research, 41, 75-81.
Hoenig, J., Kenna, J., & Youd, A. (1970). Social and economic aspects of transsexualism. British Journal of Psychiatry, 117, 163-172.
Hofstra, M. B., van der Ende, J., & Verhulst, F. C. (2000). Continuity and change of psychopathology from childhood into adulthood: A 14-year follow-up study. Journal of the American Academy of Child & Adolescent Psychiatry, 39, 850-858.
Hofstra, M. B., van der Ende, J., & Verhulst, F. C. (2001). Child and adolescent problems predict DSM-IV disorders in adulthood: A 14-year follow-up of a Dutch Epidemiological Sample. Journal of the American Academy of Child & Adolescent Psychiatry, 341, 182-189.
Holden, R. R., & Fekken, G. C. (1989). Three common social desirability scales: Friends, acquaintances, or strangers? Journal of Research in Personality, 23, 180-191.
Hollingshead, A. B. (1975). Four factor index of social status. (Unpublished manuscript). Department of Sociology, Yale University, New Haven, CT.
Hollingshead, A. B., & Redlich, F. C. (1958). Social class and mental illness. New York: Wiley.
Horton, J., Compton, W. M., & Cottler, L. B. (1998). Assessing psychiatric disorders among drug users: reliability of the revised DIS-IV (abstract). In L. Harris (Ed.), NIDA research monograph: Problems of drug dependence (p. 205). Washington, DC: NIH.
Hoshiai, M., Matsumoto, Y., Sato, T., Ohnishi, M., Okabe, N., Kishimoto, Y.,…Kurodo, S. (2010). Psychiatric comorbidity among patients with gender identity disorder. Psychiatry and Clinical Neurosciences, 64, 514-519.
Hoult, T. (1983/1984). Human sexuality in biological perspective. Journal of Homosexuality, 9, 137-156.
Hudson, C. G. (1988). Socioeconomic status and mental illness: Implications of the research for policy and practice. Journal of Sociology and Social Welfare, 15, 27-54.
Hudson, C. G. (2005). Socioeconomic status and mental illness: Tests of the social causation and selection hypotheses. American Journal of Orthopsychiatry, 75, 3-18.
Irwin, P., & Thompson, N. L. (1977). Acceptance of the rights of homosexuals: A social profile. Journal of Homosexuality, 3, 107-121.
Isay, R. A. (1997, November 21). Remove gender identity disorder in DSM. Psychiatric News, 32(22), 9-13.
Jacobson, C. M., & Gould, M. (2007). The epidemiology and phenomenology of non-suicidal self-injurious behavior among adolescents: A critical review of the literature. Archives of Suicide Research, 11, 127-147.
Jenkins, J. (2008). Psychosocial adversity and resilience. In M. Rutter, D. V. M. Bishop, D. S. Pine, S. Scott, J. Stevenson, E. Taylor, & A. Thapar (Eds.), Rutter’s child and adolescent psychiatry (pp. 377-391). Oxford: Blackwell Publishing.
Jensen, L., Gambles, D., & Olsen, J. (1988). Attitudes towards homosexuality: A cross-cultural analysis of predictors. The International Journal of Social Psychiatry, 34, 47-57.
Johnson, L. L., Bradley, S. J., Birkenfeld-Adams, A. S., Kuksis, M. A. R., Maing, D. M., Mitchell, J. N., et al. (2004). A parent-report Gender Identity Questionnaire for Children. Archives of Sexual Behavior, 33, 105-116.
Jolles, I. (1952). A study of validity of some hypotheses for the qualitative interpretation of the H-T-P for children of elementary school age: I. Sexual identification. Journal of Clinical Psychology, 8, 113-118.
Kallman, F. J. (1952). Twin and sibship study of overt male homosexuality. American Journal of Human Genetics, 4, 136-146.
Kessler, R. C., Borges, G., & Walters, E. E. (1999). Prevalence and risk factors for lifetime suicide attempts in the National Comorbidity Survey. Archives of General Psychiatry, 56, 617-626.
Kessler, S. J., & McKenna, W. (1978). Gender: An ethnomethodological approach. Chicago: University of Chicago Press.
Kilpatrick, D. G., Saunders, B. E., & Smith, D. W. (2002). Research in brief: Youth victimization: Prevalence and implications. Washington, DC: U.S. Department of Justice, National Institute of Justice.
King, M. F., & Brunner, G. C. (2000). Social desirability bias: A neglected aspect of validity testing. Psychology and Marketing, 17, 79-103.
King, M., Semlyen, J., Tai, S. S., Killaspy, H., Osborn, D., Popelyuk, D., et al. (2008). A systematic review of mental disorder, suicide, and deliberate self-harm in lesbian, gay and bisexual people. BMC Psychiatry, 8. doi:10.1186/1471-244X-8-70.
Kinsey, A. C., Pomeroy, W. B., & Martin, C. E. (1948). Sexual behavior in the human male. Philadelphia: W. B. Saunders.
Kirk, K. M., Bailey, J. M., Dunne, M. P., & Martin, N. G. (2000). Measurement models for sexual orientation in a community twin sample. Behavior Genetics, 30, 345-356.
Klin, A., Danovitch, J. H., Merz, A. B., & Volkmar, F. R. (2007). Circumscribed interests in higher functioning individuals with autism spectrum disorders: An exploratory study. Research & Practice for Persons with Severe Disabilities, 32, 89-100.
Kosky, R. J. (1987). Gender-disordered children: Does inpatient treatment help? Medical Journal of Australia, 146, 565-569.
Kulkin, H. S., Chauvin, E. A., & Percle, G. A. (2000). Suicide among gay and lesbian adolescents and young adults. A review of the literature. Journal of Homosexuality, 40, 1-29.
Lambert, S. L. (2009). The assessment of body image in boys with gender identity disorder: A comparison to clinical control boys and community control boys. Unpublished doctoral dissertation, York University, Toronto, Ontario, Canada.
Landén, M., & Rasmussen, P. (1997). Gender identity disorder in a girl with autism: A case report. European Child & Adolescent Psychiatry, 6, 170-173.
Landolt, M. A., Bartholomew, K., Saffrey, C., Oram, D., & Perlman, D. (2004). Gender nonconformity, childhood rejection, and adult attachment: A study of gay men. Archives of Sexual Behavior, 33, 117-128.
Langer, S. J., & Martin, J. I. (2004). How dresses can make you mentally ill: Examining gender identity disorder in children. Child and Adolescent Social Work Journal, 21, 5-23.
Langevin, R. (1985). Sexual strands: Understanding and treating sexual anomalies in men. Hillsdale, NJ: Erlbaum.
Längström, N., Rahman, Q., Carlström, E., & Lichtenstein, P. (2010). Genetic and environmental effects on same-sex sexual behavior: A population based study of twin in Sweden. Archives of Sexual Behavior, 39, 75-80.
Laumann, E. O., Gagnon, J. H., Michael, R. T., & Michaels, S. (1994). The social organization of sexuality: Sexual practices in the United States. Chicago: University of Chicago Press.
Lawrence, A., & Zucker, K. J. (2012). Gender identity disorders. In D. C. Biedel & M. Hersen (Eds.), Adult psychopathology and diagnosis (6th ed., pp. 601-636). Hoboken, NJ: John Wiley & Sons.
Lebovitz, P. S. (1972). Feminine behavior in boys: Aspects of its outcome. American Journal of Psychiatry, 128, 1283-1289.
Lemelle, A. J., & Battle, J. (2004). Black masculinity matters in attitudes toward gay males. Journal of Homosexuality, 47, 39-41.
LeVay, S. (1993). The sexual brain. Massachusetts: MIT Press.
LeVay, S. (2011). Gay, straight, and the reason why: The science of sexual orientation. New York: Oxford University Press.
Lever, J. (1994, August 23). Sexual revelations: The 1994 Advocate survey of sexuality and relationships: The mean. The Advocate, 18-24.
Liu, R. T., & Mustanski, B. (2012). Suicidal ideation and self-harm in lesbian, gay, bisexual, and transgender youth. American Journal of Preventative Medicine, 42, 221-228.
Lippa, R. (1998). Gender-related individual differences and the structure of vocational interests: The importance of people-things dimension. Journal of Personality and Social Psychology, 74, 996-1009.
Lippa, R. A. (2005). Gender, nature, and nurture (2nd ed.). Mahwah, NJ: Lawrence Erlbaum Associates.
Lombardi, E. L., Wilchins, R. A., Priesing, D., & Malfouf, D. (2001). Gender violence: Transgender experiences with violence and discrimination. Journal of Homosexuality, 42, 89-101.
Lottes, I. L., & Kuriloff, P. J. (1994). The impact of college experience on political and social attitudes. Sex Roles, 31, 31-54.
Maccoby, E. E. (1998). The two sexes: Growing up apart, coming together. Cambridge, MA: Belknap Press.
MacDonald, A. P. (1983). A little bit of lavender goes a long way: A critique of research on sexual orientation. Journal of Sex Research, 19, 94-100.
MacFarlane, D. F. (1984). Transsexual prostitution in New Zealand: Predominance of persons of Maori extraction. Archives of Sexual Behavior, 13, 301-309.
Maguen, S., & Shipherd, J. C. (2010). Suicide risk among transgender individuals. Psychology & Sexuality, 1, 34-43.
Martin, C. L. (1989). Children’s use of gender-related information in making social judgements. Developmental Psychology, 25, 80-88.
Martin, H. P. (1991). The coming-out process for homosexuals. Hospital and Community Psychiatry, 42, 158-162.
Masi, G., Mucci, M., & Millepiedi, S. (2001). Separation anxiety disorder in children and adolescents. CNS Drugs, 15, 93-104.
Mathijssen, J. J. J. P., Koot, H. M., & Verhulst, F. C. (1999). Predicting change in problem behavior from child and family characteristics and stress in referred children and adolescents. Development and Psychopathology, 11, 305-320.
Mathy, R. M. (2003). Transgender identity and suicidality in a nonclinical sample: Sexual orientation, psychiatric history, and compulsive behaviors. Journal of Psychology & Human Sexuality, 14, 47-65.
Maughan, B., & Rutter, M. (2008). Development and psychopathology: A life course perspective. In M. Rutter, D. V. M. Bishop, D. S. Pine, S. Scott, J. Stenvenson, E. Taylor, & A. Thapar (Eds.), Rutter’s child and adolescent psychiatry (pp. 160-181). Oxford: Blackwell Publishing.
Mays, V. M., & Cochran, S. D. (2001). Mental health correlates of perceived discrimination among lesbian, gay, and bisexual adults in the United States. American Journal of Public Health, 91, 1869-1876.
McDaniel, J. S., Purcell, D. W., & D’Augelli, A. R. (2001). The relationship between sexual orientation and risk for suicide: Research findings and future direction for research and prevention. Suicide and Life-Threatening Behavior, 31(Suppl.), 60-83.
McDonald, G. J. (1982). Individual differences in the coming out process for gay men: implications for theoretical models. Journal of Homosexuality, 8, 47-60.
McLanahan, S., & Sandefur, G. (1994). Growing up with a single parent: What hurts, what helps. Cambridge: Harvard University Press.
McNeil, T. F., & Kaij, L. (1979). Etiological relevance of comparisons of high-risk and low-risk group. Acta Psychiatrica Scandinavica, 59, 545-560.
Menvielle, E. J. (1998). Gender identity disorder [Letter to the Editor]. Journal of the American Academy of Child and Adolescent Psychiatry, 37, 243-244.
Menvielle, E. J. (2012). A comprehensive program for children with gender variant behaviors and gender identity disorders. Journal of Homosexuality, 59, 357-369.
Menvielle, E. J., & Hill, D. B. (2011). An affirmative intervention for families with gender-variant children: A process evaluation. Journal of Gay & Lesbian Mental Health, 15, 94-123.
Menvielle, E. J., & Tuerk, C. (2002). A support group for parents of gender-nonconforming boys. Journal of the American Academy of Child and Adolescent Psychiatry, 41, 1010-1013.
Meyer, I. H. (1995). Minority stress and mental health in gay men. Journal of Health and Social Behavior, 36, 38-56.
Meyer, I. H. (2003). Prejudice, social stress, and mental health in lesbian, gay and bisexual populations: Conceptual issues and research evidence. Psychological Bulletin, 129, 647-697.
Meyer, W. I., Bockting, W. O., Cohen-Kettenis, P., Coleman, E., DiCeglie, D., Devor, H., et al. (2001). The Harry Benjamin International Gender Dysphoria Associations's Standards of Care for Gender Identity Disorders, sixth version. Journal of Psychology and Human Sexuality, 13, 1-30.
Meyer-Bahlburg, H. F. L. (1985). Gender identity disorder of childhood: Introduction. Journal of the American Academy of Child Psychiatry, 24, 681-683.
Meyer-Bahlburg, H. F. L. (2002). Gender identity disorder in young boys: A parent-and peer based treatment protocol. Clinical Child Psychology and Psychiatry, 7, 360-376.
Meyer-Bahlburg, H. F. L. (2010). From mental disorder to iatrogenic hypogonadism: Dilemmas in conceptualizing gender identity variants as psychiatric conditions. Archives of Sexual Behavior, 39, 461-476.
Meyer-Bahlburg, H. F. L., Dolezal, C., Baker, S. W., Ehrhardt, A. A., & New, M. I. (2006). Gender development in women with congenital adrenal hyperplasia as a function of disorder severity. Archives of Sexual Behavior, 35, 667-684.
Meyer-Bahlburg, H. F. L., Dolezal, C., Baker, S. W., & New, M. I. (2008). Sexual orientation in women with classical or non-classical congenital adrenal hyperplasia as a function of degree of prenatal androgen excess. Archives of Sexual Behavior, 37, 85-99.
Michael, R., Gagnon, J., Laumann, E., & Kolata, G. (1994). Sex in America: A definitive survey. Boston: Little, Brown.
Minter, S. (1999). Diagnosis and treatment of gender identity disorder in children. In M. Rottnek (Ed.), Sissies and tomboys. Gender nonconformity and homosexual childhood (pp. 9–33). New York: New York University Press.
Money, J. (1955). Hermaphroditism, gender and precocity in hyperadrenocorticism: Psychologic findings. Bulletin of the Johns Hopkins Hospital, 96, 253-264.
Money, J. (1988). Gay, straight, and in-between: The sexology of erotic orientation. New York: Oxford University Press.
Money, J. (1994). The concept of gender identity disorder in childhood and adolescence after 39 years. Journal of Sex & Marital Therapy, 20, 163-177.
Money, J., & Russo, A. J. (1979). Homosexual outcome of discordant gender identity/role in childhood: Longitudinal follow-up. Journal of Pediatric Psychology, 4, 29-41.
Morrow, D. F. (2004). Social work practice with gay, lesbian, bisexual, and transgender adolescents. Families in Society, 85, 91-99.
Muehlenhard, C. L., & Peterson, Z. D. (2011). Distinguishing between sex and gender: History, current conceptualizations, and implications. Sex Roles, 64, 791-803.
Mukkades, N. M. (2002). Gender identity problems in autistic children. Child: Care, Health & Development, 28, 529-532.
Mustanksi, B. S., Chivers, M. L., & Bailey, J. M. (2002). A critical review of recent biological research on human sexual orientation. Annual Review of Sex Research, 13, 89-140.
Neale, J. M., & Weintraub, S. (1975). Children vulnerable to psychopathology: The Stony Brook High-Risk Project. Journal of Abnormal Child Psychology, 3, 95-113.
Nemoto, T., Bödeker, B., & Iwamoto, M. (2011). Social support, exposure to violence and transphobia, and correlates of depression among male-to-female transgender women with a history of sex work. American Journal of Public Health, 101, 1980-1988.
Newman, B. S., & Muzzonigro, P. G. (1993). The effects of traditional family values on the coming out process of gay male adolescents. Adolescence, 28, 213-226.
Newton-Howes, G., Tryer, P., Anagnostakis, K., Cooper, S., Bowden-Jones, O., Weaver, T., & COSMIC Study Team. (2010). The prevalence of personality disorder, its comorbidity with mental state disorders, and its clinical significance in community mental health teams. Social Psychiatry and Psychiatric Epidemiology, 45, 453-460.
Nordenström, A., Servin, A., Bohlin, G., Larsson, A., & Wedell, A. (2002). Sex-typed toy play behavior correlates with the degree of prenatal androgen exposure assessed by CYP21 genotype in girls with congenital adrenal hyperplasia. The Journal of Clinical Endocrinology and Metabolism, 87, 5119-5124.
Nuttbrock, L., Hwahng, S., Bockting, W., Rosenblum, A., Mason, M., Macri, M., & Becker, J. (2010). Psychiatric impact of gender-related abuse across the life course of male-to-female transgender persons. Journal of Sex Research, 47, 12-23.
Nyberg, K. L., & Alston, J. P. (1976). Analysis of public attitudes towards homosexuality. Journal of Homosexuality, 2, 99-107.
Oswalt, S. B., & Wyatt, T. J. (2011). Sexual orientation and differences in mental health, stress, and academic performance in a national sample of US college students. Journal of Homosexuality, 58, 1255-1280.
Parker, J. G., Rubin, K. H., Price, J. M., & DeRosier, M. E. (1995). Peer relationships, child development and adjustment: A developmental psychopathological perspective. In D. Cicchetti & D. Cohen (Eds.), Developmental psychopathology: Vol 2. Risk, disorder, and adaptation (pp. 96-161). New York: Wiley.
Pasterski, V. L., Geffner, M. E., Brain C., Hindmarsh, P., Brook, C., & Hines, M. (2005). Prenatal hormones and postnatal socialization by parents as determinants of male-typical toy play in girls with congenital adrenal hyperplasia. Child Development, 76, 264-278.
Pasterski, V. L., Geffner, M. E., Brain C., Hindmarsh, P., Brook, C., & Hines, M. (2011). Prenatal hormones and childhood sex segregation: Playmate and play style preferences in girls with congenital adrenal hyperplasia. Hormones and Behavior, 59, 549-555.
Pasterski, V. L., Hindmarsh, P., Geffner, M. E., Brook, C., Brain C., & Hines, M. (2007). Increased aggression and activity level in 3- to 11-year-old girls with congenital adrenal hyperplasia. Hormones and Behavior, 52, 368-374.
Patterson, C. J., Vaden, N. A., Griesler, P. C., & Kupersmidt, J. B. (1991). Income level, gender, ethnicity, and household composition as predictors of children’s peer companionship outside of school. Journal of Applied Developmental Psychology, 12, 447-465.
Paul, J. P. (1993). Childhood cross-gender behavior and adult homosexuality: The resurgence of biological models of sexuality. Journal of Homosexuality, 24, 41-54.
Pickstone-Taylor, S. D. (2003). Children with gender nonconformity [Letter to the Editor]. Journal of the American Academy of Child and Adolescent Psychiatry, 42, 266.
Pillard, R. C., Poumadere, J., & Carretta, R. A. (1981). Is homosexuality familial? A review, some data, and a suggestion. Archives of Sexual Behavior, 10, 465-475.
Pillard, R. C., & Weinrich, J. D. (1986). Evidence of familial nature of male homosexuality. Archives of General Psychiatry, 43, 808-812.
Plöderl, M., & Fartacek, R. (2009). Childhood gender nonconformity and harassment as predictors of suicidality among gay, lesbian, bisexual, and heterosexual Austrians. Archives of Sexual Behavior, 38, 400-410.
Postema, L., Wood, H., Singh, D., Fantus, S., Hyun, J., Leef, J., Bradley, S. J., & Zucker, K. J. (2011). Brief report: Do children with gender identity disorder have intense/ obsessional interests? A preliminary study. Manuscript submitted for publication.
Rekers, G. A., Bentler, P. M., Rosen, A. C., & Lovaas, O. I. (1977). Child gender disturbances: A clinical rationale for intervention. Psychotherapy: Theory, Research and Practice, 14, 2–11.
Rekers, G. A., & Lovaas, I. (1974). Behavioral treatment of deviant sex role behaviors in a male child. Journal of Applied Behavior Analysis, 7, 173-190.
Rekers, G. A., & Yates, C. E. (1976). Sex-typed play in feminoid boys vs. normal boys and girls. Journal of Abnormal Child Psychology, 4, 1-8.
Remafedi, G., French, S., Story, M., Resnick, M. D., & Blum, R. (1998). The relationship between suicide risk and sexual orientation: Results of a population-based study. American Journal of Public Health, 88, 57-60.
Richardson, J. (1996). Setting limits of gender health. Harvard Review of Psychiatry, 4, 49-53.
Richardson, J. (1999). Response: Finding the disorder in gender identity disorder. Harvard Review of Psychiatry, 7, 43-50.
Rieger, G., Chivers, M. L., & Bailey, J. M. (2005). Sexual arousal patterns of bisexual men. Psychological Science, 16, 579-584.
Rieger G., Linsenmeier, J. A., Gygax, L., & Bailey, J. M. (2008). Sexual orientation and childhood gender nonconformity: Evidence from home videos. Developmental Psychology, 44, 46-58.
Rieger G., Linsenmeier, J. A., Gygax, L., Garcia, S., & Bailey, J. M. (2010). Dissecting “gaydar”: accuracy and the role of masculinity-femininity. Archives of Sexual Behavior, 39, 124-140.
Rieger, G., & Savin-Williams, R. (2012). Gender nonconformity, sexual orientation, and psychological well-being. Archives of Sexual Behavior, 41, 611-621.
Robins, L. N. (1966). Deviant children grown up: A sociological and psychiatric study of sociopathic personality. Baltimore: Williams and Wilkins.
Robins, L. N., Cottler, L. B., Bucholz, K. K., & Compton, W. (1995). Diagnostic Interview Schedule, Version 4. St. Louis, MO: Washington University.
Robins, L. N., & Helzer, J. (1985). The Diagnostic Interview Schedule Version III-A. St. Louis, MO: Washington University.
Robins, L. N., Helzer, J. E., Croughan, J., & Ratcliff, K. S. (1981). National Institute of Mental Health Diagnostic Interview Schedule: Its history, characteristics, and validity. Archives of General Psychiatry, 38, 381-389.
Rogers, R. (2001). Handbook of diagnostic and structured interviewing. New York: Guilford Press.
Romano, E., Bell, T., & Billette, J-M. (2011). Prevalence and correlates of multiple victimization in a nation-wide adolescent sample. Child Abuse & Neglect, 35, 468-479.
Rosario, M., Schrimshaw, E. W., & Hunter, J. (2008). Predicting different patterns of sexual identity development overtime among lesbian, gay, and bisexual youths: A cluster analytic approach. American Journal of Community Psychology, 42, 266-282.
Rosario, M., Schrimshaw, E. W., Hunter, J., & Braun, L. (2006). Sexual identity development among lesbian, gay, and bisexual youths: Consistency and change over time. Journal of Sex Research, 43, 46-58.
Rosin, H. (2008, November). A boy’s life. The Atlantic, 302, 56-71.
Ross, M. W.(1983). The married homosexual man: A psychological study. Boston: Routledge & Kegan Paul.
Ruble, D. N., Martin, C. L., & Berenbaum, S. A. (2006). Gender development. In W. Damon & R. M. Lerner (Series eds.) and N. Eisenberg (Vol. ed.), Handbook of child psychology: Vol. 3. Social, emotional, and personality development (6th ed., pp. 858-932). New York: Wiley.
Ryan, C., Huebner, D., Diaz, R. M., & Sanchez, J. (2009). Family rejection as a predictor of negative health outcomes in white and Latino lesbian, gay, and bisexual young adults. Pediatrics, 123, 346-352.
Saeger, K. (2006). Finding our way: Guiding a young transgender child. Journal of GLBT Family Studies, 2, 207-245.
Safren, S. A., & Heimberg, R. G. (1999). Depression, hopelessness, suicidality, and related factors in sexual minority and heterosexual adolescents. Journal of Consulting and Clinical Psychology, 67, 859-866.
Sandfort, T. G. M., Bakker, F., Schellevis, F. G., & Vanwesenbeeck, I. (2006). Sexual orientation and mental and physical health status: Findings from a Dutch population survey. American Journal of Public Health, 96, 1119-1125.
Sattler, J. M. (2001). Assessment of children: Cognitive applications (4th ed.). San Diego: Jerome M. Sattler Publisher, Inc.
Saunders, B. E. (2003). Understanding children exposed to violence: Toward an integration of overlapping ?elds. Journal of Interpersonal Violence, 18, 356-376.
Savin-Williams, R. C. (1998). The disclosure to families of same-sex attractions by lesbian, gay, and bisexual youths. Journal of Research on Adolescence, 8, 49-68.
Savin-Williams, R. C., & Diamond, L. M. (2000). Sexual identity trajectories among sexual-minority youths: Gender comparisons. Archives of Sexual Behavior, 29, 607-627.
Savin-Williams, R. C., & Dube, E. M. (1998). Parental reactions to their child’s disclosure of a gay/lesbian identity. Family Relations, 47, 7-13.
Savin-Williams, R. C., & Ream, G. L. (2003). Suicide attempts among sexual-minority male youth. Journal of Clinical Child and Adolescent Psychology, 32, 509-522.
Schneider, B. H. (2000). Friends and enemies: Peer relations in childhood. London, England: Arnold.
Schwartz, G., Kim, R. M., Kolundzija, A. B., Rieger, G., & Sanders, A. R. (2010). Biodemographic and physical correlates of sexual orientation in men. Archives of Sexual Behavior, 39, 93-109.
Sedgwick, E. K. (1991). How to bring your kids up gay. Social Text, 9, 18-27.
Sell, R. L. (1997). Defining and measuring sexual orientation: A review. Archives of Sexual Behavior, 26, 643-658.
Servin, A., Nordenström, A., Larsson, A., & Bohlin, G. (2003). Prenatal androgens and gender-typed behavior: a study of girls with mild and severe forms of congenital adrenal hyperplasia. Developmental Psychology, 39, 440-450.
Shaffer, N. (2005). Transgender patients: Implications for emergency department policy and practice. Journal of Emergency Nursing, 31, 405-407.
Silverthorn, N. A., & Gekoski, W. L. (1995). Social desirability effects on measures of adjustment to university, independence from parents, and self-efficacy. Journal of Clinical Psychology, 51, 244-251.
Simon, L., Zsolt, U., Fogd, D., & Czobor, P. (2011). Dysfunctional core beliefs, perceived parenting behavior and psychopathology in gender identity disorder: A comparison of male-to-female, female-to-male transsexual and nontranssexual control subjects. Journal of Behavior Therapy and Experimental Psychiatry, 42, 38-45.
Singh, D., Deogracias, J. J., Johnson, L. L., Bradley, S. J., Kibblewhite, S. J., Meyer-Bahlburg, H. F. L., et al. (2010). The gender identity/gender dysphoria questionnaire for adolescents and adults: Further validity evidence. Journal of Sex Research, 47, 49-58.
Singh, D., McMain, S., & Zucker, K. J. (2011). Gender identity and sexual orientation in women with Borderline Personality Disorder. Journal of Sexual Medicine, 8, 447-454.
Smith, Y. L. S., van Goozen, S. H. M., & Cohen-Kettenis, P. T. (2001). Adolescents with gender identity disorder who were accepted or rejected for sex reassignment surgery: A prospective follow-up study. Journal of the American Academy of Child and Adolescent Psychiatry, 40, 472-481.
Smith, Y. L. S., van Goozen, S. H. M., Kuiper, A. J., & Cohen-Kettenis, P. T. (2005). Transsexual subtypes: clinical and theoretical significance. Psychiatry Research, 137, 151-160.
Spiegel, A. (2008, May). Parents consider treatment to delay son’s puberty: New therapy would buy time to resolve gender crisis. NPR, All Things Considered. Retrieved June 13, 2011 from www.npr.org.
Steensma, T. D., Biemond, R., de Boer, F., & Cohen-Kettenis, P. T. (2011). Desisting and persisting gender dysphoria after childhood: A qualitative follow-up study. Clinical Child Psychology and Psychiatry, 16, 499-516.
Steensma, T. D., & Cohen-Kettenis, P. T. (2011). Gender transitioning before puberty? [Letter to the Editor]. Archives of Sexual Behavior, 40, 649-650.
Steensma, T. D., van der Ende, J., Verhulst, F. C., & Cohen-Kettenis, P. T. (2012). Gender variance in childhood and sexual orientation in adulthood: A prospective study. Journal of Sexual Medicine. Advance online publication. doi: 10.1111/j.1743-6109.2012.02701.x
Stein, E. (2012). Commentary on the treatment of gender-variant and gender-dysphoric children and adolescents: Common themes and ethical reflections. Journal of Homosexuality, 59, 480-500.
Stieglitz, K. A. (2010). Development, risk, and resilience of transgender youth. Journal of the Association of Nurses in Aids Care, 21, 192-206.
Stokes, J. P., Damon, W., & McKirnan, D. J. (1997). Predictors of movement towards homosexuality: A longitudinal study of bisexual men. Journal of Sex Research, 34, 304-312.
Stoller, R. J. (1964). The hermaphroditic identity of hermaphrodites. Journal of Nervous and Mental Disease, 139, 453-457.
Storms, M. D. (1980). Theories of sexual orientation. Journal of Personality and Social Psychology, 38, 783-792.
Strahan, R., & Gerbasi, K. C. (1972). Short, homogeneous versions of Marlowe-Crowne Social Desirability Scale. Journal of Clinical Psychology, 28, 191-193.
Szatmari, P., Bryson, S. E., Boyle, M. H., Streiner, D. L., & Duku, E. (2003). Predictors of outcome among high functioning children with autism and Asperger’s Syndrome. Journal of Child Psychology and Psychiatry, 44, 520-528.
Tan, L., & Grace, R. C. (2008). Social desirability and sexual offenders: A review. Sexual Abuse: A Journal of Research and Treatment, 20, 61-87.
Taywaditep, K. J. (2001). Marginalization among the marginalized: Gay men's anti-
effeminacy attitudes. Journal of Homosexuality, 42(1), 1-28.
Toomey, R. B., Ryan, C., Diaz, R. M., Card, N. A., & Russell, S. T. (2010). Gender non-conforming lesbian, gay, bisexual, and transgender youth: School victimization and young adult psychological adjustment. Developmental Psychology, 46, 1580-1589.
van Beijsterveldt, C. E. M., Hudziak, J. J., & Boomsma, D. I. (2006). Genetic and environmental influences on cross-gender behavior and relation to behavior problems: A study of Dutch twins at ages 7 and 10 years. Archives of Sexual Behavior, 35, 647-658.
Vanderburgh, R. (2009). Appropriate therapeutic care for families with pre-pubescent transgender/gender-dissonant children. Child and Adolescent Social Work Journal, 26, 135-154.
VanderLaan, D. P., Gothreau, L. M., Bartlett, N. H., & Vasey, P. L. (2011a). Separation anxiety in feminine boys: Pathological or prosocial? Journal of Gay & Lesbian Mental Health, 15, 30-45.
VanderLaan, D. P., Gothreau, L. M., Bartlett, N. H., & Vasey, P. L. (2011b). Recalled separation anxiety and gender-atypicality in childhood: A study of Canadian heterosexual and homosexual men and women. Archives of Sexual Behavior, 40, 1233-1240.
van Kesteren, P. J. M., Asscheman, H., Megens, J. A. J., & Gooren, L. J. G. (1997). Mortality and morbidity in transsexual subjects treated with cross-sex hormones. Clinical Endocrinology, 47, 337-342.
Vasey, P. L., & Bartlett, N. H. (2007) What can the Samoan “fa’afafine” teach us about the Western concept of gender identity disorder in childhood. Perspectives in Biology and Medicine, 50, 481-490.
Vasey, P. L., VanderLaan, D. P., Gothreau, L. G., & Bartlett, N. H. (2011). Traits of separation anxiety in childhood: A retrospective study in Samoan men, women, and fa’afafine. Archives of Sexual Behavior, 40, 511-517.
Verhulst, F. C. (1995). The epidemiology of child and adolescent psychopathology: Strengths and limitations. In F. C. Verhulst & H. M. Koot (Eds.), The epidemiology of child and adolescent psychopathology (pp. 1-21). New York: Oxford.
Verhulst, F. C., & Koot, H. M. (1991). Longitudinal research in child and adolescent psychiatry. Journal of the American Academy of Child and Adolescent Psychiatry, 30, 361-368.
Verschoor, A. M., & Poortinga, J. (1988). Psychosocial differences between Dutch male and female transsexuals. Archives of Sexual Behavior, 17, 173-178.
Vilain, E. (2000). Genetics of sexual development. Annual Review of Sex Research, 11, 1-25.
Wallien, M. S. C., & Cohen-Kettenis, P. T. (2008). Psychosexual outcome of gender dysphoric children. Journal of the American Academy of Child and Adolescent Psychiatry, 47, 1413-1423.
Wallien, M. S. C., Quilty, L. C., Steensma, T. D., Singh, D., Lambert, S. L., Leroux, A.,…Zucker, K. J. (2009). Cross-national replication of the Gender Identity Interview for Children. Journal of Personality Assessment, 91, 545-552.
Wallien, M. S. C., Swaab, H., & Cohen-Kettenis, P. T. (2007). Psychiatric comorbidity among children with gender identity disorder. Journal of the American Academy of Child and Adolescent Psychiatry, 46, 1307-1314.
Wallien, M. S. C., van Goozen, S. H. M., & Cohen-Kettenis, P. T. (2007). Physiological correlates of anxiety in children with gender identity disorder. European Child & Adolescent Psychiatry, 16, 309-315.
Wallien, M. S. C., Veenstra, R., Kreukels, B. P. C., & Cohen-Kettenis, P. T. (2010). Peer group status of gender dysphoric children: A sociometric study. Archives of Sexual Behavior, 39, 553-560.
Wechsler, D. (1974). Manual: Wechsler Intelligence Scale for Children--Revised. New York: Psychological Corporation.
Wechsler, D. (1981). Wechsler Adult Intelligence Scale--Revised. San Antonio, TX: The Psychological Corporation.
Wechsler, D. (1991). Wechsler Intelligence Scale for Children--Third Edition. San Antonio, TX: The Psychological Corporation.
Wechsler, D. (1997). Wechsler Adult Intelligence Scale--Third Edition. San Antonio, TX: The Psychological Corporation.
Wechsler, D. (2002). Wechsler Preschool and Primary Scale of Intelligence--Third Edition. San Antonio, TX: Psychological Corporation.
Wechsler, D. (2003). Wechsler Intelligence Scale for Children--Fourth Edition. San Antonio, TX: The Psychological Corporation.
Wechsler, D. (2008). Wechsler Adult Intelligence Scale--Fourth Edition. San Antonio, TX: The Psychological Corporation.
Weissman, M. M., Bland, R. C., Canino, G. J., Greenwald, S., Hwu, H. G., Joyce, P. R.,…Yeh, E. K. (1999). Prevalence of suicide ideation and suicide attempts in nine countries. Psychological Medicine, 29, 9-17.
Weitz, C., & Osburg, S. (1996). Transsexualism in Germany: Empirical data on epidemiology and application of the German Transsexuals’ act during its first 10 years. Archives of Sexual Behavior, 25, 409-425.
Welner, Z., Reich, W., Herjanic, B., Jung, K. G., & Amado, H. (1987). Reliability, validity, and parent-child agreement studies of the Diagnostic Interview for Children and Adolescents (DICA). Journal of American Academy of Child Psychiatry, 26, 649-653.
Werry, J. S., & McCellan, J. M. (1992). Predicting outcome in child and adolescent (early onset) schizophrenia and bipolar disorder. Journal of the American Academy of Child and Adolescent Psychiatry, 31, 147-150.
Werry, J. S., McCellan, J. M., & Chard, L. (1991). Childhood and adolescent schizophrenic, bipolar, and schizoaffective disorders: A clinical and outcome study. Journal of the American Academy of Child and Adolescent Psychiatry, 30, 457-465.
Whitam, F. (1977). Childhood indicators of male homosexuality. Archives of Sexual Behaivor, 6, 89-96.
Whitam, F. L., Diamond, M., & Martin, J. (1993). Homosexual orientation in twins: a report on 61 pairs and three triplet sets. Archives of Sexual Behavior, 12, 207-226.
Wilson, I., Griffin, C., & Wren, B. (2002). The validity of the diagnosis of gender identity disorder (child and adolescent criteria). Clinical Child Psychology and Psychiatry, 7, 335-351.
World Health Organization. (1993). The ICD-10 classification of mental and behavioural disorders: clinical descriptions and diagnostic guidelines. Geneva: Author.
Yunger, J. L., Carver, P. R., & Perry, D. G. (2004). Does gender identity influence children’s psychological well-being? Developmental Psychology, 40, 572-582.
Zietsch, B. P., Verweij, K. J., Heath, A. C., Madden, P. A., Martin, N. G., Nelson, E. C., & Lynskey, M. T. (2012). Do shared etiological factors contribute to the relationship between sexual orientation and depression? Psychological Medicine, 42, 521-532.
Zimmerman, M., Rothschild, L., & Chelminski, L. (2005). The prevalence of DSM-IV personality disorders in psychiatric outpatients. American Journal of Psychiatry, 16, 1911-1918.
Zucker, K. J. (1985). Cross-gender identified children. In B. W. Steiner (Ed.), Gender dysphoria: Development, research, and management (pp. 75-174). New York: Plenum Press.
Zucker, K. J. (1992). Gender identity disorder. In S. R. Hooper, G. W. Hynd, & R. E. Mattison (Eds.), Child psychopathology: Diagnostic criteria and clinical assessment (pp. 305-342). Hillsdale, NJ: Erlbaum.
Zucker, K. J. (1994). Gender identity disorder in children. MEDICINE North America, 17, 373-375.
Zucker, K. J. (1999a). Commentary on Richardson’s (1996) “Setting limits on gender health”. Harvard Review of Psychiatry, 7, 37-42.
Zucker, K. J. (1999b). Gender identity disorder in the DSM-IV [Letter to the Editor]. Journal of Sex and Marital Therapy, 25, 5–9.
Zucker, K. J. (2000). Gender identity disorder. In A. J. Sameroff, M. Lewis, & S. M. Miller (Eds.), Handbook of developmental psychopathology (pp. 671-686). New York: Kluwer Academic/Plenum Publishers.
Zucker, K. J. (2001a). Gender identity disorder in children and adolescents. In G. O. Gabbard (Ed.), Treatments of psychiatric disorders (3rd ed., Vol. 2, pp. 2069-2094). Washington, DC: American Psychiatric Press.
Zucker, K. J. (2001b). Biological influences on psychosexual differentiation. In R. K. Unger (Ed.), Handbook of the psychology of women and gender (pp. 101-115). New York: John Wiley & Sons.
Zucker, K. J. (2002). Gender identity disorder. In M. Rutter & E. Taylor (Eds.), Rutter’s child and adolescent psychiatry (pp. 737-753). Oxford: Blackwell Publishing.
Zucker, K. J. (2004a). Gender identity development and issues. Child and Adolescent Psychiatric Clinics of North America, 13, 551-568.
Zucker, K. J. (2004b). Gender identity disorder. In I. B. Weiner (Ed.), Adult psychopathology case studies (pp. 207-228). New York: Wiley.
Zucker, K. J. (2005a). Gender identity disorder in girls. In D. J. Bell, S. L. Foster, & E. J. Mash (Eds.), Handbook of behavioral and emotional problems in girls (pp. 285-319). New York: Kluwer Academic/Plenum Publishers.
Zucker, K. J. (2005b). Measurement of psychosexual differentiation. Archives of Sexual Behavior, 34, 375-388.
Zucker, K. J. (2005c). Gender identity disorder in children and adolescents. Annual Review of Clinical Psychology, 1, 467-492.
Zucker, K. J. (2006a). Gender identity disorder. In D. A. Wolfe & E. J. Mash (Eds.), Behavioral and emotional disorders in adolescents: Nature, assessment, and treatment. (pp. 535-562). New York: Guilford Press.
Zucker, K. J. (2006b). Commentary on Langer and Martin’s (2004) “How dresses can make you mentally ill: Examining gender identity disorder in children.” Child and Adolescent Social Work Journal, 23, 533-555.
Zucker, K. J. (2006c). “I’m a half-boy, half-girl”: Play psychotherapy and parent counselling for gender identity disorder. In R. L. Spitzer, M. B. First, J. B. W. Williams, & M. Gibbons (Eds.), DSM-IV-TR casebook, Vol. 2. Experts tell how they treated their own patients (pp. 321-334). Washington, DC: American Psychiatric Publishing.
Zucker, K. J. (2007). Gender identity disorder in children, adolescents, and adults. In G. Gabbard (Ed.), Gabbard’s treatment of psychiatric disorders (4th ed.) (pp. 683-701). Washington, DC: American Psychiatric Press.
Zucker, K. J. (2008a). Gender identity. In M. L. Wolraich, D. D. Drotar, P. H. Dworkin, & E. C. Perrin (Eds.), Developmental-behavioral pediatrics: Evidence and practice (pp. 825-839). Philadelphia: Mosby/Elsevier.
Zucker, K. J. (2008b). Children with gender identity disorder: Is there a best practice? [Enfants avec troubles de l’identité sexuée: y-a-t-il une pratique la meilleure?]
Neuropsychiatrie de l’Enfance et de l’Adolescence, 56, 358-364.
Zucker, K. J., (2008c). Reflections on the relation between sex-typed behavior in childhood and sexual orientation in adulthood. Journal of Gay & Lesbian Mental Health, 12, 29-59.
Zucker, K. J. (2010a). The DSM diagnostic criteria for gender identity disorder in children. Archives of Sexual Behavior, 39, 477-498.
Zucker, K. J. (2010b). Gender identity and sexual orientation. In M. K. Dulcan (Ed.), Dulcan’s textbook of child and adolescent psychiatry (pp. 543-552). Washington, DC: American Psychiatric Publishing.
Zucker, K. J., Allin, S., Babul-Hirji, R., Bradley, S. J., Chitayat, D., Khoury, A. E., et al. (2003). Assessment of gender identity and gender role behaviour: A comparison of girls with gender identity disorder, girls exposed prenatally to gender-atypical levels of androgens, and control girls [Abstract]. The Endocrinologist, 13, 291.
Zucker, K. J., & Bradley, S. J. (1995). Gender identity disorder and psychosexual problems in children and adolescents. New York: Guilford Press.
Zucker, K. J., & Bradley, S. J. (2004). Gender identity and psychosexual disorders. In J. M. Wiener & M. K. Dulcan (Eds.), Textbook of child and adolescent psychiatry (3rd ed.) (pp. 813-835). Washington, DC: American Psychiatric Publishing.
Zucker, K. J., Bradley, S. J., Ben-Dat, D. N., Ho, C., Johnson, L., & Owen, A. (2003). Psychopathology in the parents of boys with gender identity disorder [Letter to the Editor]. Journal of the American Academy of Child and Adolescent Psychiatry, 42, 2-4.
Zucker, K. J., Bradley, S. J., Kuskis, M., Pecore, K., Birkenfeld-Adams, A., Doering, …Wild, J. (1999). Gender constancy judgments in children with gender identity disorder: Evidence for a developmental lag. Archives of Sexual Behavior, 28, 475-502.
Zucker, K. J., Bradley, S. J., & Lowry Sullivan, C. B. (1996b). Traits of separation anxiety in boys with gender identity disorder. Journal of the American Academy of Child and Adolescent Psychiatry, 35, 791-798.
Zucker, K. J., Bradley, S. J., Lowry Sullivan, C. B., Kuksis, M., Birkenfeld-Adams, A., & Mitchell, J. N. (1993). A gender identity interview for children. Journal of Personality Assessment, 61, 443-456.
Zucker, K. J., Bradley, S. J., Oliver, G., Blake, J., Fleming, S., & Hood, J. (1996a). Psychosexual development of women with congenital adrenal hyperplasia. Hormones and behavior, 30, 300-318.
Zucker, K. J., Bradley, S. J., Owen-Anderson, A., Kibblewhite, S. J., & Cantor, J. M. (2008). Is gender identity disorder in adolescents coming out of the closet? [Letter to the Editor]. Journal of Sex and Marital Therapy, 34, 287-290.
Zucker, K. J., Bradley, S. J., Owen-Anderson, A., Kibblewhite, S. J., Wood, H., Singh, D., & Choi, K. (2012a). Demographics, behavior problems, and psychosexual characteristics of adolescents with gender identity disorder or transvestic fetishism. Journal of Sex and Marital Therapy, 38, 151-189.
Zucker, K. J., Bradley, S. J., Owen-Anderson, A., Singh, D., Blanchard, R., & Bain, J. (2011). Puberty-blocking hormonal therapy for adolescents with gender identity disorder: A descriptive clinical study. Journal of Gay & Lesbian Mental Health, 15, 58-82.
Zucker, K. J., Bradley, S. J., Owen-Anderson, A., & Singh, D. (2010b, April). A parent-report Gender Identity/Gender Role Questionnaire for Adolescents. Poster presented at the Fourth Gender Development Research Conference, San Francisco, CA.
Zucker, K. J., Bradley, S. J., & Sanikhani, M. (1997). Sex differences in referral rates of children with gender identity disorder: Some hypotheses. Journal of Abnormal Child Psychology, 25, 21
Zucker, K. J., Bradley, S. J., Sullivan, C. B., Kuskis, M., Birkenfeld-Adams, & Mitchell, J. N. (1993). A gender identity interview for children. Journal of Personality Assessment, 61, 443-456.
Zucker, K. J., & Cohen-Kettenis, P. T. (2008). Gender identity disorder in children and adolescents. In D. L. Rowland & L. Incrocci (Eds.), Handbook of sexual and gender identity disorders (pp. 376-422). New York: Wiley.
Zucker, K. J., Doering, R. W., Bradley, S. J., & Finegan, J. K. (1982). Sex-typed play in gender-disturbed children: A comparison to sibling and psychiatric controls. Archives of Sexual Behavior, 11, 309-321.
Zucker, K. J., Drummond, K. D., Bradley, S. J., & Peterson-Badali, M. (2009). Troubled mediations on psychosexual differentiations: Regply to Hegarty (2009). Developmental Psychology, 45, 904-908.
Zucker, K. J., Finegan, J. K., Doering, R. W., &. Bradley, S. J. (1983). Human figure drawings of gender-problem children: A comparison to siblings, psychiatric, and normal controls. Journal of Abnormal Child Psychology, 11, 287-298.
Zucker, K. J., & Green, R. (1992). Psychosexual disorders in children and adolescents. Journal of Child Psychology and Psychiatry, 33, 107-151.
Zucker, K. J., & Lawrence, A. A. (2009). Epidemiology of gender identity disorder: Recommendations for the Standards of Care of the World Professional Association for Transgender Health. International Journal of Transgenderism, 11, 8-18.
Zucker, K. J., Lozinski, J. A., Bradley, S. J., & Doering, R. W. (1992). Sex-typed responses in the Rorschach protocols of children with gender identity disorder. Journal of Personality Assessment, 58, 295-310.
Zucker, K. J., Mitchell, J. N., Bradley, S. J., Tkachuk, J., Cantor, J. M., & Allin, S. M. (2006). The Recalled Childhood Gender Identity/Gender Role Questionnaire: Psychometric properties. Sex Roles, 54, 469-483.
Zucker, K. J., Owen, A., Bradley, S. J., & Ameeriar, L. (2002). Gender-dysphoric children and adolescents: A comparative analysis of demographic characteristics and behavior problems. Clinical Child Psychology and Psychiatry, 7, 398-411.
Zucker, K. J., & Seto, M. C. (2008). Gender identity and sexual disorders. In M. Rutter, D. V. M. Bishop, D. S. Pine, S. Scott, J. Stenvenson, E. Taylor, & A. Thapar (Eds.), Rutter’s child and adolescent psychiatry (pp. 864-881). Oxford: Blackwell Publishing.
Zucker, K. J., & Spitzer, R. L. (2005). Was the gender identity disorder of childhood diagnosis introduced into DSM-III as a backdoor maneuver to replace homosexuality? A historical note. Journal of Sex & Marital Therapy, 31, 31-42.
Zucker, K. J., Wilson-Smith, D. N., Kurita, J. A., & Stern, A. (1995). Children’s appraisals of sex-typed behavior in their peers. Sex Roles, 33, 703-725.
Zucker, K. J., Wood, H., Singh, D., & Bradley, S. J. (2012b). A developmental biopsychosocial model for the treatment of children with gender identity disorder. Journal of Homosexuality, 59, 369-397.
Zuger, B. (1978). Effeminate behavior present in boys form childhood: Ten additional years of follow-up. Comprehensive Psychiatry, 19, 363-369.
DSM-IV-TR Diagnostic Criteria for
Gender Identity Disorder
A. A strong and persistent cross-gender identification (not merely a desire for any perceived cultural advantages of being the other sex.
In children, the disturbance is manifested by four (or more) of the following:
1. Repeatedly stated desire to be, or insistence that he or she is, the other sex.
2. In boys, preference for cross-dressing or simulating female attire; in girls, insistence on wearing only stereotypical masculine clothing.
3. Strong and persistent preferences for cross-sex roles in make-believe play or persistent fantasies of being the other sex.
4. Intense desire to participate in the stereotypical games and pastimes of the other sex.
5. Strong preference for playmates of the other sex.
In adolescents and adults, the disturbance is manifested by symptoms such as a stated desire to be the other sex, frequent passing as the other sex, desire to live or be treated as the other sex, or the conviction that he or she has the typical feelings and reactions of the other sex.
B. Persistent discomfort with his or her sex or sense of inappropriateness in the gender role of that sex.
In children, the disturbance is manifested by any of the following:
In boys: assertion that his penis or testes are disgusting or will disappear or assertion that it would be better not to have a penis, or aversion toward rough-and-tumble play and rejection of male stereotypical toys, games, and activities.
In girls: rejection of urinating in a sitting position, assertion that she has or will grow a penis, or assertion that she does not want to grow breasts or menstruate or marked aversion toward normative female clothing.
In adolescents and adults, the disturbance is manifested by symptoms such as preoccupation with getting rid of primary and secondary sex characteristics (e.g., request for hormones, surgery or other procedures to physically alter sexual characteristics to simulate the other sex) or belief that he or she was born the wrong sex.
C. The disturbance is not concurrent with a physical intersex condition.
D. The disturbance causes clinically significant distress or impairment in social, occupational, or other important areas of functioning.
________________________________________________________________
Note. From the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition-Text Revision (p. 581). Copyright 2000 by the American Psychiatric Association.
Appendix B
Proposed DSM-5 Diagnostic Criteria for Gender Dysphoria in Children
Proposed DSM-5 Diagnostic Criteria for Gender Dysphoria (in Children)[65]
________________________________________________________________
A. A marked incongruence between one’s experienced/expressed gender and assigned gender, of at least 6 months duration, as manifested by at least 6 of the following indicators (including A1):
- A strong desire to be of the other gender or an insistence that he or she is the other gender (or some alternative gender different from one's assigned gender)
- In boys, a strong preference for cross-dressing or simulating female attire; in girls, a strong preference for wearing only typical masculine clothing and a strong resistance to the wearing of typical feminine clothing
- A strong preference for cross-gender roles in make-believe or fantasy play
- A strong preference for the toys, games, or activities typical of the other gender
- A strong preference for playmates of the other gender
- In boys, a strong rejection of typically masculine toys, games, and activities and a strong avoidance of rough-and-tumble play; in girls, a strong rejection of typically feminine toys, games, and activities
- A strong dislike of one’s sexual anatomy
- A strong desire for the primary and/or secondary sex characteristics that match one’s experienced gender
B. The condition is associated with clinically significant distress or impairment in social, occupational, or other important areas of functioning, or with a significantly increased risk of suffering, such as distress or disability.
Subtypes
With a disorder of sex development
Without a disorder of sex development
Appendix C
Phone Script
I: Interviewer (Devita Singh)
P: Parent of Potential Participant
I: Hello, may I speak to (name of parent). My name is Devita Singh. I work with Dr. Ken Zucker from the Centre for Addiction and Mental Health. Dr. Zucker last saw you and (name of participant) in (give year). [For those participants last seen before 1997, I will indicate that we used to be called the Clarke Institute of Psychiatry].
P: Hi. How are you?
I: I am fine, thank you. Let me explain why I am calling you. Right now, Dr. Zucker and I are doing a follow-up project on all the boys that have been seen in our clinic over the years and who are now at least 17 years old[66]. We are interested in finding out how children who were seen in the clinic are doing now. Because (name of participant) was a minor when he was first assessed by Dr. Zucker, I wanted to speak with you first about asking (name of participant) if he would be willing to speak with me over the telephone to hear about our project and then deciding if he would like to be a part of it.
P: Can you tell me more about what the study is about?
I: Of course. The purpose of the project is for us to find out how the youngsters we have seen over the years are doing with regard to their gender, sexuality, and overall emotional well-being. We would ask (name of participant) to come to the Centre for about 5 hours, including breaks. During this time, (name of participant) will meet with me. I am a student at the University of Toronto who is working with Dr. Zucker. During our meeting, (name of participant) will be interviewed about his gender identity and sexual development asked to complete some psychological tests and questionnaires. If it is ok with (name of participant), we would also ask you to complete two questionnaires about (name of participant) behavior, which we would mail to you. We will be able to provide some financial compensation for (name of participant’s) participation, including covering costs of transportation.
P: Yes, that is fine with me.
I: Ok. Should I speak with (name of participant) now or would you like to talk with him first and I can call back tomorrow?
Appendix D
Vignette: Parent Report on Gender Identity and Sexual Orientation
Damon was initially assessed in the Gender Identity Service when he was 5 years old.
Damon’s mother, Ms. Salvator, was contacted for follow-up when Damon was 22-years-old. Ms. Salvator indicated that Damon no longer lived with her and agreed to inform Damon that we were interested in conducting a follow-up assessment with him. It was very difficult for Ms. Salvator to contact Damon as he did not have a permanent address or telephone and was living temporarily with various friends. Her only means of contacting was through email. After several months of attempted contact, Damon indicated to his mother that he was not interested in participating in the follow-up study but was comfortable with his mother providing us with information.
Ms. Salvator explained that her and Damon’s life had been chaotic. Damon dropped out of high school when he was 16 years old and moved out of his mother’s home four years thereafter. Ms. Salvator had not seen Damon since he left her home. To the best of Ms. Salvator’s knowledge, Damon never had paid employment. Regarding gender identity and sexual orientation, Ms. Salvator stated that Damon was living as a gay male and was very involved with the gay community. She added that Damon had been open about his sexuality for several years and appeared to be happy with his biological status as male. Ms. Salvator reported that Damon’s twin sibling died of a possible drug-overdose about two years after Damon left high school. Ms. Salvator reported that Damon “never recovered” from his sibling’s death.
Based on the information obtained from Damon’s mother, Damon was classified as a desister with regard to gender identity and as homosexual in sexual orientation.
Appendix E
Participant-Initiated Research Contact
Reasons for Clinical Contact
Participant-Initiated Clinical Contact |
|||
|
Participant ID |
Year of Follow-up |
Age at Follow-up |
Reason for Clinical Contact |
|
1 |
1995 |
18.82 |
Gender dysphoria |
|
2 |
1997 |
15.50 |
Other clinical reasons: depression, school phobia |
|
3 |
1998 |
18.10 |
Other clinical reasons: depression, conflicted about sexual attraction to old men, curiosity about the purpose of the childhood assessment |
|
4 |
2000 |
16.01 |
Sexual orientation |
|
5 |
2000 |
16.63 |
Other clinical reasons: parent-child conflict |
|
6 |
2002 |
20.09 |
Sexual orientation |
|
7 |
2002 |
15.46 |
Other clinical reasons: social problems |
|
8 |
2002 |
13.62 |
Gender dysphoria |
|
9 |
2002 |
16.90 |
Gender dysphoria and sexual orientation |
|
10 |
2003 |
22.53 |
Sexual orientation |
|
11 |
2003 |
23.55 |
Gender dysphoria |
|
12 |
2003 |
16.26 |
Other clinical reasons: alcohol abuse, poor academic performance |
|
13 |
2003 |
17.11 |
Other clinical reasons: depression |
|
14 |
2004 |
27.13 |
Other clinical reasons: substance dependence |
|
15 |
2004 |
18.70 |
Other clinical reasons: depression |
|
16 |
2004 |
20.35 |
Other clinical reasons: depression |
|
17 |
2005 |
17.06 |
Other clinical reasons: behavior problems |
|
18 |
2005 |
18.47 |
Other clinical reasons: behavior problems |
|
19 |
2005 |
16.20 |
Sexual orientation and other clinical reasons: ADHD, learning difficulties |
|
20 |
2006 |
16.97 |
Other clinical reasons: learning disability |
|
21 |
2007 |
13.07 |
Gender dysphoria |
|
22 |
2007 |
15.97 |
Gender dysphoria |
|
|
|
|
|
|
23 |
2008 |
16.84 |
Other clinical reasons: substance abuse, poor academic performance, anxiety |
|
24 |
2008 |
16.61 |
Gender dysphoria |
|
25 |
2009 |
15.53 |
Other clinical reasons: learning disability, anxiety |
|
26 |
2009 |
17.68 |
Gender dysphoria |
|
27 |
2009 |
16.01 |
Other clinical reasons: substance abuse, conduct disorder |
|
28 |
2009 |
17.18 |
Other clinical reasons: medication reassessment |
|
29 |
2010 |
15.41 |
Other clinical reasons: social withdrawal, poor academic performance |
|
30 |
2010 |
14.51 |
Other clinical reasons: alcohol use |
|
31 |
2011 |
15.09 |
Sexual orientation |
|
32 |
2011 |
16.23 |
Sexual orientation |
Appendix F
Research Consent Form
RESEARCH CONSENT FORM
Title of Research Project: Gender Identity and Psychosocial Development
Investigators: Kenneth J. Zucker, Ph.D., Primary Investigator (416-535-8501 x 4040)
Devita Singh, M.A., Co-Investigator (416-535-8501 x 4175)
Devita Singh or Dr. Zucker has explained that the purpose of this study is to gain a better understanding of gender identity development into late adolescence or young adulthood. You will be asked questions about you in an interview and will also complete questionnaires and take some tests. Part of the interview will be about your sexual development and experiences. The interview will be recorded with a tape recorder. Your participation will take place in a quiet room at the Centre for Addiction and Mental Health. The following points have been explained:
- Your participation will include the following: during a single session, you will complete a total of 8 paper-and-pencil questionnaires, 1 interview, and 2 tests. The session will last for approximately 5 hours, including breaks.
- You have the right to refuse to answer any questions.
- Participation in this research is voluntary. You can withdraw your participation at any time, even after beginning an interview or task.
- All of the information collected will remain strictly confidential. Only people associated with the study will see your responses. This consent form will be stored separately from all other information that you have provided. Your responses will not be associated with your name; instead, your name will be converted to a code number on all questionnaires and forms.
- Your privacy will be protected in any scientific presentation or publication resulting from this study. The audio recording of your interview will only be used to record your responses. The tapes will then be destroyed.
- You will receive $___ for compensation of your time.
- With your consent, we will also contact your parent or guardian to complete a questionnaire about your development.
- Information that you provide about yourself will be kept confidential and stored using a code number that does not include your name. The audiotape of your interview will be stored in a locked filing cabinet. The audiotapes will be retained for 5 years after the completion of any scientific publications that result from this study, and at that time, they will be destroyed.
- The investigator will answer any questions about the research now or during the course of the study. If you have any other questions or concerns, you can address them to the primary investigator, Dr. Kenneth Zucker (416-535-8501, extension 4040) or the co-investigator, Devita Singh (416-535-8501 x 4175). You will be given a copy of this consent form for your records.
- Dr. Padraig Darby, Chair, Research Ethics Board, Centre for Addiction and Mental Health, may be contacted by research subjects to discuss their rights. Dr. Darby may be reached by telephone at 416-535-8501, extension 6876.
- As part of continuing review of the research, your study records may be assessed on behalf of the Research Ethics Board and, if applicable, by the Health Canada Therapeutic Products Programme. A person from the research ethics team may contact you (if your contact information is available) to ask you questions about the research study and your consent to participate. The person assessing your file or contacting you must maintain your confidentiality to the extent permitted by law.
I consent to participate in this study and I consent to allow my parents or guardian to complete a questionnaire about me.
____________________________
Name of Participant (Please Print)
____________________________ _____________________
Signature of Participant Date
____________________________
Name of Person Obtaining Consent (Please Print)
____________________________ _____________________
Signature of Person Obtaining Consent Date
Appendix G
Semi-Structured Interview to Assess Gender Identity Disorder in Biological Males
Semi-Structured Interview for Gender Identity Disorder
Timeframe: Past 12 months
Point A Criteria
- In the past 12 months, have you felt like you wanted to be a woman?
____ YES ____SOMETIMES ____NO
If YES or SOMETIMES, Ask:
- How often do you have these feelings of wanting to be a woman?
- Describe what it is that makes you feel this way.
- Are there situations where you find these feelings stronger or more intense?
If YES, ask to elaborate.
- Are there times in the past 12 months when you have felt confused as to whether you wanted to be a man or a woman?
If YES, ask to elaborate.
- Have you ever told anyone that you wanted to be a woman?
____ YES ____SOMETIMES ____NO
- Do you frequently pass as the other sex?
____ YES ____SOMETIMES ____NO
If YES or SOMETIMES, ASK:
a. In what type of situations do you present yourself as a woman? (social situations, internet, etc)
b. How? (e.g., clothing)
c. How often do you present yourself as a woman?
- Do you have the desire to live and/or be treated as the opposite sex?
____ YES ____SOMETIMES ____NO
- Do you believe that you have the typical feelings and reactions of the opposite sex?
____ YES ____SOMETIMES ____NO
Point B Criteria
- Would you like to receive sex hormones to feminize your physical appearance (e.g., to grow breasts; to not have body hair)?
____ YES ____SOMETIMES ____NO
- Would you like to have surgery to create a vagina?
____ YES ____SOMETIMES ____NO
- Would you like to get rid of male sex characteristics, such as your penis or testes?
____ YES ____SOMETIMES ____NO
IF YES or SOMETIMES to 1, 2, or 3 above, Ask:
Have you seen a doctor to request hormones or surgery?
If YES, ask to elaborate.
- Do you believe that you should have been born a female?
____ YES ____SOMETIMES ____NO
Distress Criteria
1. Do these feelings about your gender cause you significant stress in social life? If YES, how?
2. Do these feelings about your gender identity cause you significant stress in your occupational life (e.g., job, school, etc.)? If YES, how?
Appendix H
Inter-rater Reliability for Kinsey Ratings of Sexual Fantasy and Sexual Behavior
|
|
|
|
Kappa Statistics For Kinsey Sexual Fantasy Ratings |
|
|
Variable |
Kappa |
|
Crush |
1.00 |
|
Visual |
0.94 |
|
Dreams |
1.00 |
|
Masturbation |
0.81 |
|
Global Fantasy Rating |
0.95 |
|
|
|
|
Kappa Statistics For Kinsey Sexual Behavior Ratings |
|
|
Variable |
Kappa |
|
Dating |
1.00 |
|
Holding hands |
0.91 |
|
Kissing |
1.00 |
|
Genital/breast contact |
1.00 |
|
Intercourse |
1.00 |
|
Global Behavior Rating |
1.00 |
Appendix I
Suicidality Questionnaire
Suicidality Questionnaire
These questions ask about feelings or behaviors about hurting yourself.
The next six questions will be about any feelings or thoughts you have had since the age of 13.
- Since the age of 13, have you ever seriously considered attempting suicide?
- Never
- Rarely
- Sometimes
- Often
- Did you make a plan about how you would attempt suicide?
- Yes
- No
- Since the age of 13, how many times did you actually attempt suicide?
- 0 times
- 1 time
- 2 or 3 times
- 4 or 5 times
- 6 or more times
- If you have attempted suicide in the past, did your attempt result in an injury, poisoning, or overdose that had to be treated by a doctor or nurse?
- I did not attempt suicide in the past
- Yes
- No
- If you attempted suicide since you were 13, how did you feel at the time you tried to attempt suicide?
- I knew I was not going to die.
- I really wanted to die.
- Have your feelings about suicide been related to your unhappiness about being a male.
- Very much related
- Somewhat related
- A little related
- Not at all related
The next questions are similar but will be about your feelings and thoughts within the past 12 months.
- During the past 12 months, did you ever seriously consider attempting suicide?
- Never
- Rarely
- Sometimes
- Often
- During the past 12 months, did you make a plan about how you would attempt suicide?
- Yes
- No
- During the past 12 months, how many times did you actually attempt suicide?
- 0 times
- 1 time
- 2 or 3 times
- 4 or 5 times
- 6 or more times
- If you attempted suicide during the past 12 months, did your attempt result in an injury, poisoning, or overdose that had to be treated by a doctor or nurse?
- I did not attempt suicide in the past 12 months
- Yes
- No
- If you attempted suicide in the past 12 months, how did you feel at the time you tried to attempt suicide.
- I knew I was not going to die.
- I really wanted to die.
- How do you feel now?
- I am glad to be alive.
- I wish I had been successful.
- Have your feelings about suicide been related to your unhappiness about being a male?
- Very much related
- Somewhat related
- A little related
- Not at all related
Appendix J
Victimization Survey
Victimization Survey
Since the age of 13, how often have these things happened to you because of your gender identity?
|
|
Never |
Once |
Twice |
3 or more |
If more than 3, how many? |
|
a. Verbal insults |
0 |
1 |
2 |
3 |
______ |
|
b. Someone threatened to tell others about your gender identity
|
0 |
1 |
2 |
3 |
______ |
|
c. Threats of physical violence |
0 |
1 |
2 |
3 |
______ |
|
d. Objects thrown at you |
0 |
1 |
2 |
3 |
______ |
|
e. Punched, kicked or beaten |
0 |
1 |
2 |
3 |
______ |
|
f. Threatened with a knife, gun, or another weapon |
0 |
1 |
2 |
3 |
______
|
|
g. Sexually attacked |
0 |
1 |
2 |
3 |
______ |
In the past 12 months, how often have these things happened to you because of your gender identity?
|
|
Never |
Once |
Twice |
3 or more |
If more than 3, how many? |
|
a. Verbal insults |
0 |
1 |
2 |
3 |
______ |
|
b. Someone threatened to tell others about your gender identity
|
0 |
1 |
2 |
3 |
______ |
|
c. Threats of physical violence |
0 |
1 |
2 |
3 |
______ |
|
d. Objects thrown at you |
0 |
1 |
2 |
3 |
______ |
|
e. Punched, kicked or beaten |
0 |
1 |
2 |
3 |
______ |
|
f. Threatened with a knife, gun, or another weapon |
0 |
1 |
2 |
3 |
______
|
|
g. Sexually attacked |
0 |
1 |
2 |
3 |
______ |
If you scored Never for verbal insults OR threats to tell others about your gender identity on the first page, skip this page and continue on page 3 (the next page).
Of all the times you were verbally insulted, where did these incidents occur (check off the applicable locations)?
£ Home £ Social settings (e.g., bars, parks, etc.)
£ High school £ College Campus
£ Neighbourhood £ Work place
£ Other: __________________
Of all the times you were ever verbally insulted, how many incidents were done by:
|
Relationship (Check if YES, did it) |
How many times? |
|
Relationship (Check if YES, did it) |
How many times? |
|
£ Mother |
_______ |
|
£ Male strangers |
_______ |
|
£ Father |
_______ |
|
£ Female strangers |
_______ |
|
£ Stepmother |
_______ |
|
£ Teachers |
_______ |
|
£ Stepfather |
_______ |
|
£ Physical education teachers |
_______ |
|
£ Your mother’s girlfriend or boyfriend
|
_______ |
|
£ Boyfriends |
_______ |
|
£ Your father’s girlfriend or boyfriend |
_______ |
|
£ Girlfriends |
_______ |
|
£ Your brother(s) |
_______ |
|
£ Houseparents (in group home) |
_______ |
|
£ Your sister(s) |
_______ |
|
£ Fosterparents |
_______ |
|
£ Other members of the family
|
_______ |
|
£ Counselors |
_______ |
|
£ Male peer who was neither a friend nor a stranger |
_______ |
|
£ Other people: ____________________________ |
_______ |
|
£ Female peer who neither a friend nor a stranger |
_______ |
|
£ Other people: __________________________
|
_______ |
|
£ Male friends |
_______ |
|
£ Female friends |
_______ |
If you scored Never for any physical violence (e.g., physical threats, objects thrown, punched, kicked, or beaten, and threats with weapons) on the first page, skip this page and continue on page 4 (the next page).
Of all the times you were threatened with physical violence, where did these incidents occur (check off the applicable locations)?
£ Home £ Social settings (e.g., bars, parks, etc.)
£ High school £ College Campus
£ Neighbourhood £ Work place
£ Other: __________________
Of all the times you were every threatened with physical violence, how many incidents were done by:
|
Relationship (Check if YES, did it) |
How many times? |
|
Relationship (Check if YES, did it) |
How many times? |
|
£ Mother |
_______ |
|
£ Male strangers |
_______ |
|
£ Father |
_______ |
|
£ Female strangers |
_______ |
|
£ Stepmother |
_______ |
|
£ Teachers |
_______ |
|
£ Stepfather |
_______ |
|
£ Physical education teachers |
_______ |
|
£ Your mother’s girlfriend or boyfriend
|
_______ |
|
£ Boyfriends |
_______ |
|
£ Your father’s girlfriend or boyfriend |
_______ |
|
£ Girlfriends |
_______ |
|
£ Your brother(s) |
_______ |
|
£ Houseparents (in group home) |
_______ |
|
£ Your sister(s) |
_______ |
|
£ Fosterparents |
_______ |
|
£ Other members of the family
|
_______ |
|
£ Counselors |
_______ |
|
£ Male peer who was neither a friend nor a stranger |
_______ |
|
£ Other people: ____________________________ |
_______ |
|
£ Female peer who neither a friend nor a stranger |
_______ |
|
£ Other people: __________________________
|
_______ |
|
£ Male friends |
_______ |
|
£ Female friends |
_______ |
If you scored Never for sexual attacks on the first page, skip this page and continue on page 5 (the next page).
Of all the times you were attacked sexually, where did these incidents occur (check off the applicable locations)?
£ Home £ Social settings (e.g., bars, parks, etc.)
£ High school £ College Campus
£ Neighbourhood £ Work place
£ Other: __________________
Of all the times you were ever attacked sexually, how many incidents were done by?
|
Relationship (Check if YES, did it) |
How many times? |
|
Relationship (Check if YES, did it) |
How many times? |
|
£ Mother |
_______ |
|
£ Male strangers |
_______ |
|
£ Father |
_______ |
|
£ Female strangers |
_______ |
|
£ Stepmother |
_______ |
|
£ Teachers |
_______ |
|
£ Stepfather |
_______ |
|
£ Physical education teachers |
_______ |
|
£ Your mother’s girlfriend or boyfriend
|
_______ |
|
£ Boyfriends |
_______ |
|
£ Your father’s girlfriend or boyfriend |
_______ |
|
£ Girlfriends |
_______ |
|
£ Your brother(s) |
_______ |
|
£ Houseparents (in group home) |
_______ |
|
£ Your sister(s) |
_______ |
|
£ Fosterparents |
_______ |
|
£ Other members of the family
|
_______ |
|
£ Counselors |
_______ |
|
£ Male peer who was neither a friend nor a stranger |
_______ |
|
£ Other people: ____________________________ |
_______ |
|
£ Female peer who neither a friend nor a stranger |
_______ |
|
£ Other people: __________________________
|
_______ |
|
£ Male friends |
_______ |
|
£ Female friends |
_______ |
If you have been the target of harassment, threats, or violence because of your gender identity have you always reported it to an appropriate official (e.g., teacher, police, job supervisor)?
- Not applicable
- No, I never reported any incidents.
- No, but I have reported some. How many? __________
- Yes, I reported all incidents. How many? ____________
Have you changed the way you act in any way because of fears of being harassed or attacked because of your gender identity (e.g., avoid certain locations or social groups)?
- No
- Yes
How have you changed your behavior? Please write below.
_______________________________________________________________
_______________________________________________________________
_______________________________________________________________
_______________________________________________________________
Thinking back on any of these incidents, how upset do you get when you think about it now?
- Not at all
- Some
- A lot
How have the incidents affected the way you saw your future?
- Made no difference
- Made me worry about the future
- Made me wonder if life was worth living
Appendix K
Gender Identity and Sexual Orientation at Follow-up
|
Gender Identity and Sexual Orientation at Follow-up |
|
||||||
|
No. |
FU Date(s)a |
Age at Assessment (in years) |
Age at follow-up (in years) |
Kinsey Ratings |
DSM |
||
|
Fantasy |
Behavior |
||||||
|
|
|
|
|
|
|
|
|
|
1 |
1987-11-16 |
6.42 |
18.24 |
6 |
6 |
+ |
|
|
2 |
1986-01-03 |
5.69 |
15.05 |
0 |
0 |
+ |
|
|
3 |
1987-10-23 |
8.23 |
17.73 |
0 |
0 |
- |
|
|
4 |
1986-01-28 a 1990-03-14 2011-01-28 |
6.39 |
15.15 18.27 39.15 |
6 |
6 |
+ |
|
|
5 |
1986-07-08 a 1987-07-27 |
5.87 |
14.06 15.11 |
0 |
7 |
+ |
|
|
6 |
1987-02-04 a 1989-03-13 |
5.42 |
14.15 16.26 |
7 |
7 |
+ |
|
|
7 |
1986-08-05 |
9.53 |
17.65 |
0 |
7 |
- |
|
|
8 |
1987-07-03 a 1988-12-03 |
5.07 |
13.96 15.39 |
0 |
7 |
+ |
|
|
9 |
1986-12-19 |
7.95 |
16.10 |
0 |
0 |
- |
|
|
10 |
1986-03-25 |
12.85 |
20.14 |
5 |
6 |
- |
|
|
11 |
1987-11-16 a 1990-07-15 1993-12-15 |
5.33 |
14.15 16.80 20.23 |
5 |
7 |
+ |
|
|
12 |
1986-02-11 a 1987-02-11 1989-04-27 |
8.79 |
15.82 16.82 19.04 |
3 |
7 |
+ |
|
|
13 |
1987-04-22 |
6.19 |
14.22 |
7 |
7 |
+ |
|
|
14 |
1989-03-16 a 1988-12-29 |
4.69 |
14.46 14.25 |
0 |
7 |
- |
|
|
No. |
FU Date(s)a |
Age at Assessment (in years) |
Age at follow-up (in years) |
Kinsey Ratings |
DSM |
|
|
Fantasy |
Behavior |
|||||
|
15 |
1986-06-24 |
10.38 |
17.32 |
0 |
0 |
- |
|
16 |
1983-11-02 a 1986-11-30 |
7.00 |
11.14 14.21 |
0 |
0 |
+ |
|
17 |
1987-03-19 |
7.19 |
14.68 |
0 |
0 |
+ |
|
18 |
1986-07-21 |
12.37 |
18.84 |
1 |
0 |
- |
|
19 |
1986-04-15 a 1988-11-07 |
10.70 |
17.09 19.38 |
6 |
6 |
- |
|
20 |
1988-02-02 |
6.46 |
14.34 |
0 |
0 |
+ |
|
21 |
1988-10-12 a 1992-02-15 2010-08-09 |
5.85 |
13.31 17.65 35.14 |
6 |
6 |
+ |
|
22 |
1991-12-19 |
5.14 |
15.83 |
0 |
7 |
+ |
|
23 |
1986-12-23 a 1988-07-27 1993-11-16 |
11.13 |
16.88 18.28 23.59 |
6 |
6 |
- |
|
24 |
1986-12-22 a 1990-01-11 |
10.49 |
16.03 19.08 |
6 |
6 |
- |
|
25 |
1993-04-01 |
5.34 |
20.00 |
6 |
6 |
+ |
|
26 |
1988-08-04 |
8.58 |
15.32 |
0 |
7 |
+ |
|
27 |
1987-08-06 |
11.07 |
16.74 |
3 |
4 |
+ |
|
28 |
1988-11-24 |
8.46 |
14.76 |
0 |
7 |
+ |
|
29 |
1991-12-02 |
5.61 |
14.96 |
0 |
7 |
- |
|
30 |
1990-01-21 |
9.14 |
16.53 |
0 |
7 |
- |
|
31 |
1992-03-23 a 1998-10-15 |
3.75 |
13.09 19.65 |
5 |
3 |
+ |
|
No. |
FU Date(s)a |
Age at Assessment (in years) |
Age at follow-up (in years) |
Kinsey Ratings |
DSM |
|
|
Fantasy |
Behavior |
|||||
|
32 |
1987-11-09 |
9.31 |
14.06 |
2 |
7 |
+ |
|
33 |
1986-02-04 |
12.29 |
15.06 |
3 |
7 |
- |
|
34 |
2002-06-07 |
7.18 |
26.04 |
6 |
6 |
- |
|
35 |
1990-10-15 |
11.01 |
17.95 |
0 |
7 |
- |
|
36 |
1988-03-11 |
10.23 |
14.53 |
0 |
7 |
- |
|
37 |
1990-07-26 |
8.58 |
15.01 |
0 |
0 |
+ |
|
38 |
2004-06-06 |
6.90 |
27.13 |
6 |
6 |
+ |
|
39 |
1988-03-07 |
10.71 |
14.63 |
5 |
7 |
- |
|
40 |
1991-11-16 |
8.99 |
15.47 |
5 |
6 |
+ |
|
41 |
2009-02-23 |
3.77 |
27.51 |
5 |
5 |
+ |
|
42 |
1988-06-12 |
11.99 |
14.82 |
7 |
7 |
- |
|
43 |
1991-12-20 |
9.68 |
16.03 |
0 |
0 |
- |
|
44 |
2009-09-11 |
6.35 |
29.60 |
6 |
7 |
+ |
|
45 |
2003-08-20 |
5.59 |
22.53 |
6 |
6 |
+ |
|
46 |
2009-10-24 |
7.29 |
30.31 |
6 |
6 |
+ |
|
47 |
2009-07-29 |
4.72 |
27.29 |
6 |
6 |
+ |
|
48 |
1998-06-22 |
6.75 |
18.10 |
6 |
6 |
+ |
|
49 |
2003-06-04 |
8.22 |
23.55 |
6 |
6 |
+ |
|
50 |
2000-05-11 |
3.52 |
16.01 |
6 |
6 |
+ |
|
51 |
2002-07-03 |
5.91 |
20.09 |
4 |
6 |
+ |
52 |
2010-03-31 |
4.04 |
26.03 |
6 |
7 |
+ |
|
53 |
2010-01-22 |
6.94 |
28.70 |
5 |
6 |
+ |
No. |
FU Date(s)a |
Age at Assessment (in years) |
Age at follow-up (in years) |
Kinsey Ratings |
DSM |
|
|
Fantasy |
Behavior |
|||||
|
54 |
2010-01-25 |
4.96 |
26.67 |
6 |
6 |
- |
|
55 |
2010-01-23 |
5.09 |
26.59 |
6 |
6 |
+ |
|
56 |
2010-09-20 |
4.15 |
26.08 |
1 |
0 |
+ |
|
57 |
2009-12-15 |
5.22 |
26.12 |
5 |
6 |
+ |
58 |
2010-04-28 |
6.33 |
26.26 |
6 |
6 |
+ |
|
59 |
2010-01-30 |
3.95 |
23.60 |
5 |
6 |
+ |
|
60 |
2010-02-08 |
6.73 |
26.08 |
6 |
6 |
+ |
|
61 |
2003-04-17 |
3.85 |
16.26 |
0 |
– |
+ |
|
62 |
2004-08-26 |
5.13 |
18.70 |
6 |
6 |
+ |
|
63 |
2010-05-26 |
5.25 |
24.24 |
6 |
6 |
+ |
|
64 |
2010-05-19 |
4.67 |
23.50 |
3 |
4 |
- |
|
65 |
1999-03-25 a 2004-12-30 |
7.13 |
14.58 20.35 |
6 |
6 |
+ |
|
66 |
2010-03-01 |
9.03 |
27.35 |
6 |
6 |
- |
|
67 |
2002-08-29 |
5.19 |
16.29 |
6 |
1 |
+ |
|
68 |
2010-11-19 |
4.16 |
22.93 |
5 |
4 |
+ |
|
69 |
2000-08-31 |
8.11 |
16.63 |
2 |
7 |
- |
|
70 |
2011-03-06 |
4.41 |
23.38 |
0 |
0 |
+ |
|
71 |
2009-08-18 |
4.32 |
21.65 |
6 |
6 |
+ |
|
72 |
2010-12-20 |
3.57 |
22.16 |
0 |
0 |
- |
|
73 |
2003-10-08 |
6.58 |
17.11 |
6 |
6 |
- |
No. |
FU Date(s)a |
Age at Assessment (in years) |
Age at follow-up (in years) |
Kinsey Ratings |
DSM |
|
|
Fantasy |
Behavior |
|||||
|
74 |
2009-03-23 |
6.95 |
22.87 |
6 |
6 |
+ |
|
75 |
2006-06-02 |
3.98 |
16.97 |
0 |
0 |
+ |
|
76 |
2009-01-31 |
6.82 |
21.98 |
5 |
6 |
+ |
77 |
2005-05-12 |
6.02 |
17.06 |
0 |
0 |
+ |
|
78 |
1997-04-10 |
12.67 |
15.50 |
7 |
7 |
- |
|
79 |
2008-03-19 |
4.06 |
16.84 |
6 |
6 |
+ |
|
80 |
2009-11-23 |
7.45 |
22.32 |
2 |
0 |
+ |
|
81 |
2005-07-18 a 2002-01-08 2001-05-30 |
9.46 |
18.47 14.94 14.35 |
0 |
0 |
- |
|
82 |
2002-08-30 |
9.47 |
15.46 |
0 |
0 |
- |
|
83 |
2009-07-04 |
10.30 |
20.27 |
6 |
6 |
+ |
|
84 |
2002-08-28 |
8.87 |
13.62 |
6 |
6 |
+ |
|
85 |
2009-03-21 |
5.83 |
17.14 |
3 |
3 |
+ |
|
86 |
2009-02-08 |
4.31 |
15.53 |
5 |
7 |
+ |
|
87 |
2009-08-27 |
9.27 |
20.75 |
0 |
0 |
- |
|
88 |
2009-06-13 |
7.62 |
19.77 |
6 |
6 |
+ |
|
89 |
2009-03-08 |
8.19 |
19.05 |
5 |
0 |
- |
|
90 |
2009-11-22 |
8.66 |
20.05 |
3 |
0 |
+ |
|
91 |
2002-07-29 |
12.82 |
16.90 |
0 |
7 |
- |
|
92 |
2009-10-02 |
9.07 |
20.25 |
0 |
0 |
- |
|
93 |
2011-02-06 |
5.35 |
17.43 |
6 |
6 |
+ |
|
No. |
FU Date(s)a |
Age at Assessment (in years) |
Age at follow-up (in years) |
Kinsey Ratings |
DSM |
|||
|
Fantasy |
Behavior |
|||||||
|
94 |
2005-09-01 |
9.46 |
16.20 |
– |
– |
+ |
||
|
95 |
2010-12-15 |
10.35 |
22.18 |
6 |
6 |
+ |
||
|
96 |
2010-08-16 |
4.39 |
15.41 |
0 |
0 |
+ |
||
|
97 |
2011-02-09 |
3.69 |
15.09 |
4 |
0 |
+ |
||
|
98 |
2009-02-25 |
10.0 |
19.19 |
0 |
0 |
+ |
||
|
99 |
2010-07-19 |
4.53 |
14.51 |
0 |
7 |
+ |
||
|
100 |
2009-04-08 |
9.13 |
17.68 |
6 |
6 |
+ |
||
|
101 |
2011-03-02 |
6.39 |
16.23 |
1 |
0 |
+ |
||
|
102 |
2009-09-25 |
12.48 |
20.42 |
3 |
3 |
- |
||
|
103 |
2009-09-12 |
8.84 |
16.01 |
3 |
3 |
+ |
||
|
104 |
2008-04-16 |
10.76 |
16.61 |
6 |
6 |
+ |
||
|
105 |
2009-12-18 |
12.99 |
20.22 |
0 |
7 |
- |
||
|
106 |
2007-04-26 |
8.51 |
13.07 |
0 |
0 |
+ |
||
|
107 |
2010-07-10 |
11.53 |
18.96 |
5 |
6 |
+ |
||
|
108 |
2007-04-27 a 2007-09-26 |
11.60 |
15.55 15.97 |
6 |
7 |
- |
||
|
109 |
2009-10-30 |
9.68 |
15.69 |
6 |
6 |
+ |
||
|
110 |
2009-11-21 |
12.84 |
17.18 |
0 |
0 |
- |
||
|
Parent Report
|
|
|||||||
|
111 |
2010-11-09 |
3.75 |
31.28 |
– |
– |
+ |
||
|
112 |
1995-05-08 |
8.36 |
18.82 |
(6) |
– |
+ |
||
|
No. |
FU Date(s)a |
Age at Assessment (in years) |
Age at follow-up (in years) |
Kinsey Ratings |
DSM |
|
|
Fantasy |
Behavior |
|||||
|
113 |
2009-09-09 |
8.69 |
33.34 |
(6) |
– |
- |
|
114 |
2009-06-29 |
5.48 |
28.73 |
(6) |
– |
- |
|
115 |
2009-08-10 |
4.63 |
27.73 |
– |
– |
+ |
|
116 |
1995-12-15 |
7.30 |
16.67 |
(6) |
– |
- |
|
117 |
2009-10-09 |
5.39 |
27.75 |
(6) |
– |
- |
|
118 |
2010-08-19 |
5.88 |
28.11 |
(6) |
– |
- |
119 |
2009-11-20 |
9.27 |
31.40 |
(6) |
– |
- |
|
120 |
2009-08-10 |
7.82 |
29.57 |
(0) |
– |
- |
|
121 |
2009-09-20 |
6.93 |
28.69 |
– |
– |
- |
|
122 |
2009-11-17 |
3.33 |
24.77 |
(6) |
– |
+ |
|
123 |
2009-11-19 |
4.65 |
24.77 |
(0) |
– |
+ |
|
124 |
2010-01-11 |
6.16 |
25.60 |
(0) |
– |
+ |
|
125 |
2009-12-14 |
6.35 |
25.23 |
– |
– |
- |
|
126 |
2009-09-21 |
5.28 |
23.65 |
(6) |
– |
+ |
|
127 |
2010-01-31 |
4.73 |
23.50 |
(0) |
– |
+ |
|
128 |
2001-11-15 |
11.14 |
21.58 |
(6) |
– |
- |
|
129 |
2010-02-11 |
3.84 |
22.47 |
(6) |
– |
+ |
|
130 |
2003-06-15 |
11.24 |
23.16 |
(6) |
– |
- |
|
131 |
2011-04-07 |
4.60 |
24.18 |
(6) |
– |
+ |
|
132 |
2010-03-10 |
10.21 |
28.15 |
– |
– |
- |
|
133 |
2002-12-19 |
5.55 |
18.10 |
(6) |
– |
+ |
|
134 |
2009-02-04 |
10.18 |
21.55 |
(6) |
– |
+ |
|
No. |
FU Date(s)a |
Age at Assessment (in years) |
Age at follow-up (in years) |
Kinsey Ratings |
DSM |
||
|
Fantasy |
Behavior |
||||||
|
135 |
2009-03-09 |
12.06 |
23.98 |
(6) |
– |
+ |
|
|
136 |
2010-01-07 |
6.76 |
19.50 |
– |
– |
+ |
|
|
137 |
2009-06-08 |
11.91 |
23.29 |
|
– |
- |
|
|
138 |
2009-03-11 |
8.79 |
18.19 |
– |
– |
+ |
|
|
139 |
2009-02-02 |
11.90 |
21.17 |
(6) |
– |
- |
|
|
Note. For Kinsey ratings (last 12 months), 0 = exclusively heterosexual in relation to birth sex and 6 = exclusively homosexual in relation to birth sex. A dash in the Kinsey columns indicate that data were not available. A bracketed score in the Kinsey Fantasy column indicates that the participant did not complete a full sexual orientation interview but sufficient data were available to inform a Kinsey rating. In the DSM column, a plus sign indicates the participant meet full DSM-III, DSM-III-R, or DSM-IV criteria for GID at the childhood assessment. A minus sign indicates the participant was subthreshold for the diagnosis of GID. aSome participants were assessed at more than one follow-up points. In these cases, data from the most recent assessment were used. |
|
||||||
Appendix L
Diagnostic Interview for Children and Adolescents or Diagnostic Interview Schedule
Diagnoses at Follow-up
|
Diagnostic Interview for Children and Adolescents Diagnoses at Follow-up
|
|||
|
ID |
Diagnosis(es) |
No. of Diagnoses |
Clinical Comments |
|
1 |
None |
0
|
|
|
2 |
None |
0
|
|
|
3 |
Adjustment Disorder with Depressed Mood |
1
|
|
|
4 |
None |
0
|
|
|
5 |
None |
0
|
|
|
6 |
None |
0
|
|
|
7 |
None |
0
|
|
|
8 |
None |
0
|
|
|
9 |
Conduct, Non-Aggressive Alcohol Abuse
|
2
|
|
|
10 |
None
|
0 |
|
|
11 |
None
|
0 |
|
|
12 |
None
|
0 |
|
|
13 |
None
|
0 |
|
|
14 |
None
|
0 |
|
|
15 |
None
|
0 |
|
|
16 |
Adjustment Disorder with Depressed mood
|
1 |
|
|
17 |
Conduct,
Non-aggressive |
2 |
|
|
18 |
None
|
0 |
|
|
19 |
None
|
0 |
|
|
20 |
Conduct, Non-Aggressive
|
1 |
|
|
21 |
None
|
0 |
|
|
22 |
None
|
0 |
|
|
23 |
Conduct, Non-Aggressive Adjustment Disorder with Depressed Mood
|
2 |
|
|
24 |
None
|
0 |
|
|
25 |
None
|
0 |
|
|
26 |
None
|
0 |
|
|
27 |
None
|
0 |
|
|
28 |
Overanxious Disorder
|
1 |
|
|
29 |
Conduct, Aggressive
|
1 |
|
|
30 |
None
|
0 |
|
|
31 |
Conduct, Non-Aggressive Adjustment Disorder with Depressed Mood
|
2 |
Multiple suicide attempts |
|
32 |
None
|
0 |
|
|
33 |
None
|
0 |
|
|
34 |
None
|
0 |
|
|
35 |
None
|
0 |
|
|
36 |
None
|
0 |
|
|
37 |
Conduct, Aggressive Major Depression |
2 |
1 suicide attempt (prescription medication)
|
|
38 |
Overanxious Disorder |
1
|
|
|
39 |
Marijuana Abuse Adjustment Disorder with Depressed Mood |
2 |
2 suicide attempts
|
|
40 |
Adjustment Disorder with Depressed Mood Overanxious Disorder |
2 |
Medications: Prozac and Zoloft
|
|
41 |
Adjustment Disorder with Depressed Mood |
1 |
2 suicide attempts
|
|
42 |
Conduct, Non-Aggressive
|
1 |
|
|
43 |
None |
0 |
Sub-threshold for Major Depression
|
|
44 |
Overanxious Disorder |
1 |
Sub-threshold for Major Depression
|
|
45 |
Conduct, Non-Aggressive Conduct, Aggressive Alcohol Abuse Marijuana Abuse Other Drug Abuse (Cocaine) Adjustment
Disorder with Depressed Mood
|
7 |
Medication: Paxil, Zanax |
|
46 |
Adjustment Disorder with Depressed Mood |
1 |
|
|
47 |
Oppositional Disorder Adjustment Disorder with Depressed Mood |
2 |
Sub-threshold for Alcohol Abuse; was on anti-depressant medication; 2 suicide attempts
|
|
48 |
Oppositional Disorder |
1 |
|
|
49 |
Adjustment Disorder with Depressed Mood Overanxious Disorder
|
2 |
|
|
50 |
None
|
0 |
|
|
51 |
Major Depression Overanxious Disorder
|
2 |
Medication: Paxil |
|
52 |
Conduct, Non-Aggressive Alcohol Abuse Marijuana Abuse Other Drug Abuse (Ketamine, Ecstasy) Other Drug Dependence (Ketamine, Ecstasy) Major Depression Overanxious Disorder
|
7 |
|
|
53 |
None
|
0 |
|
|
54 |
None
|
0 |
|
|
55 |
Oppositional Defiant Disorder |
1 |
Sub-threshold for major depression
|
|
56 |
None |
0 |
|
|
|
|
|
|
|
57 |
Conduct, Aggressive Conduct, Non-Aggressive Other Drug Abuse (Esctacy) Adjustment Disorder with Depressed Mood |
4 |
Medications: Wellbutrin and Celexa; 1 suicide attempt
|
|
58 |
Overanxious Disorder |
1 |
Was on Prozac
|
|
59 |
Alcohol Abuse Alcohol Dependence Marijuana Abuse Other Drug Abuse (Hallucinogens) Other Drug Dependence (Hallucinogens) Adjustment Disorder with Depressed Mood Overanxious Disorder
|
7 |
1 suicide attempt |
|
60 |
Conduct, Non-Aggressive
|
1 |
|
|
61 |
None
|
0 |
|
|
62 |
Major Depression Overanxious Disorder
|
2 |
Medication: Zoloft |
|
63 |
Oppositional Disorder Marijuana Abuse
|
2 |
Prozac |
|
64 |
None |
0 |
|
|
Diagnostic Interview Schedule Diagnoses at Follow-up |
|||
|
ID |
Diagnosis(es) |
No. of Diagnoses |
Clinical Comments |
|
1 |
None
|
0 |
|
|
2 |
None
|
0 |
|
|
3 |
None
|
0 |
Medication: Effexor |
|
4 |
None
|
0 |
|
|
5 |
None
|
0 |
On medication for ADHD
|
|
6 |
None |
0 |
Sub-threshold for Drug Abuse (Marijuana, Cocaine) and Drug Dependence
|
|
7 |
None |
0 |
|
|
8 |
Drug Dependence (Amphetamines) |
1 |
|
|
9 |
Alcohol Abuse |
1 |
|
|
10 |
Alcohol Abuse |
1 |
|
|
11 |
Major Depression, Single Episode |
1 |
|
|
12 |
Alcohol Abuse |
1 |
Sub-threshold for Major Depression
|
|
13 |
Major Depression, Recurrent |
1 |
|
|
14 |
Major Depression, Recurrent |
1 |
1 suicide attempt
|
|
15 |
Simple Phobia |
1 |
Sub-threshold for Drug Abuse and Dependence
|
|
16 |
Major Depression, Recurrent |
1 |
Sub-threshold for Bulimia
|
|
17 |
Major Depression, Single Episode
|
1 |
Sub-threshold for Drug Abuse (Marijuana)
|
|
18 |
Major Depression, Recurrent Alcohol Dependence |
2 |
|
|
19 |
Alcohol Abuse Alcohol Dependence |
2 |
Sub-threshold for Major Depression; attempted suicide
|
|
20 |
Obsessive Compulsive Disorder Simple Phobia (exclusion not met) |
2 |
|
|
21 |
Major Depression, Single Episode Alcohol Abuse
|
2 |
|
|
22 |
Social Phobia Generalized Anxiety
|
2 |
|
|
23 |
Major Depression, Single Episode Generalized Anxiety (exclusion not met)
|
2 |
|
|
24 |
Dysthymic Disorder Alcohol Abuse Alcohol Dependence
|
3 |
|
|
25 |
Major Depression, Single Episode Social Phobia (exclusion not met) Panic Disorder (exclusion not met) |
3 |
Sub-threshold for Alcohol Dependence and Drug Abuse (Marijuana); hypomanic episodes in preceding year; taking Celexa
|
|
26 |
Major Depression, Recurrent Obsessive Compulsive Disorder (exclusion not met) Social Phobia (exclusion not met) Generalized Anxiety Disorder (exclusion not met)
|
4 |
On medication for anxiety |
|
27 |
Major Depression, Recurrent Alcohol Abuse Social Phobia (exclusion not met) Panic Disorder (exclusion not met)
|
4 |
Sub-threshold for Drug Dependence |
|
28 |
Major Depression, Recurrent Alcohol Abuse Alcohol Dependence Generalized Anxiety (exclusion not met)
|
4 |
Sub-threshold for Drug Dependence (Marijuana) |
|
29 |
Major Depression, Recurrent Alcohol Abuse Drug Abuse (Marijuana, Ecstasy, Cocaine) Drug Dependence (Marijuana, Ecstasy, Cocaine)
|
4 |
Took antidepressants; 1suicide attempt |
|
30 |
Major Depression (Recurrent) Agoraphobia (exclusion not met) Social Phobia (exclusion not met) Generalized Anxiety (exclusion not met)
|
4 |
1 suicide attempt |
|
31 |
Major Depression, Recurrent Simple Phobia Agoraphobia (exclusion not met) Social Phobia (exclusion not met)
|
4 |
On antidepressants |
|
32 |
Mania (Bipolar) Drug Abuse (Cocaine, Opiates) Drug Dependence (Cocaine, Opiates) Simple Phobia Generalized Anxiety
|
5 |
|
|
33 |
Major Depression, Recurrent Drug Abuse (Marijuana) Drug
Dependence (Marijuana) Generalized anxiety (exclusion not met)
|
5 |
|
|
34 |
Major Depression, Recurrent Alcohol Abuse Alcohol Dependence Dysthymic Disorder (exclusion not met) Generalized Anxiety (exclusion not met)
|
5 |
|
|
35 |
Major Depression, Recurrent Alcohol Abuse Drug Dependence (Marijuana) Obsessive Compulsive Disorder (exclusion not met) Generalized Anxiety (exclusion not met)
|
5 |
Took antidepressants |
|
36 |
Major Depression, Recurrent Alcohol Abuse Drug Abuse (Marijuana, Cocaine, Ecstasy Drug Dependence (Marijuana, Cocaine, Ecstasy) Simple Phobia |
5 |
Medications: Celexa, Ritalin; arrested and then hospitalized once for uttering death threats to mother
|
|
37 |
Major Depression, Recurrent Alcohol Abuse Alcohol Dependence Drug Abuse (Marijuana, Cocaine, Amphetamines) Drug Dependence (Marijuana, Cocaine, Amphetamines) |
5 |
|
|
38 |
Major Depression, Single Episode Dysthymic Disorder (exclusion not met) Social Phobia (exclusion not met) Agoraphobia with Panic Attacks (exclusion not met) Generalized Anxiety (exclusion not met) |
5 |
1 suicide attempt |
|
39 |
Major Depression, Recurrent Simple Phobia Agoraphobia (exclusion not met) Social Phobia (exclusion not met) Generalized Anxiety (exclusion not met) |
5 |
|
|
40 |
Major Depression, Recurrent Drug Abuse (Marijuana, Ecstasy, Ketamine) Drug Dependence (Marijuana, Ecstacy) Simple Phobia Social Phobia (exclusion not met) Agoraphobia with Panic Attacks (exclusion not met)
|
6 |
Was on anti-depressant medication (Zoloft); 1 suicide attempt |
|
41 |
Major Depression, Recurrent Drug Abuse (Marijuana) Drug Dependence (Marijuana) Panic Disorder (exclusion not met) Generalized Anxiety (exclusion not met) Bulimia (exclusion not met) |
6 |
Medication: Cipralex |
|
42 |
Mania (Bipolar) Alcohol Abuse Bulimia Dysthymic Disorder (exclusion not met) Obsessive-Compulsive Disorder (exclusion not met) Agoraphobia with Panic Attacks (exclusion not met) Generalized Anxiety (exclusion not met) |
7 |
Sub-threshold for Drug Abuse and Dependence; attempted suicide |
|
43 |
Major Depression, Recurrent Alcohol Abuse Alcohol Dependence Dysthymic Disorder (exclusion not met) Obsessive Compulsive Disorder (exclusion not met) Simple Phobia (exclusion not met) Panic Disorder (exclusion not met) Generalized Anxiety (exclusion not met) |
8 |
Medications: Lorazepam, Paxil, Wellbutrin |
|
44 |
Major Depression, Recurrent Alcohol Abuse Drug Abuse (Ketamine) Drug Dependence (Cocaine, Ketamine) Simple
Phobia Dysthymic Disorder (exclusion not met) Panic Disorder (exclusion not met) Generalized Anxiety (exclusion not met) |
9 |
Medication: Effexor; diagnosed with AIDS |
Appendix M
Gender Identity and Sexual Orientation Outcomes in Follow-up Studies of Boys with GID
|
|
|||||
|
Gender Identity and Sexual Orientation in other Follow-up Studies of Boys with GID |
|||||
|
|
|
Sexual Orientation in Fantasy |
Sexual Orientation in Behavior |
||
|
|
Persistence of Gender Dysphoria (% ) |
Heterosexual
(%) |
Homosexual/ Bisexual (%) |
Heterosexual
(%) |
Homosexual/ Bisexual (%) |
|
Six studies summarized by Zucker & Bradley (1995)a |
9.1 (n = 5) |
- |
- |
- |
- |
|
|
|
|
|
|
|
|
Green (1987) |
2.3 (n = 1) |
25 (n = 11) |
75 (n = 33) |
20 (n = 6) |
80 (n = 24) |
|
|
|
|
|
|
|
|
Wallien & Cohen-Kettenis (2008) |
20.3% or 30%b (n = 12) |
19c (n = 4) |
81 (n = 17) |
21d (n = 4) |
79 (n = 15) |
|
|
|
|
|
|
|
|
Singh (2012) (Present Study) |
12.2 (n = 17) |
33.3 (n = 43) |
63.6 (n = 82) |
26.9 (n=29) |
47.2 (n = 51) |
|
aThe sexual orientation results for these six studies (taken collectively due to the same sample size of the individual studies) are not reported here because it was unclear whether sexual orientation was measured according to fantasy or behavior. bThis percentage reflects the persistence rate for only the males in the study. Two rates were obtained depending on the sample used to calculate the persistence rate. The conservative rate of 30% was obtained when persistence was calculated using only those boys who were successfully traced at follow-up were included in the study. The persistence rate of 20.3% was obtained using a liberal criterion whereby the boys who could not be traced and who were assumed to be desisters were included in the study. cData on sexual orientation in fantasy were available for 21 of the 40 males who completed the follow-up assessment. dData on sexual orientation in behavior were available for 19 of the 40 males who completed the follow-up assessment. |
|||||
[1] However, individuals who complete sex reassignment challenge this conceptualization of gender identity. These individuals alter surface attributes of gender, such as hair and clothing, as part of their gender role change.
[2] Items are scored based on the past 6 months on a 0-2 scale where 0 = not true, 1 = somewhat or sometimes true, and 2 = very true or often true.
[3] “Feminine” is stated here with quotations to reflect the name Green (1987) assigned to this group of boys.
[4] The comparison group was matched on a number of variables, including age, number, age, and sex of siblings, marital status of parents, and education level of parents (Green, 1987).
[5] GID as a diagnostic category had not yet been introduced to the DSM at the time when Green (1987) began data collection.
[6] This recalculation was done by me for the purpose of this chapter.
[7] This recalculation of persistence rates for boys only was done by me for the purpose of this chapter and to allow for comparison to the persistence rates for boys with GID obtained in the present study and by Green (1987). These rates were not explicitly reported by Wallien and Cohen-Kettenis (2008).
[8] Drummond et al. (2008) reported on the long-term outcome of 25 biological females with GID assessed in childhood (mean age, 8.88 years) at the Child and Adolescent Gender Identity Service at CAMH. Drummond et al. reported a persistence rate of 12%; 3 of the 25 girls were gender dysphoric at follow-up (mean age, 23.24).
[9]Wallien and Cohen-Kettenis (2008) compared their outcomes groups on childhood measures of sex-typed behavior, but not on childhood demographic variables or childhood behavioral problems. Group comparison on childhood GID diagnosis was done using chi-square analyses. Group comparison on the Gender Identity Interview and Gender Identity Questionnaire for Children were done using t-tests.
[10] The Gender Identity Interview and Gender Identity Questionnaire for Children were developed in the Gender Identity Service at the Centre for Addiction and Mental Heath in Toronto.
[11] Across all studies, sexual orientation is classified in relation to birth sex.
[12] For the desisters, data on sexual orientation in fantasy and behavior were available for only 16 and 13 participants, respectively. For persisters, data on sexual orientation in fantasy and behavior were available for only 5 and 6 participants, respectively. Wallien and Cohen-Kettenis (2008) did not explain these missing data.
[13] Included studies and case reports.
[14] Pairs were matched as closely as possible to age, IQ, parents’ social class, and parents’ marital status.
[15] During this wave of systematic data collection, there was a relatively greater focus on recruitment during 2009 compared to 2010. In 2010, recruitment occurred primarily during the first 6 months of the year. Thus, a larger number of participants were assessed in 2009 compared to 2010.
[16]Using t-tests, the 107 participants who entered the study through routine research contact were compared to the 32 participants who were recruited into the study after they had re-contacted the clinic for clinical reasons on childhood demographic variables (age at assessment, IQ, social class, marital status, ethnicity), CBCL behavior problems in childhood (Internalizing T score, Externalizing T score, Total T score), and nine measures of childhood sex-typed behavior. There were no significant differences between the two groups on the demographic variables of age at assessment, social class, ethnicity or marital status (ps > .05). The comparison on childhood IQ approached significance, t(137) = 1.97, p = .051, with the routine research entry participants having, on average, a higher IQ than the clinical entry participants. On the CBCL, there was a significant difference on Internalizing problems only, t(137) = -2.02, p = .046, with the clinical entry participants rated by their parents as having more internalizing problems compared to the research entry participants. Of the nine measures of childhood sex-typed behavior, the two groups differed significantly on three: (1) free play, t(119) = -2.11, p = .037, (2) Gender Identity Interview, t(83) = -2.09, p = .04, and (3) Gender Identity Questionnaire for Children, t(95) = 2.39, p = .019, with the clinical entry participants having, on average, more childhood cross-gender behavior than the research entry participants. Of the 32 clinical entry participants, 8 had re-contacted the clinic because of gender dysphoria. The above described comparisons were repeated to compare the research and clinical entry participants but with these 8 participants excluded. With the 8 participants who contacted the clinic for gender dysphoria removed, there were no significant group differences on demographic variables, CBCL behavior problems, and measures of childhood sex-typed behavior (all ps > .05).
[17]Correlation among subtests scores, index, scores and full scale IQ across versions of the WISC ranges from medium to high (Wechsler, 2003).
[18] Absolute range on the GIQAA is 1-5, with a lower score reflecting more gender dysphoria.
[19] The Kinsey Scale: 0 = Exclusively heterosexual, 1 = Predominantly heterosexual, only incidentally homosexual 2 = Predominantly heterosexual but more than incidentally homosexual, 3 = Equally homosexual and homosexual, 4 = Predominantly homosexual, but more than incidentally heterosexual, 5 = Predominantly homosexual, but incidentally heterosexual, and 6 = Exclusively homosexual (Kinsey et al. 1948).
[20] IQ data were missing for 11 of the 163 boys who were eligible for the study but were not contacted.
[21]For some participants who did not complete the face-to-face assessment, data on sexual orientation were available. In these cases, participants were assigned a Kinsey fantasy rating of 0 for heterosexual sexual orientation and 6 for homosexual sexual orientation.
[22] Given the strong correlation between Kinsey fantasy and behavior ratings and that there were less missing data on the Kinsey fantasy variable, participants were classified into one of four outcome groups based on their fantasy ratings. Measuring sexual orientation on the basis of fantasy is methodologically more robust than measuring sexual orientation on the basis of sexual behavior. A person’s sexual behavior may be influenced by many factors other than sexual fantasy or sexual feelings, such as moral sense and availability of a sexual partner (LeVay, 2011) and, in general, may be more variable than erotic feelings (Harry, 1985a).
[23] The ANCOVA model was adjusted to accommodate a categorical covariate.
[24] Although the groups did not differ significantly on cross-sex toy preference on the PPPSI, this measure is included here because there was a trend in the direction of a significant group difference.
[25] For some participants, data were not available on all six measures. In these cases, the composite score was the average of the number of variables for which there were data.
[26] A preliminary analysis with marital status included as a predictor variable showed that this variable did not have a significant effect and was, therefore, excluded in the final regression model.
[27] I did not perform correlation analyses between peer relations and Internalizing and Externalizing T score because the three items from the Peer Relations Scale loaded on at least one of the broad-band factors and it would have been too cumbersome to re-score all the CBCLs with these items removed.
[28] The ANCOVA model was adjusted to accommodate a categorical covariate.
[29] This is a proportion score which represents participants’ scores on the GIQAA or the GDQ, depending on which measure was administered.
[30] Absolute range on the GIQAA is 1-5, with a lower score reflecting more gender dysphoria.
[31]In one case, although the participant (in Group 1) did not endorse significant gender dysphoria on the Gender Identity Questionnaire for Adolescents and Adults, he was classified as a persister because subsequent follow-up information provided by the participant himself at later dates indicated that he was, in fact, struggling with his gender identity. Regrettably, the Gender Identity Questionnaire for Adolescents and Adults was not re-administered to him. In the second case, the participant was the only heterosexual desister (Group 4).
[32] The males in Singh et al. (2010) were significantly older than the participants in the present study.
[33] These analyses were repeated using partial correlations in which age at assessment, age at follow-up, and follow-up interval were controlled for. The pattern of significant findings did not change.
[34] The ANCOVA model was adjusted to accommodate a categorical covariate.
[35] The ANCOVA model was adjusted to accommodate a categorical covariate.
[36] The ANCOVA model was adjusted to accommodate a categorical covariate.
[37]Group means for number of suicide attempts since the age of 13: Bisexual/homosexual persisters (M = 1.43, SD = .53); bisexual/homosexual desisters (M = 1.43; SD = .73); heterosexual desisters (M = 1.10, SD = .32).
[38] Since the purpose of this analysis was to examine if there was a significant difference between the groups on whether suicidal thinking was endorsed or not, participants’ response on Items 18 and 91 were recoded dichotomously where 0 indicated that the item was not endorsed and 1 indicated that the item was endorsed.
[39] Age range, 15-18.
[40] Age range, 18-59.
[41] Age range, 15-18.
[42] Age range, 18-59.
[43] For the participants who experienced victimization, they were bullied in regard to their gender role behaviors and being effeminate, rather than about their gender identity per se.
[44] Since the YSR/ASR instructs participants to complete ratings based on the past 6 months and is, therefore, a reflection of current behavior problems, the mean overall victimization score for the past 12 months was used instead of lifetime (since the age of 13 years) victimization score.
[45] For the chi-square analysis, Wallien and Cohen-Kettenis’ conservative persistence rate of 30% (i.e., calculated using only the 40 boys who were successfully traced a follow-up) was used. However, the chi-square analysis can also be conducted using the liberal persistence rate of 20.3%. Using this method, the difference in persistence rates across the three studies remained significant, χ2(2) = 7.58, p = .02.
[46] In the present study, 19% of the potential participants could not be traced/contacted. The corresponding percentages of untraced participants in Drummond et al. (2008) and Wallien and Cohen-Kettenis (2008) were 8% and 30%, respectively.
[47] The persistence rate in the present study was almost identical to that obtained by Drummond et al. (2008)(12%) in their follow-up study of girls with GID.
[48] Although participants were interviewed about sexual fantasies and sexual behaviors, sexual orientation classification was based on their reported fantasies. The rationale for this approach was provided in the Results chapter.
[49] “Coming out” is the process of sexual orientation identity development for gay, lesbian, and bisexual individuals and is sometimes used synonymously with the disclosure of sexual identity to others (e.g., Heatherington & Lavner, 2008). While there is individual variation, stage theories suggest that the process generally begins with awareness of same-sex attraction, followed by same-sex, and sometimes opposite-sex, sexual experience and gradual acceptance and integration of a gay/lesbian/bisexual identity. Coming out is generally thought to culminate with disclosure (Floyd & Bakeman, 2006; Martin, 1991; McDonald, 1982).
[50] For analyses, only three of the four outcome groups (bisexual/homosexual persisters, bisexual/homosexual desisters, and heterosexual desisters) were compared. The heterosexual persister was excluded from the group analyses.
[51] Predictor variables were age at childhood assessment, Full Scale IQ in childhood, social class, and marital status.
[52] In the context of strong negative attitudes towards homosexuality, some might view a transsexual outcome as more favorable than a homosexual one because, in living as a woman, these individuals would typically self-label as heterosexual rather than as homosexual to reflect their female gender identity.
[53] The measures were the Gender Identity Questionnaire for Children and the Gender Identity Interview, both of which were developed in the Toronto gender identity clinic.
[54] Predictor variables were age at childhood assessment, Full Scale IQ in childhood, social class, and composite z-score of childhood sex-typed behavior.
[55] In the present follow-up sample, the presence of a PDD was not assessed at follow-up as the semi-structured diagnostic interviews did not include a module to assess for PDD.
[56] Wallien and Cohen-Kettenis (2008) reported that 9 of the 14 girls who were successfully traced at follow-up were gender dysphoric and the remaining 5 girls were desisters, which yielded a persistence rate of 64.2%. However, an additional 4 girls could not be traced at follow-up and were assumed by Wallien and Cohen-Kettenis to be desisters. When these participants were included in the calculation of a more liberal persistence rate, persistence dropped to 50%. Regardless of whether one uses the liberal or more conservative persistence rate, the rates obtained by Wallien and Cohen-Kettenis were substantially higher than the 12% persistence rate obtained by Drummond et al. (2008).
[57] Wallien and Cohen-Kettenis (2008) did not publish overall sample means and standard deviation on these measures, therefore precluding direct comparison to the boys in the present study.
[58] To clarify, Wallien and Cohen-Kettenis’ research was conducted at the specialized gender identity clinic in Amsterdam, which I sometimes refer to as the Dutch or Amsterdam clinic.
[59] Sexually attracted to biological males.
[60] In other follow-up studies of boys with GID, the number of persisters was small; therefore, variability would not be expected. The lone persister in Green’s (1987) study desired sex-reassignment surgery. In the six follow-up studies summarized by Zucker and Bradley (1995), 2 of the 5 individuals described as having a “transsexual” outcome were taking cross-sex hormones and 1 had completed sex-reassignment surgery. In the remaining two cases, details on degree of transitioning were not provided.
[61] Predictor variables were age at childhood assessment, Full Scale IQ in childhood, social class, and a composite measure of childhood sex-typed behavior.
[62] Recent studies using community samples of youth suggest that rates of self-harm behaviors, including non-suicidal self-injurious behaviors, is a growing health concern and may be higher than rates of suicidal ideation and attempt (e.g., Jacobson & Gould, 2007). Growing concern about the high rates of self-harm behaviors among youth had led DSM-5 work groups to consider the possibility of defining non-suicidal self-injury as a distinct syndrome (Glenn & Klonsky, 2010). In the present study, suicidal behavior and self-harm were not measured as separate constructs and, therefore, may represent a limitation. However, one goal of the study was to obtain general outcomes with regard to suicidality, defined broadly to include self-harm behaviors. Future studies would be needed to determine if there are unique risks for suicidal behavior and non-suicidal self-harm within this population and whether different psychosexual outcomes are associated with different risks for suicidality vs. non-suicidal self-harm behaviors.
[63] Kirk was given the pseudonym “Kraig” in Rekers and Lovaas’ (1974) treatment report. He was referred to as “Kyle” in Green (1987).
[64] It is unclear whether the participants in the study were pre sex reassignment surgery, post sex reassignment surgery, or a combination of both.
[65] Note. American Psychiatric Assocation. (2011). DSM-5 development. Retrieved from www.dsm5.org/ProposedRevision/Pages/proposedrevision.aspx?rid=192. Proposed criteria as of May 4, 2011.
[66] For potential participants who were last seen when they were over the age of 16, they will be contacted directly and the script modified accordingly.